4 Upper Eyelid Entropion
Abstract
“Upper Eyelid Entropion” discusses an eyelid malposition in which the upper eyelid margin is turned inward against the eyeball. It can be responsible for severe ocular morbidity. It is an uncommon condition in the developed world but is more common in developing countries where trachoma is endemic. It has tended to receive very little attention in standard oculoplastic texts even though its management can be difficult and challenging. Upper eyelid entropion may be broadly classified as congenital or acquired. This chapter describes all surgical procedures and postoperative care in each instance in detail.
4.1 Introduction
Upper eyelid entropion is an eyelid malposition in which the upper eyelid margin is turned inward against the globe. It can be responsible for severe ocular morbidity. It is an uncommon condition in the Western World, in contrast to a number of countries in the Third World, where trachoma is endemic. It has tended to receive very little attention in standard oculoplastic texts despite the fact that its management can be difficult and challenging. Upper eyelid entropion may be broadly classified as congenital or acquired.
4.2 Classification of Upper Eyelid Entropion
4.2.1 Congenital
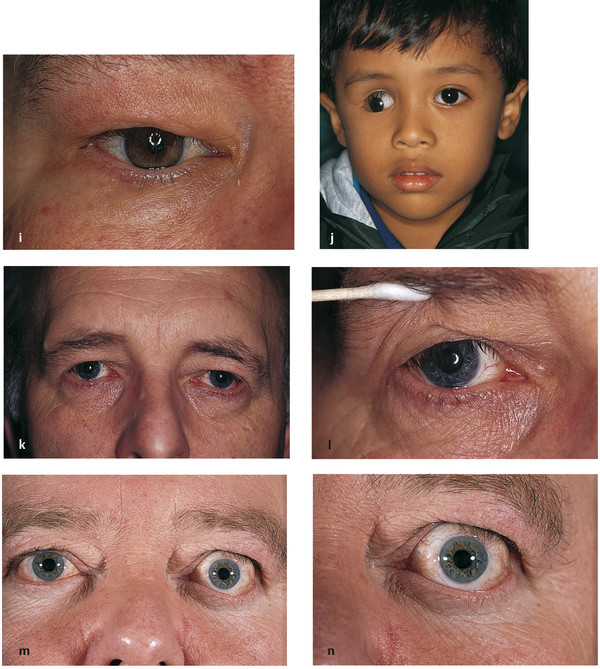
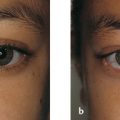
A true congenital upper lid entropion is very rare. A horizontal tarsal kink is a similar but separate entity. The upper lid tarsus in affected patients is commonly found to be abnormal and foreshortened (Fig. 4‑1).
4.2.2 Acquired
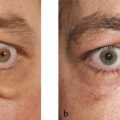
Acquired upper lid entropion can be further classified according to the underlying cause. Any cause of conjunctival scarring can lead to an acquired upper lid entropion. The entropion may be further subclassified according to its severity as mild, moderate, or severe.
Trachoma (Fig. 4‑2a).
Chronic blepharoconjunctivitis.
Chemical burns.
Cicatrizing conjunctivitis.
Topical glaucoma medications.
Stevens-Johnson syndrome (Fig. 4‑2b).
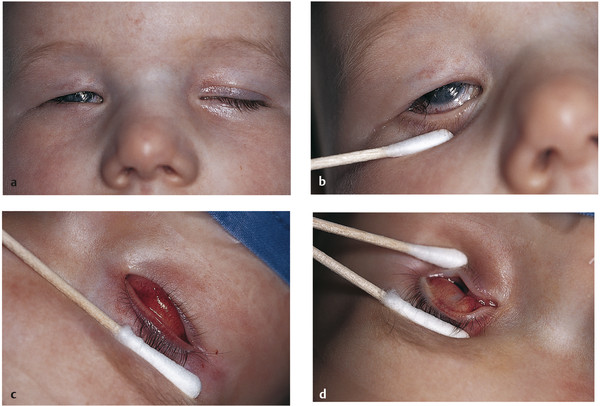
Herpes zoster ophthalmicus (Fig. 4‑2c,d).
Ocular cicatricial pemphigoid (Fig. 4‑2e,f).
Iatrogenic—such as a complication of the Fasanella-Servat procedure (Fig. 4‑2g,h).
