49. Genioplasty
Relevant Anatomy
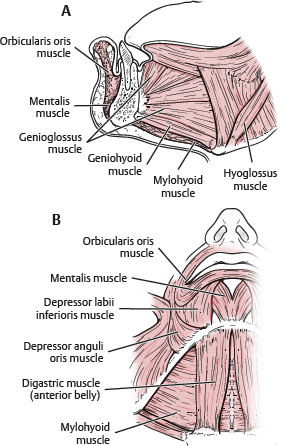
Muscles
Mentalis
Conelike, vertical fibers from incisive fossa to overlying skin
Can cause wrinkling, and if hyperdynamic, may be visible under lower lip
Midline void between fibers seen when chin dimple present
Orbicularis oris (lower fibers)
Depressor anguli oris
Quadratus (depressor) labii inferioris
Geniohyoid, genioglossus, mylohyoid, and anterior belly of digastric
Attach to lingual (posterior) aspect of chin
Bony Landmarks
Mental foramen
Digastric fossa
Mental protuberance
Mental spines
Submandibular fossa
Nerve Supply
Inferior alveolar nerve and mental nerve (terminating branch exiting mental foramen)
Mental nerve: Located at base of first or second bicuspid
Inferior alveolar nerve
Risk of injury during genioplasty procedures
Osteotomies should be 5-6 mm below mental foramen to prevent injury to nerve branches or tooth apices.
Note:
The inferior alveolar nerve can be absent or distorted in patients with hemifacial microsomia or other facial deformities.
Blood Supply
Labial branch (dominant supply) of facial artery
Inferior alveolar artery
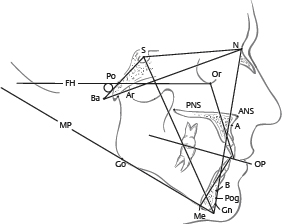
Significant Cephalometric Points
Pogonion (Pog): Most projecting portion of mandible. Denotes chin excess or deficiency in relation to other structures (i.e., nasion and lip position)
Menton (Me): Lowest (most caudal) portion of chin
Subspinale (A): Columellar-labial junction
Supramentale (B): Deepest point between pogonion and incisor
Nasion (N): Nasofrontal junction
Indications and Contraindications
Osseous Genioplasty
Indications
Horizontal asymmetries of any magnitude
Excess deficiency or excess in both vertical and sagittal planes
Moderate to severe microgenia
Secondary cases after osseous or alloplastic genioplasty
Adjunct to formal orthognathic surgery
Alloplastic genioplasty is rarely, if ever, combined with formal orthognathic lower or upper jaw surgery.
Contraindications
Inadequate bone stock (i.e., elderly patients, bone pathology)
Abnormal dentition or significant dental pathology
Patient preference to not have osteotomy
Contrary to common belief, can be a relatively simple and efficient procedure
More versatile procedure versus alloplastic augmentation
Allows multidimensional chin correction, including reduction
Alloplastic Augmentation
Indications
Mild isolated sagittal deficiencies
Need to increase only the labiomental fold depth
Relative: Concomitant necklift/facelift
Easily facilitates alloplastic augmentation as a concomitant procedure
Contraindication
Excess horizontal deficiency
Any vertical deficiency
Mandibular asymmetry
Secondary cases with bony erosion
Malocclusion: Orthognathic surgery required
Tip:
Generally, alloplastic augmentation should be used only in patients with mild to moderate chin deficiency in the sagittal plane and a shallow labiomental fold. 1 – 4
Caveat: Aesthetic surgery patients seem to prefer alloplastic augmentation, and tend to shy away from osteotomies.
Facelift/necklift procedures often include a submental incision that can easily be used for placing a chin implant.
Popular media has shown a bias toward alloplastic augmentation and present any “cuts in the bone” as very “invasive.”
Malocclusion requires consideration of orthognathic surgery and a more extensive workup (cephalometric analysis, occlusion models) and possible collaboration with an oromaxillofacial surgeon.
Significant microgenia usually requires an osseous genioplasty, because a very large implant can appear awkward.
Preoperative Evaluation
Medical comorbidities
Diabetic and immunosuppressed patients: Not good candidates for alloplastic chin implantation
Osteotomy site(s) may heal poorly.
