4 Mastopexy and Reduction Mammaplasty
The indications for mastopexy or reduction mammaplasty are based on the physical examination as well as the patient’s individual aesthetic perception. While some patients may have purely ptotic breasts (possibly requiring augmentation) and others have heavy breasts that clearly require reduction, a number of women will naturally fall in between these two extremes.
A successful mastopexy or reduction mammaplasty includes the following steps:
1. Relocation of the nipple–areola complex higher on the breast.
2. Reduction of glandular tissue, fat, and skin.
3. Creation of the new breast, leaving a scar that is as inconspicuous as possible and producing a result that is stable over time.
There are numerous ways of achieving a successful outcome. The appropriate procedure should be tailored to the individual and to the surgeon’s experience with one or more techniques. It is not within the scope of this textbook to describe all of the possible techniques for mastopexy and reduction mammaplasty. Instead, we will focus on the surgical techniques that are regarded by the authors as being the most valuable.
Surgical techniques can be grouped relative to the resulting postoperative scar into periareolar, short/vertical scar, and T-scar techniques. The appropriate surgical technique depends on the volume of tissue to be removed: minor reductions are usually managed with short-scar techniques and large reductions with long-scar techniques.
In the past, almost all reduction mammaplasties were carried out using the T-scar technique. In the last 15 years, the scar-sparing technique has become increasingly widely used. This is especially true for mastopexy in purely ptotic breasts, but also for reduction mammaplasty in moderate to medium-grade breast hypertrophy. Although some surgeons still choose this technique for severely hypertrophic breasts, the authors prefer T-scar reduction mammaplasty as it allows better planning and provides greater reliability in terms of the postoperative outcome.
Breast volume is, of course, a key factor in deciding whether a reduction or a mastopexy is appropriate. The two procedures are technically similar. Most mastopexies can be performed with a scar-sparing technique. In our view, a T-shaped incision is only indicated if the skin envelope is very lax. In smaller breast volumes, only the skin is resected. Breasts with inadequate volume may require implants (see the section on breast ptosis/augmentation mastopexy in Chapter 3, p. 20).
The lines of incision are marked preoperatively with the patient in a standing position. Proper marking provides the basis for a successful reduction or mastopexy. Marking also provides the surgeon with a further opportunity for preoperative assessment of the planned resection weight, asymmetries that may lead to intraoperative revision (which is always problematic), preexisting scars, etc. Marks should be made carefully and thoroughly, with attention to every detail.
Reduction Mammaplasty with a Short/Vertical Scar (Based on the Lejour Technique)
The principle of the short scar used in the Lejour reduction technique relies on extensive undermining of the skin in the two inferior breast quadrants and complete dissection of the gland, similar to a subcutaneous mastectomy. The empty skin envelope is then draped around the newly formed breast mound. Wound contraction causes the skin to shrink and contributes to postoperative shaping of the breast.
