45. Rhinoplasty
Functional Role of Nose
Regulate airflow, humidification, olfaction, filtration
Nasal airway: 50% of airway resistance
Nasal cycle
Alternating constriction and dilation of nasal mucosa on each nasal side
Normal cycle is 4 hours.
Abnormalities can be present from obstruction, allergies, or vasomotor irregularities (i.e., sensitivity to heat-cold changes).
Relevant Anatomy
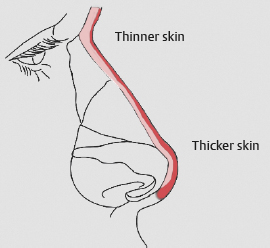
Skin
Skin thickness and sebaceousness are often underestimated components in predicting final nasal shape. 2
Skin is thickest in the lower third (tip, alae).
Skin is thinner in the upper and middle thirds, with more gliding.
Understanding the contractile properties of each patient’s nasal skin is critical to the outcome.
Modifications of the underlying bony and cartilaginous frame (particularly at the paradomal and tip regions) may be obscured by thick, poorly contractile skin.
Debulking of skin and soft tissue can be an important maneuver.
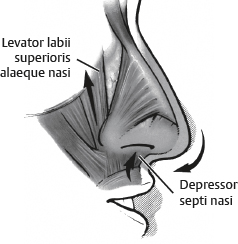
Nasal Muscles
Nasal superficial musculoaponeurotic system (SMAS)
Includes dilator nasi, transverse muscle fibers
Flares nostrils
Levator labii superioris alaeque nasi
Helps external valve to stay open
Elevates nostrils
Depressor septi nasi muscle 3 , 4
An important muscle in dynamic tip ptosis
Raises upper lip and pulls nasal tip down
Can be transpositioned or transected as part of rhinoplasty 5
Can be chemodenervated for diagnostic or treatment purposes
Blood Supply
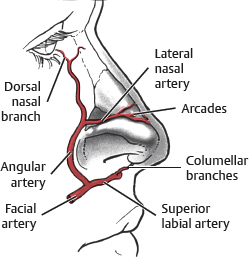
Most blood supply is located within subcutaneous plane.
Caution:
When debulking nasal soft tissue, do not violate the blood supply to the subdermal plexus.
Angular artery
Lateral nasal branch arises from this artery 2-3 mm above alar groove.
Supplies the subdermal plexus at nasal tip either unilaterally or bilaterally in 100% of cadaver specimens
Excessive defatting of skin that violates subdermal plexus can compromise vascularity of tip/columellar skin.
Note:
Stay below the alar groove during alar base resection to preserve this vessel.
Tip:
During secondary rhinoplasty, soft tissue debulking is more difficult because of scar tissue, and previously dissected nasal tip skin may be more prone to vascular compromise during dissection.
Facial artery
Branches: Superior labial artery and angular artery
Supply nasal tip via columella
Dedicated columellar branch from superior labial artery
Ophthalmic artery
Gives off the following branches: Anterior ethmoidal, dorsal nasal, and external nasal arteries to sidewalls and upper third of nose
Internal Nasal Valve
Narrowest segment of nasal airway
Two thirds of airway resistance
Angle between caudal upper lateral cartilage (ULC) and septum should be >10-15 degrees.
Length, stability, and strength of ULC are important.
External Nasal Valve
Dynamic structure: Mobile alar sidewalls and caudal septum
Alar arch, along with musculature, allows stenting effect with inspiration.
Internal nasal valve narrows while external valve opens during the negative pressure effect of inspiration.
Size, shape, strength, and orientation of lower lateral cartilage (LLC) help to determine external valve sufficiency.
External nasal valve insufficiency 1 , 6
Flaccid or weak LLC
Slitlike nostril rims (vertical/narrow: iatrogenic or inherent)
Thin alar sidewalls
Malposition of LLC (cephalically oriented)
Caudal edge of LLC is an excessive distance from nostril rim, so alar rim support is not provided during inspiration.
Tip:
External valve insufficiency is a significant contributor to postrhinoplasty airway complications. Diagnosis of potential external valve insufficiency is required, and preservation of at least a 6 mm rim strip of LLC, along with alar contour grafts and/or lateral crural strut grafts, may be necessary.
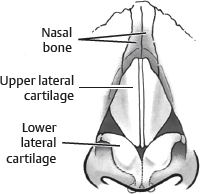
Nasal Vaults
Three nasal vaults: Bony, upper cartilaginous, and lower cartilaginous
Bony Vault
Paired nasal bones and ascending process of the maxilla
Proximal third to half of nose
Ethnic variations in length may exist.