Age: Higher-age patients may have osteopenic bone—not good candidates for osseous genioplasty
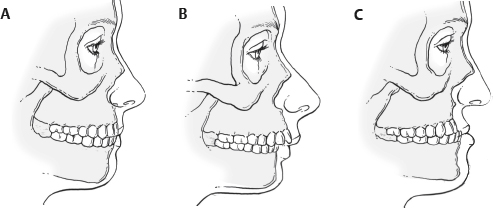
Occlusion type (Fig. 49-3)
Normal occlusion (Angle class I)
Mesiobuccal cusp of maxillary first molar occludes into the buccal groove of the mandibular first molar (Fig. 49-3, A).
Angle class II malocclusion
Mesiobuccal cusp of maxillary first molar occludes medial to the buccal groove (Fig. 49-3, B).
Most common malocclusion in North American whites.
Class II is often an indication for further evaluation and possibly orthognathic surgery with maxillary and mandibular osteotomies.
Angle class III malocclusion
Mesiobuccal cusp of the maxillary first molar occludes distal to the buccal groove of the mandibular first molar (Fig. 49-3, C).
Tip:
Obtaining previous orthodontic history is important; because occlusion may have been corrected without addressing maxillary and mandibular disharmonies (deformity becomes masked).
Dentition
Before 15 years of age, permanent dentition may not be fully erupted.
Greater risk of injury during osteotomies
Elderly patients may have retruded alveolar ridge (if edentulous), which contributes to chin pad ptosis.
Presence of little bone stock
May be better candidates for alloplastic augmentation
Patients with poor dentition or infected dentition are very poor candidates for any form of genioplasty until fully treated.
Life-Size Photographs
Bilateral sagittal view, frontal views, and bilateral oblique (three-quarter) views
Midface Height
Vertical maxillary excess: Especially important when accompanied by a deep labiomental fold
Patient better served by formal orthognathic correction, with or without a genioplasty
Nose-Chin-Lip Evaluation
Nasofacial harmony is linked with chin dimensions and vice versa.
Chin projection should be 3 mm posterior to nose-lip-chin plane (NLCP). 5
Nasal length: Two thirds of midfacial height and exactly equal to chin vertical length 5
Symmetry of Lower Third of Face
Right-to-left asymmetries of the mandible and chin may require multiple osteotomy configurations to centralize chin or canting of the osteotomy line and differential plate bending.
Difficult to correct with alloplastic augmentation alone
Soft Tissue Analysis
Soft tissue pad: Normally 9-11 mm thick
Palpated at pogonion and off midline with patient in repose and then when smiling
Soft tissue contribution can predict effects of augmentation.
Stomion: Junction between upper and lower lip in repose
Upper/lower lips: Lower lip eversion from deep bite, excess lip bulk, or excess overjet may deepen labiomental fold. 4
Labiomental fold
Indentation or crease between lower lip and lowest point of mandible (menton) best seen on sagittal view
Fold aesthetics dependent on vertical proportion of mandible and facial length 3
Example: Deep fold may look good on longer faces. 3
Evaluate for height (when stomion-to-menton is divided into thirds, fold often falls at junction of upper and middle third).
If fold is too low, augmentation may only address chin pad. 4
Depth
Fold depth approximately 6 mm in men and 4 mm in women 6
If deep, horizontal vector, chin augmentation may result in an awkward exaggerated deep fold and an overprojected chin
If shallow, may be further effaced by vertical augmentation
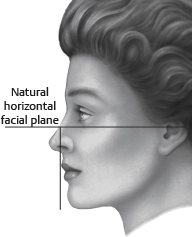
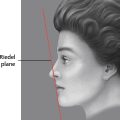
Riedel line: A line drawn vertically down facial plane on sagittal view, tangential to anterior upper and lower lip (Fig. 49-5)
Lower lip should be 2-3 mm posterior to upper lip projection.
Pogonion should never project beyond this line and should be slightly posterior to it (or just touching it).

Senior Author Tip:
The simplest and most useful means for assessing the chin projection disharmony is Riedel line, which connects the upper to the lowermost projected points and should touch the pogonion.
Dynamic and Static Chin Pad Analysis
A thin chin pad on smiling: Potential for increased pad effacement with increased bony prominence (i.e., native or from augmentation)
Burr reduction or osteotomy setback may be required.
A thick pad may increase submental soft tissue fullness and worsen the cervicomental angle if bony setback performed
Witch’s-Chin Deformity
Definition: Ptosis of soft tissue caudal to menton and an exaggerated submental crease
Correction requires soft tissue/muscle resection and/or repositioning.
Augmentation can exaggerate deformity.
Tip:
Mentalis muscle fixation superiorly is critical to preventing any soft tissue descent. Secondary cases may require soft tissue fixation with a Mitek device (DePuy Synthes) to prevent ptosis recurrence. 7
Related posts:




Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