The specific steps in the surgical procedure are as follows:
1. Marking
2. Infiltration
3. De-epithelialization
4. Liposuction
5. Surgical excision and creation of a new breast mound
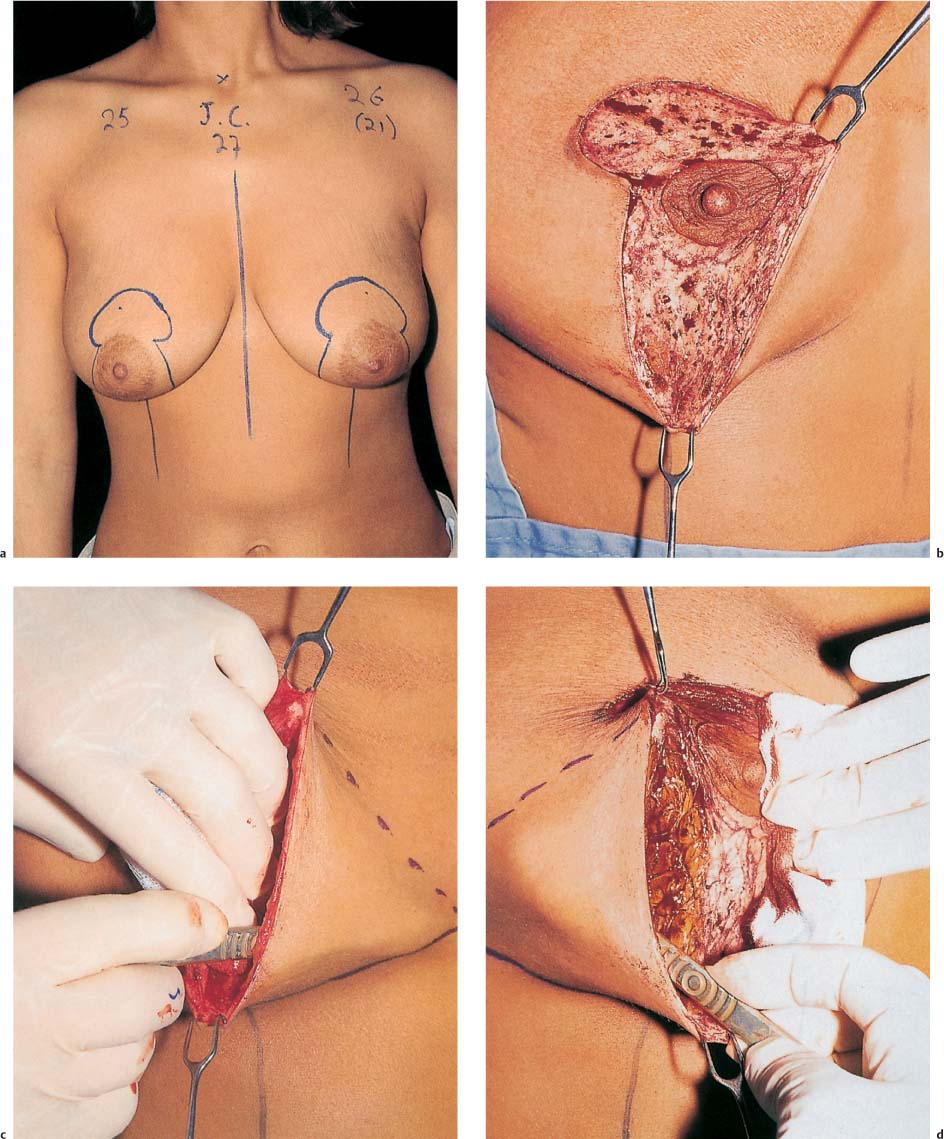
Surgical Marking (Fig. 4.2)
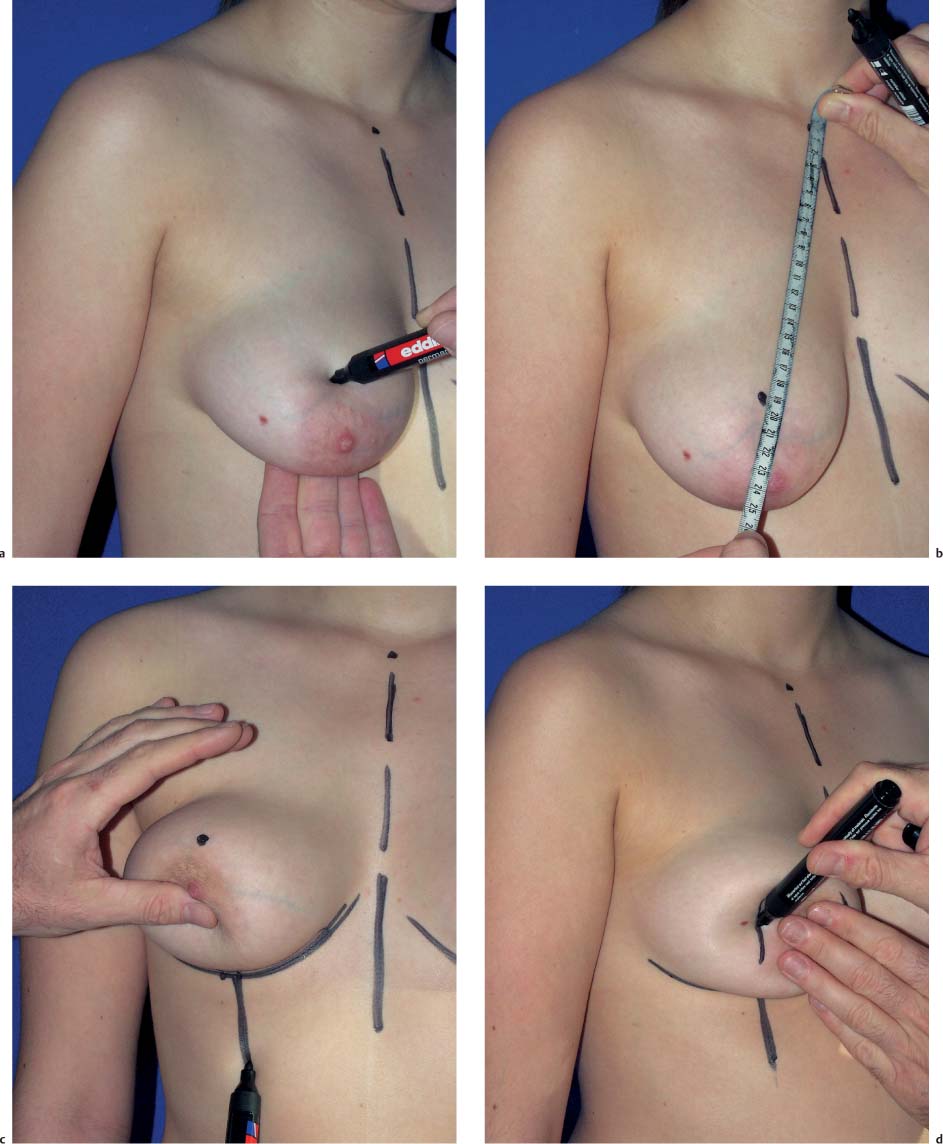
The surgical marks are drawn freehand with the patient in a standing position and are adjusted to her individual body habitus and the desired surgical result.
1. The midsternal line and inframammary fold are marked.
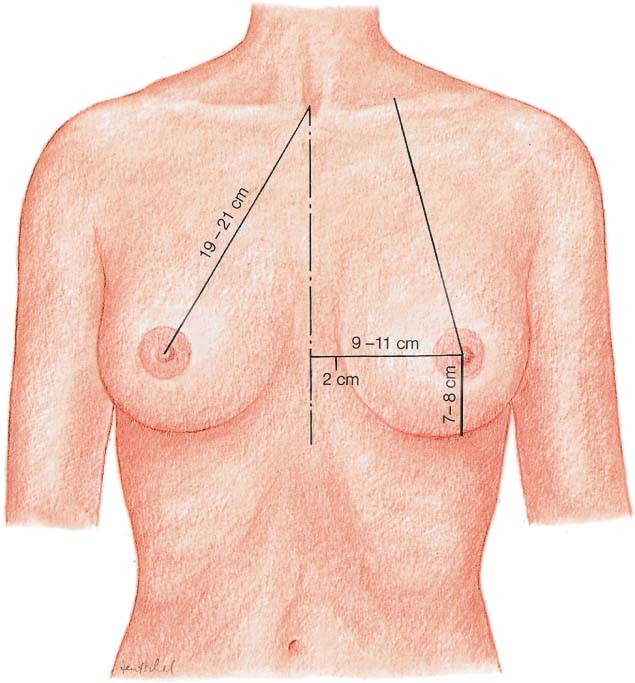
2. The future nipple site is a located at a point on the opposite side of the breast above the inframammary fold, usually 21–23 cm from the sternal notch. Overcorrection should be avoided. Since there is no true skin resection inframammilary, the new nipple site can thus sometimes appear to be too high after the operation. The future site of the nipple should therefore be marked more “conservatively” than in T-shaped incisions.
The breast is lifted with the middle finger of the left (or right) hand in the area of the inframammary fold. The new nipple position is at this point—projected from the fingerpoint onto the upper side of the breast. This point should always be confirmed by measuring the distance to the sternal notch. Nothing is more difficult to correct than a new nipple that is located too high on the breast.
3. The midline of the breast (“breast meridian”) is drawn from the inframammary fold downward. When the patient is in a standing position, it is generally at the level of the nipple and usually 9–11 cm from the midline. This vertical marking serves as a guide for determining the lateral margins of the skin resection.
