43. Nasolabial Fold
Pertinent Anatomy
The nasolabial fold is a combination of complex mechanisms consisting of skin, adjacent redundant cheek, the nasal ala, the lip, and dermal attachments of the various interacting and overlapping facial mimetic muscles with independent vectors of interaction, all affecting the modiolus, and thus the human smile. 1 – 8
Observations about the Nasolabial Fold after Anatomic Dissection
Gross Dissection
The fold is a distinct fusion plane that separates the fatty cheek from the dense upper lip.
The nasolabial fold is a discrete unit with distinct anatomic boundaries. 9
Upper lip mimetic muscles insert into the orbicularis oris at the level of the fold.
The exact arrangement of the muscular insertions into the dermis along the nasolabial fold is unknown, but perhaps this is what contributes to the uniqueness of every person’s nasolabial fold.
Little superficial fat covers the orbicularis oris, and in contrast, more fat is above the fold in the cheek region.
The zygomaticus major and minor, levator labii superioris, and levator labii superioris alaeque nasi lie beneath the subcutaneous tissues.
The levator anguli oris and buccinator muscles are deeper.
The mimetic muscles abut the overlying dermis only when they reach the orbicularis oris border.
Medial to the fold is a paucity of subcutaneous fat between the dermis and orbicularis oris, where skin is adherent to the sphincter directly.
The upper lip levators are protected by a generous amount of subcutaneous fat from their origin on the zygoma and maxilla to their insertion into the orbicularis oris and modiolus.
The modiolus 6 : Fibrovascular structure that forms a dense, compact, mobile mass.
Consists of interlacing arrays of terminal muscle fibers converging toward (labial tractors) or diverging away from (orbicularis oris) the center
Center is situated about 1.5 cm away from the labial commissure.
Texture, volume, and thickness (about 1 cm) can be palpated on bidigital examination.
Apex is covered by panniculus fibrosus.
Tip:
The complex anatomy of nasolabial fold is well defined and must be understood in order to address clinical changes that occur and select appropriate and individualized treatment.
Histologic Observations
Responses to several publications 3 , 4 , 5 – 7 , 10 on microscopic anatomy around the nasolabial fold have overlapping, complementary elements:
The various mimetic muscles eventually insert into the entire perioral sphincter, composed of orbicularis muscle and modiolus.
The zygomaticus major and minor, modiolus, and levator labii superioris have cutaneous slips extending intermittently into the nasolabial fold dermis.
The nasolabial fold comprises (1) dense fibrous tissue, (2) muscle fibers branching from the levator muscles of the upper lip, and (3) striated muscle bundles originating in the fold fascia.
The lip elevator muscles and the “fold muscles” course down the lip to traverse the orbicularis oris and insert into the dermis of the (1) upper lip, (2) the cutaneous vermilion junction, and (3) the vermilion.
The muscle fibers of the levator superioris and zygomaticus major course down the cheek, with some muscle fibers separating from the main body to insert into the nasolabial fold fascia, traveling in many directions at the fold.
The Smas and the Nasolabial Fold
Understanding the unique relationship between the nasolabial fold and the SMAS is critical to improving the aging face in this transitional zone of the central face. Histologic examinations elucidating the two have increased our understanding towards improving the nasolabial fold, whether surgically or nonsurgically.
Complementary and supporting histologic evidence from various dissections gave rise to certain conclusions about the SMAS and the nasolabial fold. 3 , 11
The SMAS continues anteriorly up to the level of zygomaticus major muscle, at which point it seems indistinguishable from the investing fascia of the muscle.
The attenuated SMAS also invests the undersurface of the zygomaticus muscle similar to its superficial coverage.
A natural plane of dissection follows the deep surface of the SMAS behind the zygomaticus major muscle and into the buccal space.
As it approaches the nasolabial fold, the SMAS anatomically divides into superficial and deep fascial leaves and envelops zygomaticus major and minor muscles.
No separate subcutaneous extension of the SMAS appears to exist.
Dynamics of the Nasolabial Fold
The movement of the nasolabial fold encompasses the complex anatomy and is a unique interaction between skin, the various facial mimetic muscles, adjacent fatty soft tissue (or the lack thereof), and the upper lip, all of which define the human smile and affect the expression of emotions. Following are some clinical observations 4 , 12 :
Individual facial muscles retain their identity and can be stimulated to contract independently.
Some muscles completely control a specific expression, whereas others incompletely control expressions, ranging from partial to full expression of the same emotion.
Elevation of the upper lip (or smiling) deepens the nasolabial fold in all people.
Smirking involves contracting single muscles and can produce discrete, unique dimples along the fold.
These discrete contour irregularities (dimpling) are the only sign of muscle action in a face that is in repose.
Full smiling exaggerates dimpling.
