46. Secondary Rhinoplasty
Indications
Postoperative Functional or Aesthetic Deformity
Poor preoperative diagnosis
Failure to properly identify the structural problem resulting in functional compromise or aesthetic imbalance 1
Inappropriate surgical planning or inadequate technique resulting in distortion of supporting osteocartilaginous framework
Problematic wound healing
Prolonged edema, ecchymosis, unfavorable scarring, obstructive or restrictive webbing, and occasionally hyperesthesia
Patient Dissatisfaction
Undesirable functional or aesthetic outcome
Breathing difficulties and asymmetry are most common complaints. 2
Inadequate preoperative counseling with regard to postoperative course, recovery time, desired and expected outcomes
Unrealistic expectations
Even with appropriate preoperative counseling, some patients continue to have unrealistic expectations
If not identified, these patients will be dissatisfied with their results regardless of the outcome. 3 , 4
Postoperative deformity and patient dissatisfaction do not always correlate.
Most Common Deformities or Problems
Displacement/deviation of anatomic structures
Underresection by overly cautious surgeons
Overresection by overly aggressive surgeons 5
Contour irregularities secondary to disruption of framework or unfavorable scarring
Prosthetic complications including infection, extrusion, inflammation, palpability, or transillumination (e.g., in dorsal silicone implants)
Surgical Obstacles
Scarring of the subcutaneous tissues resulting in adherence to the underlying cartilaginous framework and destruction of tissue planes
Osteocartilaginous distortion or damage requiring reconstruction for structural support
Limited sources of cartilage grafts secondary to previous harvest of septal or conchal cartilage
Changes in Skin Thickness
Thin skin in some patients, which is less forgiving of minor underlying deformities
Prone to graft extrusion
Thick skin secondary to prolonged edema or scarring, which is less malleable and will not show desired framework changes as easily
Compromised vascularity secondary to previous surgical incisions and scarring
Surgical Approaches
Endonasal/Closed Approach
Pros
Decreased postoperative edema and scarring because limited dissection
Indications
Isolated deformities that can be addressed independent of the overall framework
Severely scarred nose where vascularity is a significant concern
External/Open Approach
This is the preferred approach for secondary rhinoplasty. 7
Pros
Provides maximal exposure for adequate visualization
Facilitates complete release of tissue attachments causing anatomic distortion
Facilitates precise diagnosis and correction of deformities under direct visualization
Allows direct hemostatic control
Cons
Increased postoperative edema
Placement of transcolumellar incision
If original scar is well hidden but at incorrect level of columella, ignore original scar and place second incision at appropriate location
Preoperative Assessment and Planning
This is supplementary to the evaluation performed for a primary rhinoplasty, as presented in Chapter 45.
Medical History
All previous nasal surgeries
Obtain previous operative reports if possible to determine graft availability, presence of prosthetic material or hardware, and previous techniques or findings that may assist in evaluation and operative planning.
History of trauma
Allergies
Cocaine/drug use
Screen for body dysmorphic disorder (BDD) (see Chapter 1)
Mental disorder involving a distorted body image, defined as:
Preoccupation with an imagined physical deformity OR
Vastly exaggerated concern of a minimal physical deformity
In 50% of patients with BDD, the nose is the primary complaint. 8 , 9
BDD occurs in secondary rhinoplasty consultations in about 12% of cases, and in 2%-7% of all primary cosmetic patient consultations. 8 , 9
Plastic surgeons are often the first to encounter these patients; thus recognizing and addressing it are essential.
A psychiatry consult may be warranted.
Senior Author Tip:
It is crucial to make sure that the secondary rhinoplasty patient’s concerns are real and match what the surgeon sees in severity. Exaggerated concerns should be carefully assessed by asking the patient to rate the flaw on the scale of 1-10, 10 being the best. Disparity in rating beyond 3-4 points should be considered a red flag.
Comprehensive Nasal and Facial Analysis
As described in the primary rhinoplasty chapter (Chapter 45), with special attention to common secondary deformities:
Bony pyramid
Excessive narrowing or convexity
Secondary to inadequate alignment or splinting of bones after osteotomy
Irregularities/stairstep deformity
Because of unplanned fracture sites
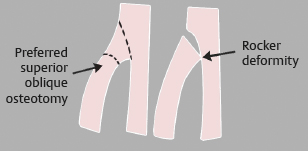
Rocker deformity (Fig. 46-1)
Occurs from inadequate placement of medial osteotomy, resulting in a wide upper dorsum
Midvault/upper lateral cartilages
Asymmetry of dorsal aesthetic lines
Nasal deviation
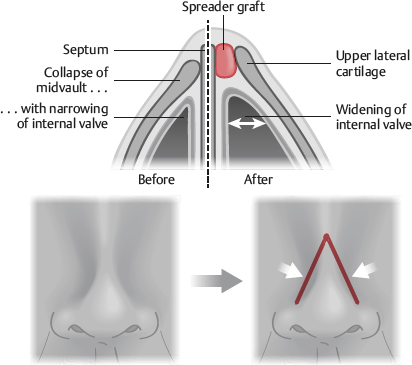
Inverted-V deformity (Fig. 46-2)
Midvault collapse leading to visibility of the the caudal edge of the nasal bones
This edge or line forms an upside down or inverted V.
Results from overresection of the dorsal midvault and upper lateral cartilages or inadequate infracture of the nasal bones
Saddle nose deformity (Fig. 46-3)
Excessively depressed upper nasal and midvault regions secondary to overresection
Supratip area
Polly beak deformity 11
Convexity located just cephalad to the nasal tip
Secondary to overresection of the noncartilaginous caudal dorsum, underresection of the cartilaginous nasal dorsum and/or excessive scar formation in the dead space of the supratip area (Fig. 46-4)
Bulbous or boxy tip deformity
Pinched nasal tip deformity
Results from collapsed alar rims after disruption of lateral crural support
Loss of tip projection
From loss of tip support: Disruption of lower lateral cartilages (LLCs) and/or intercartilaginous attachments
Overrotation
Obtuse nasolabial angle
Asymmetry of tip-defining points
Secondary to inadequate placement of tip sutures or unrecognized damage to cartilage
Infratip lobule
Excessive infratip lobule projection
From excessive length and buckling of middle crus or crura
Lack of definition
Middle crus too wide
Deformity may result from prominent caudal septum or obtuse septal angle. 14


Alae
Widened base
Alar rim collapse resulting in impaired external valve competency (Fig. 46-5)
Loss of LLC integrity and failure to reconstruct framework at initial surgery
Clinically assessed by palpating preoperative resistance of alae to gentle compressive force
Weakness is useful for diagnosing either established or predisposition to alar collapse.
Alar retraction
Alar flaring
Widened base
Notching
Secondary to inadequate placement or closure of previous incisions, scarring, and failure to place supporting grafts
Columella
Retraction, deviation, and/or inferior bowing
Intranasal

Senior Author Tip:
History of septoplasty does not necessarily mean depletion of the cartilage in the septum. A thorough examination may result in discovery of sufficient cartilage in the septum.
Related posts:




Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