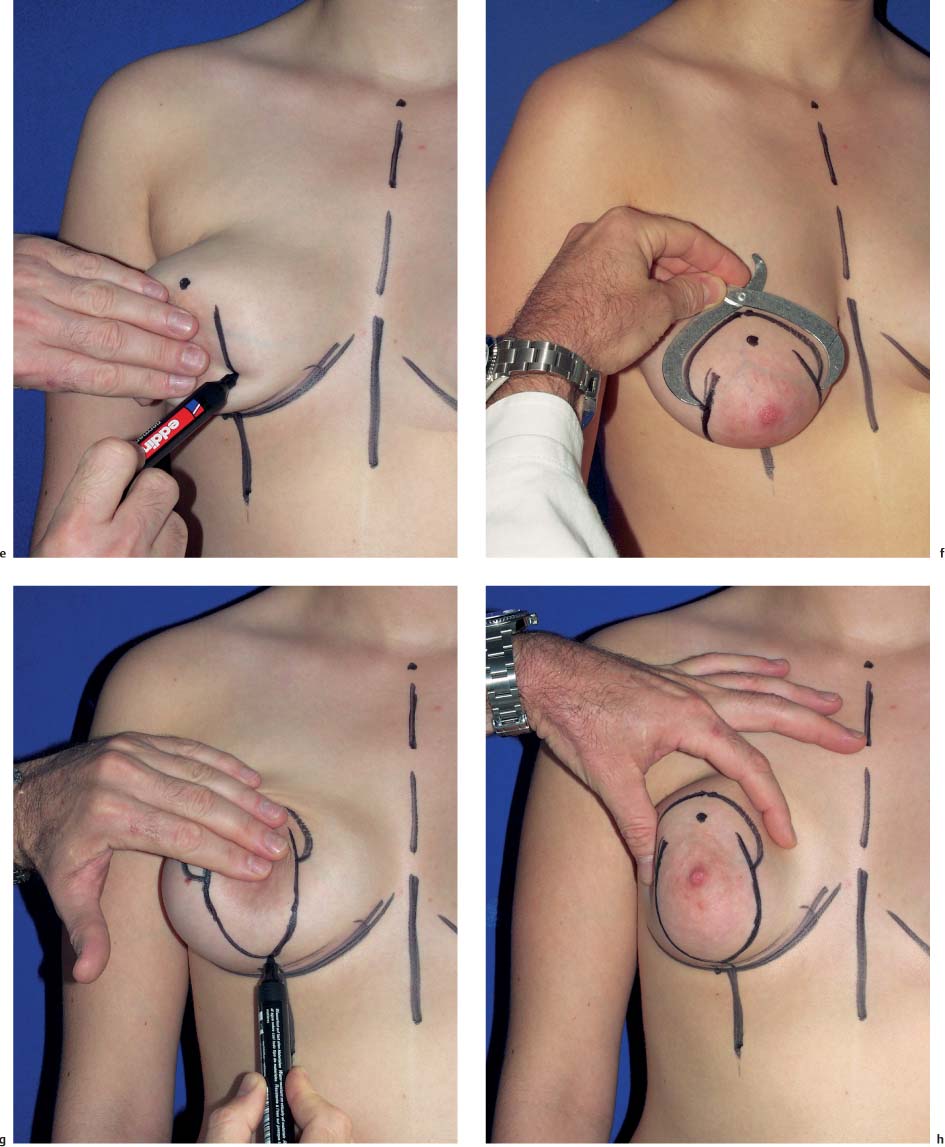
4. The lateral (vertical) resection borders are determined and drawn while the breast is being pushed medially and then laterally. It is important to push the breast upward so that the final shape will be more conical rather than flat. The degree of medial or lateral displacement varies depending on the size of the desired reduction, and a smaller or larger resection area can be marked.
5. The two vertical lines are connected inferiorly, about 2 cm above the inframammary fold.
6. While some surgeons determine and mark the new nipple position intraoperatively, the present authors prefer to do so preoperatively. The future nipple location has already been determined (as described above). Using the Lejour technique, a “mosque dome” marking is made at the future areola site. The circumference of the areola can be calculated using the formula 2 π r. Anareola with a diameter of 4 cm (=2 × 3.14 × 2), for example, would have a circumference of 12.56 cm. About 2 cm above the nipple mark, a dome-shaped area is drawn around the new nipple site, touching the vertical lines of the planned skin resection laterally. During the three-dimensional process of coning the breast during surgery, the mark, which does not initially appear to be circular, becomes rounded. Additional resection to improve the contour is therefore rarely needed.