Upper Cartilaginous Vault
Known also as nasal midvault
Paired ULCs
Underlap nasal bones 6-8 mm (keystone area)
Widest portion of nasal dorsum
Scroll area: Junction where ULCs underlap LLCs
Internal nasal valve: At junction of caudal ULC and septum
ULCs join the nasal septum at dorsum to form a T.
Affects dorsal aesthetic lines
Spreader grafts are placed at this junction.
Tip:
The “component dorsum reduction” technique helps to preserve the ULC-septal relationship through separation of the ULC from the adjacent mucoperichondrium and septum and incremental dorsal reduction. 7
Lower Cartilaginous Vault
Paired lower lateral, middle, and medial crura (cartilages)
Responsible for nasal tip shape and external valve support
Nasal Tip
Shape and position are critical in rhinoplasty.
Tripod concept: LLC and medial crura act like legs of a tripod 8 , 9 (Fig. 45-5).
Variations in length and strength of each structure influence tip position and shape.
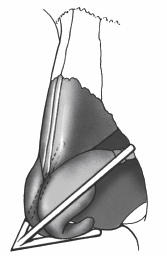
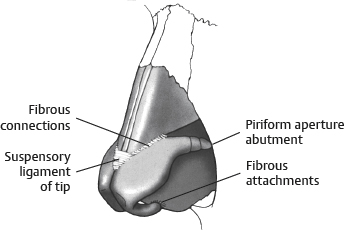
Nasal tip supported by several ligamentous attachments 9 – 11 (Fig. 45-6):
Piriform ligament: LLC abutment with piriform aperture
Domal suspensory ligament
Fibrous attachments between ULC and LLC
Medial crural ligaments
Anterior septal angle
Septum
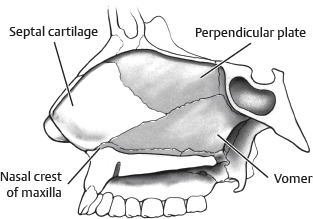
Septal cartilage, perpendicular plate of ethmoid, and vomer
Perpendicular plate of ethmoid is continuous with the cribriform plate.
Surgical or traumatic fractures of the perpendicular plate can result in CSF rhinorrhea.
Rhinoplasty fracture technique must be meticulous, gentle, and in a lateral direction to prevent cribriform injury.
Internal Nasal Valve
Formed by junction of caudal ULC and nasal septum
Normal valve angle is 10-15 degrees.
Angles <10 degrees can lead to nasal airway obstruction.
Internal nasal valve provides 50% of total airway resistance.
True spreader grafts and autospreader flaps function through increasing the internal nasal valve angle.
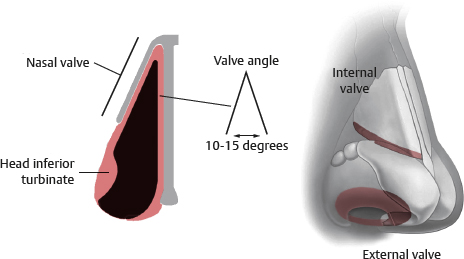
External Nasal Valve
Formed by caudal edge of LLC, alar soft tissue, membranous septum, and nostril sill
Dynamic structure
Nasal muscles help to keep open during inspiration
Alar contour grafts and lateral crural (alar) strut grafts can strengthen and reinforce external nasal valve.
Turbinates
Superior, middle, and inferior turbinates
Extensions of lateral nasal cavity wall
Anterior portion of middle and lateral turbinates project into airway and can affect airway resistance.
Inferior turbinate is capable of up to two thirds of airway resistance at internal nasal valve region.
Tip:
Often, a simple outfracture (micro or mini) of the inferior turbinate, with or without mucosal resection, is all that is needed to improve nasal airway obstruction caused by turbinate hypertrophy. A complete turbinectomy is rarely indicated and can result in an “open nose” deformity with imbalance in airway resistance.
Nasal Obstruction
Types of Nasal Airway Obstruction
Allergic rhinitis: Seasonal or obstruction related to dust, pollen, or other antigens
Bilateral obstruction: Possible severe mucosal disease
Constant-fixed obstruction: May be associated with a fixed abnormality such as septal deviation
Nasal Obstruction Complaints
Nasal crusting
Dry mouth (from mouth breathing, especially during sleep)
Frequent sore throats
Sinus problems
Nasal Obstruction History
Time of onset
Duration of obstruction
Precipitating events
Rhinorrhea (amount, duration)
Epistaxis
History of trauma or surgery
Use of medications, nasal sprays
Use of alcohol, tobacco, and drugs (especially cocaine)
History of headaches, visual disturbances, and middle ear symptoms
Tip:
A deviated septum or other nasal obstruction can be a trigger for migraine headaches. Ask specifically about migraine headache history. Migraines that are triggered by this mechanism may be significantly improved with nasal obstruction correction.
