4. Medicolegal Considerations in Aesthetic Surgery
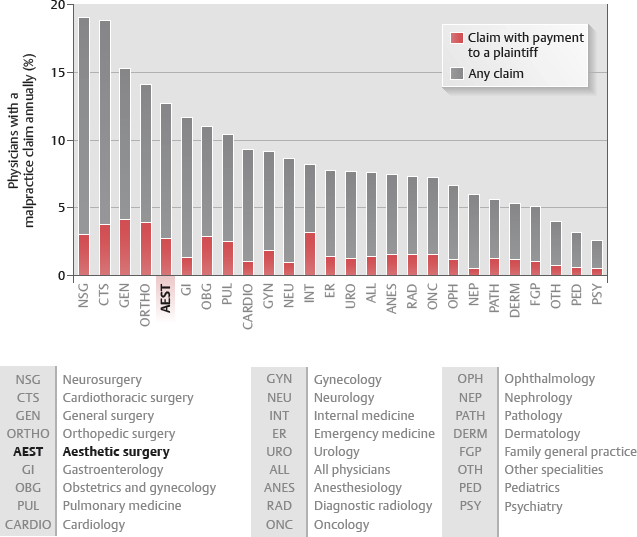
Aesthetic surgeons are the fifth most frequently sued physician, averaging one claim every 2½ years 1 (Fig. 4-1).
Prevent medical lawsuits with good patient selection, strong patient relationships, and proper documentation.
Patient Selection
More than half of the malpractice claims against aesthetic surgeons are preventable; the first step in preventing a claim is patient selection.
Expectations too Great
Patients with unrealistic and idealized expectations, or those who expect major life changes, are more likely to be disappointed with even a good surgery result.
Disappointed patients are more likely to seek legal counsel.
Patients who do not understand the risks associated with major surgical procedures are more likely to be disappointed.
Patients must understand the possible inherent complications associated with surgery.
Excessively Demanding Patients
Patients who bring photographs, drawings, and exact architectural specifications to a consultation should be managed with great caution. These patients demonstrate:
Little comprehension of the healing process vagaries
Little understanding of the natural margin of error inherent in elective surgery
Little flexibility in accepting failure
The Indecisive Patient
Senior Author Tip:
I have always had a concern about defending a decision to perform completely elective surgery with, “The patient wanted this done.” I think a patient cannot make a negligent decision. That is, the doctor has the responsibility to NOT accept patients for completely elective surgery if the choice of procedure does not reflect acceptable expectations and is achievable. Just because a patient asks for something does NOT mean it should be performed if inappropriate.
Question: “Doctor, do you think I ought to have this done?”
Answer: “I cannot make that decision for you; if you have any doubt whatsoever, I strongly encourage you to reconsider.”
The decision to undergo surgery is motivated from within:
Strongly motivated patients are more likely to be satisfied with the results.
CAUTION: Never “sell” a patient on a procedure.
Selling the patient may lead to “buyer’s remorse” ➤ lawsuit.
The Immature Patient
Youthful and immature patients may have excessively romantic expectations.
Maturity and age do not always correlate.
The Secretive Patient
Be cautious of patients desiring secret surgery or requesting elaborate precautions to prevent knowledge of their surgery. This suggests guilt about the surgery.
Guilty patients are more likely to be dissatisfied.
Dissatisfied patients are more likely to sue.
Family Disapproval
Family approval is not necessary, but family disapproval is a relative contraindication:
Less optimal results may produce the “I told you so” familial reaction.
Such reaction may deepen patient’s guilt and dissatisfaction.
Patients Physicians Do Not Like (or Who Do Not Like Them)
Surgeons should not accept patients they dislike.
Clash of personalities may affect the case outcome and/or postoperative care.
Surgeons should not accept patients who do not like them.
Perception of bad outcome is more likely, even with a good result.
Patients are much more likely to sue doctors they do not like.
The “Surgiholic”
WARNING: Patients with multiple aesthetic surgeries are not good candidates because:
Personality problems: Patients are probably compensating for poor self-image.