The dynamics of the fold move the upper lip to create different types of surface depressions. 4
A comma-shaped crease lateral to commissure
A dimple above the modiolus
A narrow puckering along the fold in the upper lip (prominent at the beginning of the lip elevation but consumed by a full smile)
Shallow dimple next to the nasal ala in the upper fold
Some people have one dimple, and others none, but rarely are two dimples present in a person.
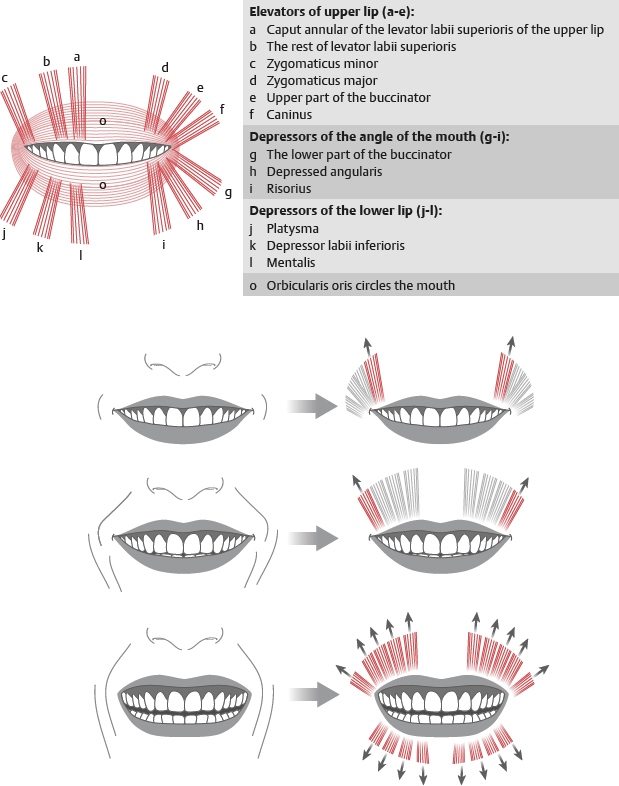
The Human Smile
Actions of the muscles surrounding the nasolabial fold and mouth give rise to the human smile, and one author noted the nasolabial fold as a keystone to the smiling mechanism. 10 , 13 , 14
The smile is formed in stages.
First stage
The lip is raised to the fold by the levator muscles and the muscle bundles originating at the fold.
The lip meets resistance at the fold because of the overlying fatty cheek mass.
Second stage
Involves the levator muscles of the upper lip raising the lip and fold upward
Paralysis of facial muscles effaces the nasolabial fold, confirming action of the mimetic muscles and their influence on deepening of the fold.
In death, the nasolabial fold is retained.
The fold is shallow in babies and deepest in elderly people.
What Deepens the Nasolabial Fold?
Deep folds are a sign of aging, and the mechanism and dynamics of the fold contribute to the gradual deepening of the folds. The following factors contribute to the deepening of the folds 4 :
Redundant skin in the overlying cheek
Ptosis of the subcutaneous fat above the nasolabial fold
Undercutting by the upper lip retractor muscles, particularly the levator labii superioris. Yousif et al 5 provided another perspective to the causes of the deepening nasolabial fold.
The nasolabial fold is the point of juncture between two skin territories.
Lateral to the fold, the territory contains no cutaneous muscle attachments, and thus is not supported by the muscles.
Medial to the line of the nasolabial fold, the muscles insert on the skin and support this area against gravity and laxity of aging skin.
During aging, the “unsupported” skin and cheek mass lateral to the fold descends at a much greater rate than the skin medial to the fold.
Tip:
The discrepancy in the rate of descent of two adjacent skin territories creates and accentuates the nasolabial fold.
Mendelson 15 compared cheek and lip contours separated by the nasolabial fold and noted the following effects of aging:
The contour of the youthful face becomes divided into a series of folds (convexities) and furrows (concavities).
In the midcheek, the round fullness of the youthful face is slowly lost, and hollowing appears as an obliquely oriented midcheek furrow.
The cheeks appear larger with aging, partly from the nasolabial furrow moving medially toward the lip.
Fullness and downward displacement of upper lip fold changes the commissure, which appears deeper and longer and droops to become the marionette furrow.
Lower lip loses its flatness to become more of a rounded fold that exaggerates depth of the marionette furrow.
Mental crease becomes deeper, longer, and downturned, as the labiomental groove.
A photogrammetric analysis further defines the relationship with aging and deepening of the nasolabial fold. 16
With aging, the cheek mass displaces anteriorly, laterally, and inferiorly.
This displacement deepens the nasolabial fold.
The relationship between the upper lip and fold remains constant.
The lateral commissure moves laterally, while the apparent angle of the nasolabial fold decreases.
Tip:
Deepening of the nasolabial fold is caused by changes in the cheek mass and its support.
Related posts:




Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