Physical Examination
Visual clues
Allergic shiners: Dark circles under eyes suggesting allergic rhinitis
Supraalar pinching or an excessively narrow midvault (inverted-V deformity) may have internal nasal valve insufficiency.
Watch midvault motion during nasal respiration.
If dynamic collapse occurs, midvault support will be needed.
Senior Author Tip:
Most patients who have breathing problems may not be aware of how else they can breathe, having been breathing through their mouth their entire life. Observation of lips being open and careful examination of the internal nose is crucial to prevent compounding the problems. Evaluation of the septum may reveal deviation, synechia, or perforation.
Cottle test
Not specific because many will be positive, but is useful
Cottle maneuver: Hold unilateral cheek laterally to stabilize the nasal sidewall on one side while occluding the contralateral airway.
If significant improvement in the ipsilateral airway is noted on deep inhalation, then internal nasal valve narrowing may be present.
Alar rims
Evaluate for notching or potential thereof, especially at soft triangle.
Dynamic notching may be a reflex of patient against external valve collapse.
Evaluate position of LLC (“parenthesis tip”).
Intranasal examination
Can use thumb to push up nostril rims to observe internal nasal valve angle without artificially stenting the valve open, which can occur with a nasal speculum
Use speculum and visualize septum, valve, turbinates with and without a vasoconstrictive agent.
Evaluate for polyps, crusting, mucosal color (excessive erythema suggests allergies).
In the septum look for spurs, deviation, perforations (postsurgical or from cocaine use).
Medical Therapies
Mucosal disease from common cold (viral rhinitis) most common cause
Bacterial rhinitis may complicate viral rhinitis.
Acute and chronic bacterial infection can be treated with a combination of:
Saline solution nasal irrigation
Short course of decongestant (spray and/or oral)
Nasal steroid spray
Mucolytic therapy
Check for concomitant sinus disease, because rhinosinusitis is common, with one aggravating the other.
Allergic rhinitis
Allergen (environmental exposure) avoidance
Antihistamines
Intranasal steroid regimen
Allergy test
Rhinitis medicamentosa: Rebound vasodilation and nasal mucosa hypertrophy-hypersecretion
Caused by overuse of nasal decongestants (vasoconstrictive agents) like Neo-Synephrine and Afrin
True cause of nasal congestion must be treated to eliminate need for decongestants.
Allergic rhinitis, nasal polyposis, septal deviation, turbinate hypertrophy
Treatment: Cessation of all decongestants, course of antihistamines, nasal steroids, and possibly an oral steroid taper
Ozena: Primary atrophic rhinitis
Causes: Aggressive submucous septal resection, total turbinectomy
Squamous metaplasia of normal columnar mucosal cells
Treatment: Irrigation with saline solution, high-dose vitamin A, possible surgical closure of the nostrils
Indications and Contraindications
Aesthetic
Initiated by patient
Proper patient selection is critical.
As with any aesthetic procedure, expectations must be realistic and achievable (see Chapter 1).
This becomes more of a challenge in secondary rhinoplasty patients (see Chapter 46).
SIMON: Acronym to describe male rhinoplasty patients
Single, immature, male, obsessive, and narcissistic
Used as a rough guide to remind surgeon of “problem rhinoplasty patients”
Good communication must assimilate surgeon’s analysis and goals with those of patients.
If surgeon’s and patient’s goals are vastly different, proceeding with rhinoplasty may be imprudent.
Asking patients to list the top three things they want to have altered may be a good general idea (particularly for patients with nonspecific aesthetic goals and those unsure of their aesthetic goals).
Generally, rhinoplasty should address the imbalances between the nose and face. 12 , 15 – 17
Specific desires and complaints should be addressed while pointing out other related deficiencies (when indicated), such as a deficient chin.
For example, a patient may have a wide nasal tip but only wants “the hump gone.”
Dynamic relationships must be discussed with patients.
For example, significant hump reduction without elevation of a droopy tip will produce an imbalanced nose that appears flat and excessively droopy.