An adjustable template with sides measuring 8 cm in length can greatly facilitate marking the new nipple site ( Fig. 4.2f ).
7. After the outer resection margins have been marked, the superior pedicle, which will be de-epithelialized, is marked. It extends from the upper border of the areola to 5–6cm below the nipple. The width of the pedicle varies depending on the breast size. While a laterally or medially based pedicle can be used, doing so contradicts one of the underlying principles of the operation, which is to remove excess adipose and glandular tissue from the lower breast pole.
Infiltration
After anesthesia has been induced, the patient is placed on the operating table in a semisitting position. The tissue in the lower portion of the breast is infiltrated in a tumescent technique with a solution of physiologic saline and epinephrine. Generous infiltration of the breast skin (excluding the pedicled nipple flap) should help minimize intraoperative bleeding.
De-epithelialization
The area above the nipple and a 5–6 cm long portion of skin below the areola are de-epithelialized. It is useful to make a spiral-shaped incision of the epidermis around the areola, followed by separation under tension.
Liposuction
In larger breasts (especially with large amounts of fat), liposuction should be carried out in the superior portion of the breast and the pedicle should be thinned.
Liposuction reduces breast volume and improves the tapering of the breast at the lateral chest wall, as well as the breast contour, especially in the cleavage area. In addition, liposuction can help facilitate plication and invagination of the pedicle, especially if the superior pedicle is long.
Liposuction is performed through a stab incision in the skin that is to be resected. Excess fat is removed with a 3-mm or 4-mm cannula. Although liposuction is generally uncomplicated, it can be difficult in patients with juvenile breast hypertrophy.