Difficult anatomy from previous procedures
Risk of unfavorable comparison with previous surgeons
Senior Author Tip:
Performing surgery on surgiholics is not worth the risk
Body Dysmorphic Disorder
Beware of patients who are occupied by physical traits that are hardly noticeable and within normal limits. Patients with body dysmorphic disorder never carry a diagnosis openly.
Avoid the temptations of financial gain.
A valid credit card is a poor criterion for elective aesthetic surgery.
Practice good surgical judgment.
Patients obsessed with a minor defect will probably continue to obsess, even with a good surgical result.
Patient Communication
Busy doctors are less likely to listen effectively; ineffective listening can lead to the perception of arrogance and disinterest, which leads to lawsuits.
Informed consent is a process and sometimes is never achieved, even after many visits.
Ten Listening Behaviors to Avoid
Dismissing the subject matter as uninteresting
Surgeons must not become bored with the same complaints they have heard many times before; patience is a virtue: refuse the urge to “move the conversation along.”
Feigning attention
More often than not, patients realize their doctor is merely “appearing engaged.”
Losing interest in verbose explanations
Patients’ explanations of their symptoms are often lengthy and unorganized.
Physicians must actively listen to their patients’ explanations to appropriately synthesize the information that allows proper care.
A disorganized patient presentation is not a defense against a lawsuit.
Listening is a physician’s duty.
Allowing distractions
Interruptions (phone, intercom, pager) should be avoided.
Becoming distracted by the speaker
Physicians should listen to patients, even those with distracting mannerisms or physical characteristics.
Listening only for facts
Physicians are scientifically trained to focus on objective observations and quantitative data. Human patients, however, are not objective or quantitative; physicians must comprehend the equally important patient emotional overtones and behavior.
Becoming distracted by the presentation
Surgeons should not become enamored with the patient’s speaking style or mannerisms, because it may cause them to miss what the patient is saying.
Allowing emotion-laden words that arouse antagonism
Angry or defensive reactions to patient comments should be avoided.
“We” is used, instead of “you.”
Note-taking
Note-taking is essential for documentation, but can be distracting.
Surgeons should listen to and make eye contact with patients, then jot down the key words needed to reconstruct the conversation shortly after the consultation.
Wasting the advantage of thought-speech speed
People can speak 150 words per minute but assimilate 500 spoken words per minute; thinking about something other than what the speaker is saying requires extra time and should not be done; active listening requires focus on the patient’s words.
Employing Good Listening Skills
Reflective feedback
Ask questions, make statements, and offer visual cues that indicate understanding.
Silence
Silence is golden; focus on what the patient is saying.
Positioning
Do not seem too relaxed (reflecting disinterest).
Do not cross your arms (appearing defensive).
Avoid sitting behind a desk (an ostensible barrier).
Try to lean forward ․a nonverbal communication that says, “I am interested.”
Employing Good Speaking Habits
Use calming speech tempo and voice tone.
Speak slowly and clearly; use a voice tone that reflects calm and empathy.
Pause for assimilation and feedback
Pause more often. Pausing during speaking gives the patient time to digest the words and ask for clarification.
Repeatedly invite questions; a good dialogue reinforces patients’ beliefs that they are participating in their care.
Ask patients to repeat instructions; repetition adds reinforcement.
Do not talk medi-speak
Use simple terminology (e.g., “cutting out” instead of “excise”).
A surgeon’s duty is not only to operate, but to ensure that their patients understand the surgery process; if they do not understand it, the surgeon has breached his or her duty.
Repetition
The average patient retains only 35 % of what is said; repetition can increase patient comprehension, which can prevent inflated expectations and decrease litigations.
Request written questions
After leaving the consultation, patients often remember questions they forgot to ask.
Encourage patients to write down questions they have before consultations. Answering their questions may avert a lawsuit.
Body language
Start with a friendly handshake. Eye contact is critical and holds a patient’s attention. A frown, raised eyebrow, sigh, or simple “hmmmm” can exacerbate patient anxiety. Alternatively, a gentle smile, combined with a confident caring attitude, will help to develop a solid doctor-patient relationship, which is essential for lawsuit avoidance.
Related posts:




Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