Tip:
Much of the history of rhinoplasty is rooted in ethnic rhinoplasty. Ethnic patients may present a unique challenge. Clinically relevant variations in patient desires, nasofacial morphology, and anatomic nuances should be taken into account in preoperative evaluation and surgical planning. 2 , 12 , 15 , 18 – 20
Functional
This chapter does not focus on functional techniques; however, when performing a rhinoplasty, comprehensively addressing the nasal airway is critical.
Patients without nasal airway obstruction before rhinoplasty may develop airway problems postoperatively unless preventative measures are taken.
For example:
Septoplasty 1 , 6 , 13 , 14 , 22
Important to perform simultaneously
Best source of most grafts used in aesthetic rhinoplasty
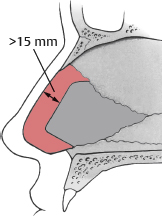
L-strut must be left intact with at least 1 cm (preferably up to 2 cm) dorsal and 1 cm caudal (Fig. 45-9).
All bony protrusions and spicules should be excised to open airway effectively.
Most critical location is across from inferior turbinate.
A protuberant nasomaxillary crest is common and should be thoroughly addressed.
Tip:
A large elevator (Boies) or nasal speculum should freely pass, without resistance, into the bilateral nasal airway after septoplasty.
Senior Author Tip:
Leaving a dorsal strut of <2 cm may result in sinking of the dorsum and development of a hump that was not present intraoperatively.
One of the most common reasons for unsuccessful straightening of a caudal nose deviation is failure to detect and reposition the dislodged caudal septum in the correct position on the nasal spine and maxillary crest. This requires removal of the redundant overlapping portion of the cartilage to facilitate repositioning the septum in the midline.
Preoperative Evaluation
Tip:
The key component of a successful rhinoplasty is accurate, detailed, and thorough preoperative analysis. Rhinoplasty has evolved into a more predictable operation because of improvements in preoperative assessment of the nasal imbalances and aesthetic deformities. After proper preoperative analysis, a component-directed surgical plan can be developed to help guide the surgeon during rhinoplasty.
Preoperative analysis requires an external examination of AP, lateral, and basilar views in addition to an internal airway examination.
Ethnic variations should be taken into account, because anatomic variations in nasofacial morphology, as well as culture-specific goals, may not always be clear (see Chapter 47).
Racial incongruity should be prevented.
A nose that is off balance with the rest of the ethnic facial traits
Skin thickness and degree of sebaceousness are best seen in AP view.
Tip:
Thick skin requires more aggressive cartilage frame modifications and conservative soft tissue debulking to reveal the true nasal shape. 2 , 18 – 20 , 23
Anteroposterior View
Symmetry and Nasal Deviation
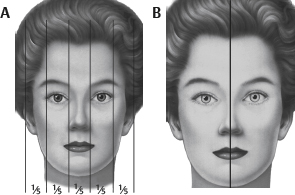
AP view of face can be divided into fifths to help evaluate proportion (Fig. 45-10, A).
Intercanthal width and alar base widths should coincide with measurements of fifths.
A line can be drawn to bisect the nasal dorsum, upper lip, Cupid’s bow, and central incisors to assess magnitude of nasal deviation (Fig. 45-10, B).
Facial asymmetries are considered.
Nasal deviation may be caudally located presenting a “twisted” appearance.
Role of asymmetry in size and shape of nasal and malar bones is evaluated.
Aesthetic Lines and Measurements
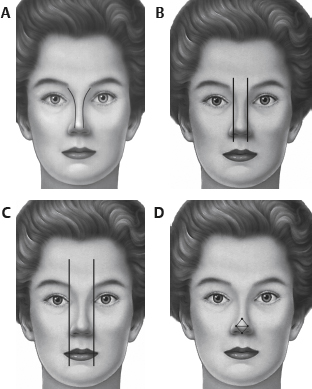
Dorsal aesthetic lines (Fig. 45-11, A)
Symmetry, deviation, width, and shape are important.
Should be gently diverging curvilinear lines extending from medial eyebrow (superciliary ridge) toward nasal tip-defining points
Width of bony base (Fig. 45-11, B)
Should be 75%-80% of alar base width
Asymmetries may exist from different angles of inclination of the nasal bones and ascending process of the maxilla.
Commonly, one side is wider (projecting more laterally) than the other.
Width of alar base (Fig. 45-11, C)
Should coincide with intercanthal width (generally)
If wider than intercanthal width, then degree of alar flare will dictate operative plan
Evaluation:
Maximal alar flare width difference from width of alar base assessed
If >2 mm, then alar flaring is present.
If < mm, then the alar base itself is wide (excessive interalar distance).
Retraction or excess inherent “nostril show” is evaluated.