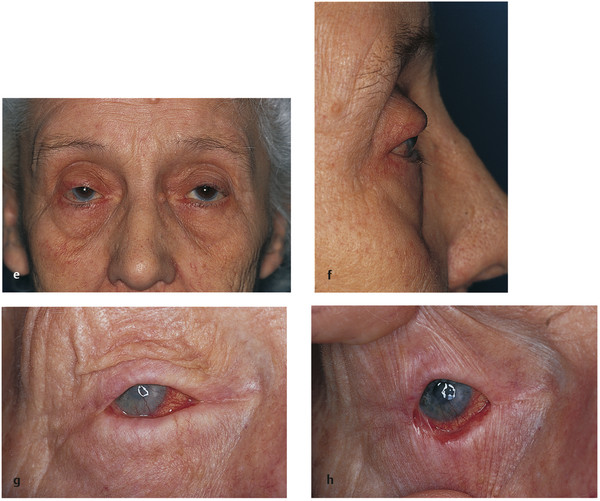
Chronic anophthalmic socket inflammation (Fig. 4‑2i,j).
Severe eyebrow ptosis (Fig. 4‑2k,l).
Thyroid eye disease (Fig. 4‑2m,n).

4.3 Patient Assessment
A careful history and meticulous clinical examination are essential to determine the cause of the entropion. In addition to a complete ocular examination, the eyelid should be everted and the posterior lamella and the superior fornix examined. It is important to establish the presence of an upper eyelid entropion and differentiate this from simple trichiasis. The presence of an early entropion is indicated by an apparent posterior migration of the meibomian gland orifices. It is important to determine whether any keratin is present on the posterior lamella. The presence and degree of eyelid retraction and lagophthalmos should be determined. If an artificial eye is present, this should be removed, and the superior fornix examined.
4.4 Surgical Management
A number of factors influence the operative management of this eyelid malposition (Box 4.1).
Box 4.1 Factors Influencing the Surgical Management of Upper Eyelid Entropion
The severity of the entropion
The thickness of the tarsal plate
The presence or absence of keratin on the posterior lamella
The degree of eyelid retraction
The degree of any lagophthalmos
The underlying etiology
The presence of a corneal graft
The planning of a future corneal graft
The presence of an artificial eye
4.4.1 Congenital Upper Eyelid Entropion
In some cases the upper lid entropion resolves spontaneously, but if it is causing distress or ocular complications the eyelid malposition should be corrected surgically. This is performed under general anesthesia.
Upper Lid Auricular Cartilage Graft
Surgical Procedure
The upper eyelid skin crease is marked with gentian violet after degreasing the skin with an alcohol wipe.
Between 2 and 3 mL of 0.25% bupivacaine with 1:200,000 units of adrenaline are injected along the upper lid skin crease immediately under the skin to prevent bleeding from the orbicularis muscle and the development of a hematoma.
A 4–0 silk traction suture is placed through the gray line of the upper eyelid centrally, and the eyelid is everted over a Desmarres retractor.
A small quantity of the local anesthetic solution is also injected subconjunctivally just above the tarsus. The Desmarres retractor is removed.
A skin crease incision is made with a No. 15 Bard Parker blade.
The incision is carried down to the tarsus centrally using blunt-tipped Westcott scissors.
The entire anterior surface of the tarsus is exposed using the Westcott scissors down to the eyelash follicles, with care not to damage these.
The eyelid retractors (the levator aponeurosis and Müller’s muscle) are freed from the surface and superior margin of the tarsus with the Westcott scissors.
An auricular cartilage graft is harvested from the patient’s ear (see Chapter 13).
The auricular cartilage graft is shaped to mimic the size and shape of a normal tarsus.
This is then placed over the patient’s tarsus, extending above its superior border onto the conjunctiva ( Fig. 4.9 ). Interrupted 7–0 Vicryl sutures may be used to fixate the graft to the patient’s tarsus.
The levator aponeurosis is then attached to the superior third of the cartilage graft with interrupted 5–0 Vicryl sutures.
The skin crease is reformed using interrupted 7–0 Vicryl Rapide sutures, taking a bite of the lower skin edge, then a bite of the eyelid levator aponeurosis, and finally a bite of the upper lid skin edge. This is tied tightly, creating a well-defined eyelid crease.
Antibiotic ointment is instilled into the eye.
Postoperative Care
The patient is discharged with a topical antibiotic ointment to apply three times per day to the eyelid wound until the sutures have dissolved and topical lubricants to be used for 3 to 4 weeks.
The patient seen in Fig. 4‑1 and Fig. 4‑3a,b is shown before and after this surgical procedure (Fig. 4‑3c,d).
Related posts:




Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