On lateral view, alar-columellar relationship should be balanced.
Should have a natural flare and inclination
Outline of infratip breakpoint should appear like a “seagull in gentle flight.”
Nasal tip (Fig. 45-11, D)
Four tip-defining points: One on each dome apex, a supratip break, and a columellar-lobule breakpoint
Lines can be drawn to assess asymmetry.
Domal angle and angle of domal divergence are assessed.
Imbalance in nasal tip aesthetic contour has various descriptions, such as bulbous, boxy, amorphous, and wide.
Tip:
Evaluating tip aesthetics, as with other nasal proportions, requires careful attention to how the light reflects off the nose. External shadows and highlights on the nose provide important clues about the underlying framework. For example, asymmetry in the tip-defining point may reveal asymmetry in height, width, shape, and position of the lateral, middle, and medial crura.
Senior Author Tip:
The intercanthal midline should be used as a reference (not the point bisecting the intereyebrow distance), because patients may pluck their eyebrows differently to reduce the impact of the nose deviation on the face.
Lobule
Excess columella or hanging columella leads to excess infratip lobule.
Breakpoints should be in harmony making a diamond shape.
Caveat: Ethnic and gender variations should be considered.
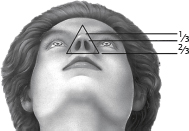
Basilar View
Alar rims should form an equilateral triangle.
Nostril height (columellar length) to infratip lobule height ratio should be approximately 60:40, respectively.
Nostril inclination is approximately 60 degrees.
Note:
Ethnic features can vary significantly.
Nostril has teardrop shape.
Alar rims should not be excessively concave or convex, within the confines of an equilateral triangle.
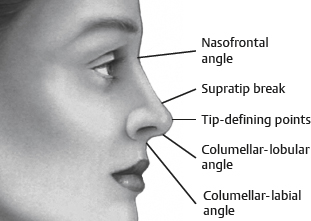
Lateral View
Multiple lengths and angles contribute to an aesthetically pleasing lateral view (Fig. 45-13).
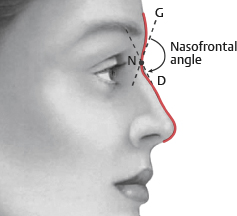
Nasofrontal angle (NFA)
Located at upper lash line and supratarsal crease (Fig. 45-14)
Formed by the intersection of the line between the glabella and the soft tissue nasion and the nasal dorsum tangent
NFA should be approximately 140 degrees.
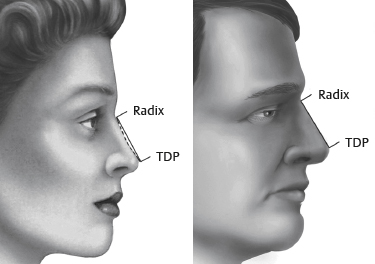
Dorsal curvature
Determined by a line drawn from the radix at the NFA to the tip-defining point (Fig. 45-15)
Female dorsum should be 2 mm posterior to this line.
Male dorsum should be at or slightly anterior to this line.
Angle of this line and where it begins can change the appearance of length.
Radix can be high or low.
Deep and inferiorly located radix has shortened nasal length (Fig. 45-16).

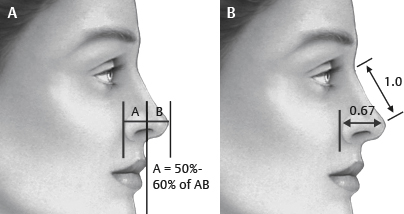
Tip projection (Fig. 45-17) 16
Ideally tip projection should be 50%-60% of the distance of a line drawn from the alar-cheek crease to the most anterior tip point (see Fig. 45-17, A).
Alternatively, tip projection is 0.67 × the nasal length. 5
Can also be assessed on basilar view
Must be proportionate to chin and lip projection
Tip rotation (Fig. 45-18)
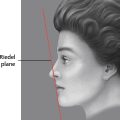
Draw line extending from anterior and posterior nostril rim.
Draw plumb line that is perpendicular to natural horizontal facial plane.
Angle between the nostril line and plumb line is the nasolabial angle (NLA) (see Fig. 45-18, A).
NLA is 95-110 degrees in females and 90-95 degrees in males.
Columellar-labial angle: Junction of columella with upper lip; varies with degree of columellar fullness and “hang”
Columellar-lobular angle: Junction of columella with the infratip lobule (30-45 degrees)
Note:
Ethnic variations and racial congruity should be considered.
Related posts:




Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