Liposuction can also be used at the end of surgery to correct minor asymmetries or relieve excess tension along the skin sutures.
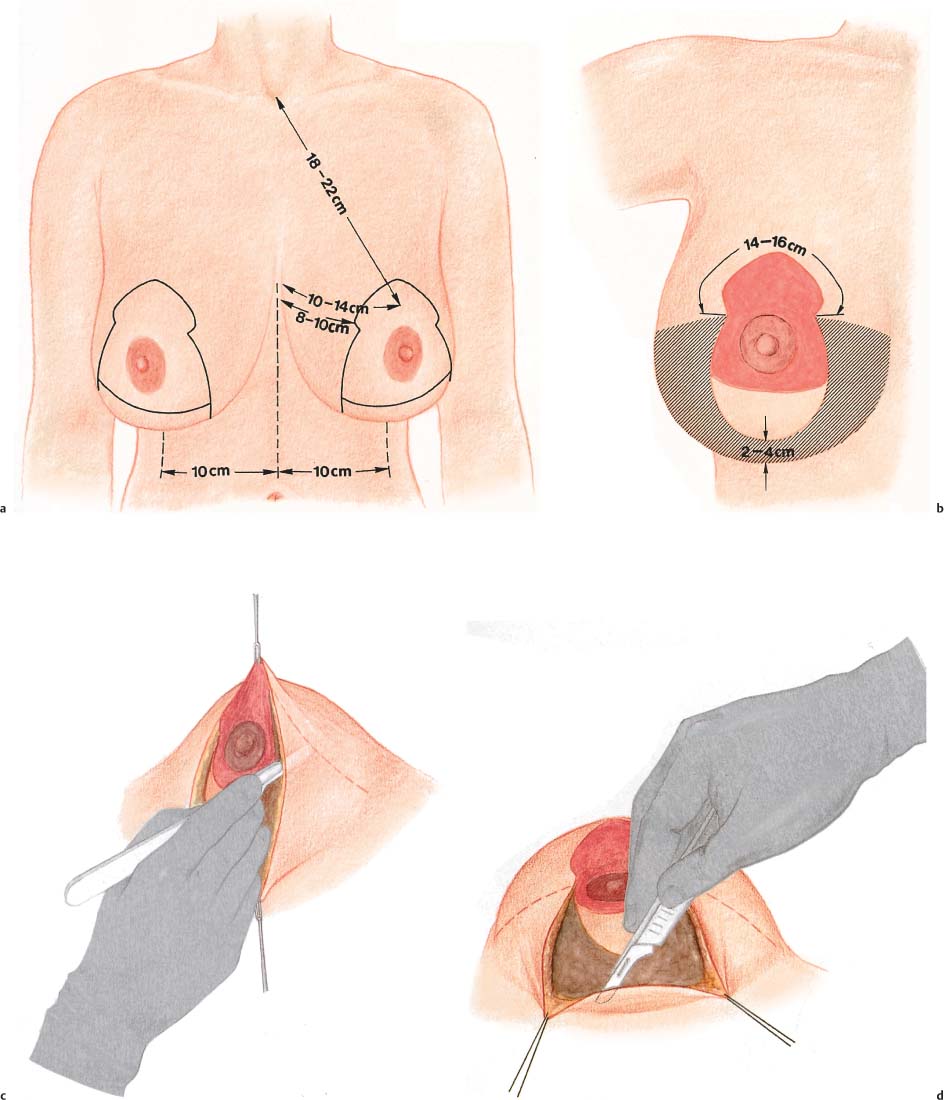
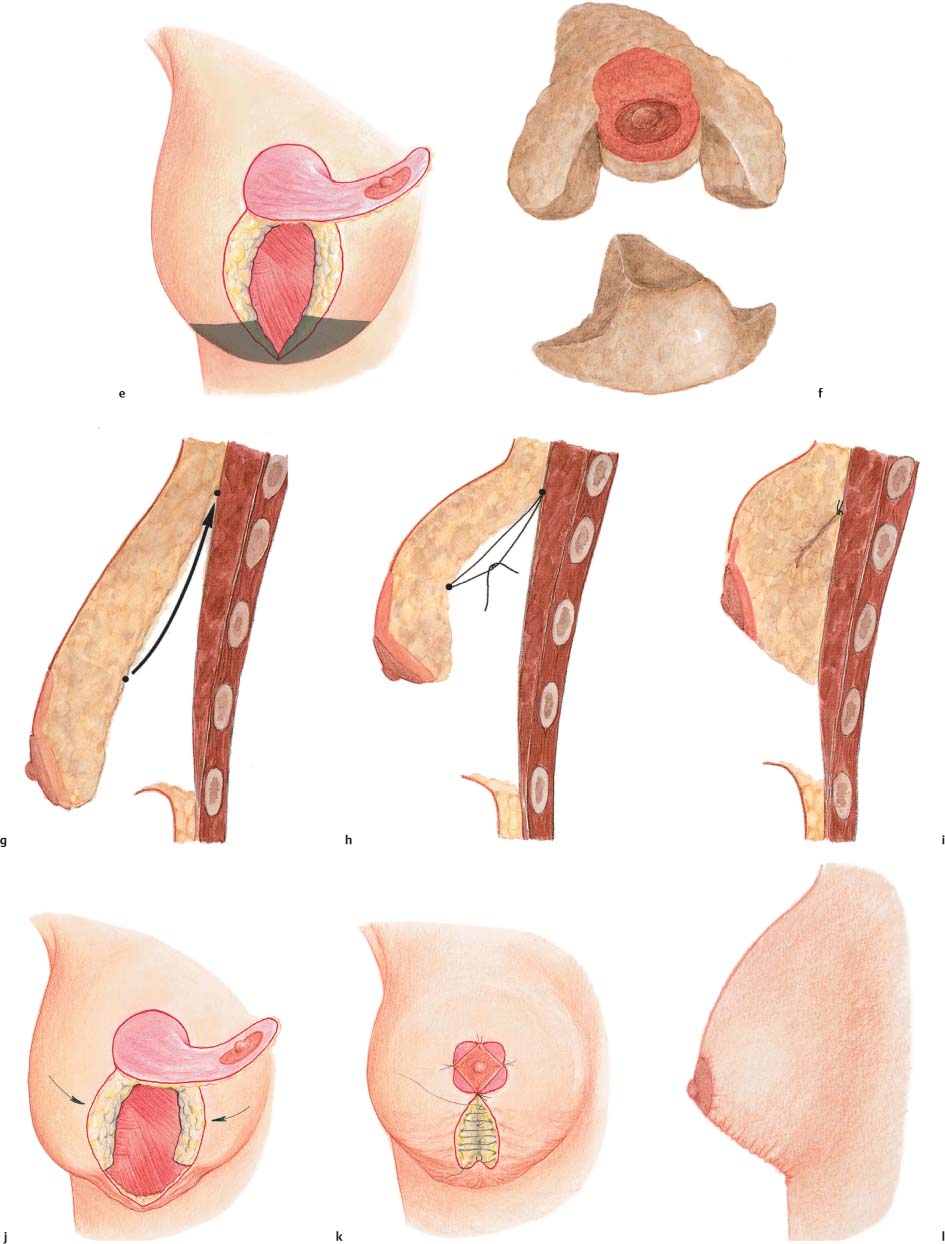
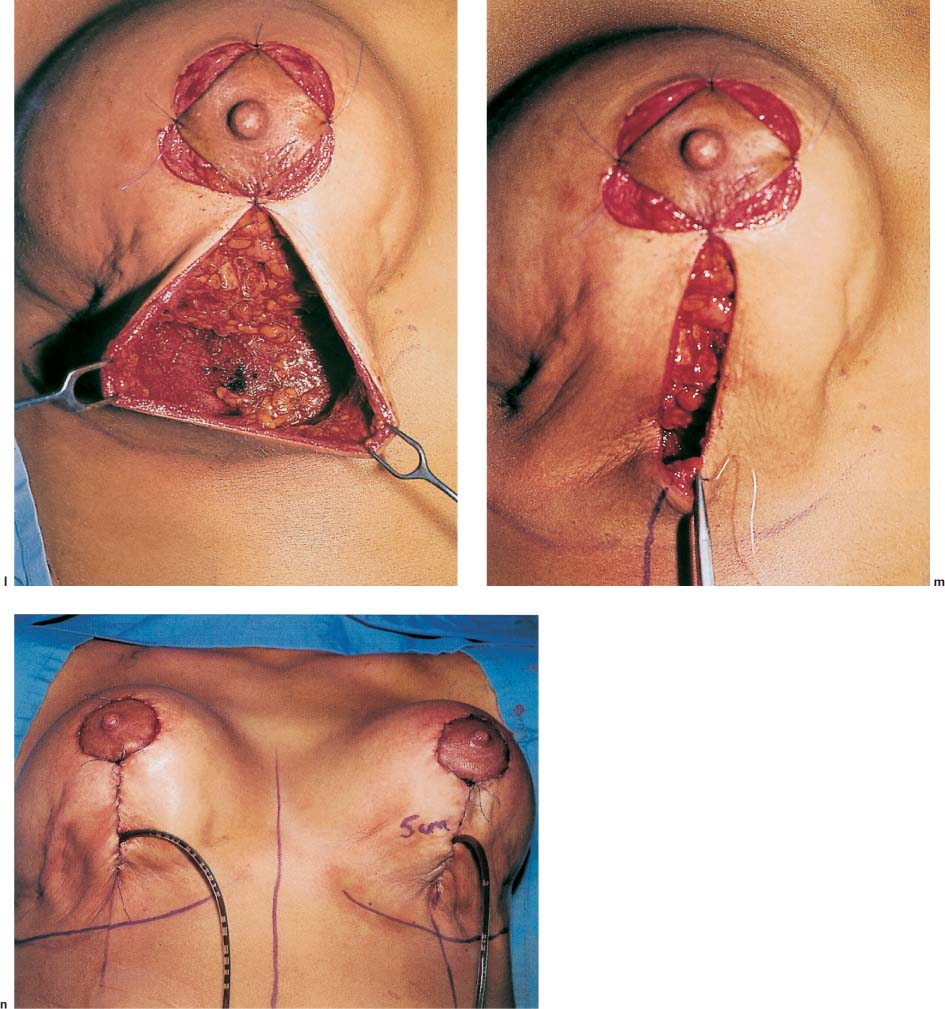
Surgical Procedure (Fig. 4.4)
The skin incision is made along the (V-shaped) markings. On both sides, it is carried 1.0–1.5 cm into the lower portion of the new areola site.
For subcutaneous dissection of the lower portion of the gland, the skin margins are clamped with ring forceps to allow superficial dissection under tension, similar to a subcutaneous mastectomy. It is important to leave only about a 0.5-cm thick layer of fat under the skin. This superficial level of dissection allows excess skin to retract. If the plane of dissection is too deep, permanent and deep skin folds result.
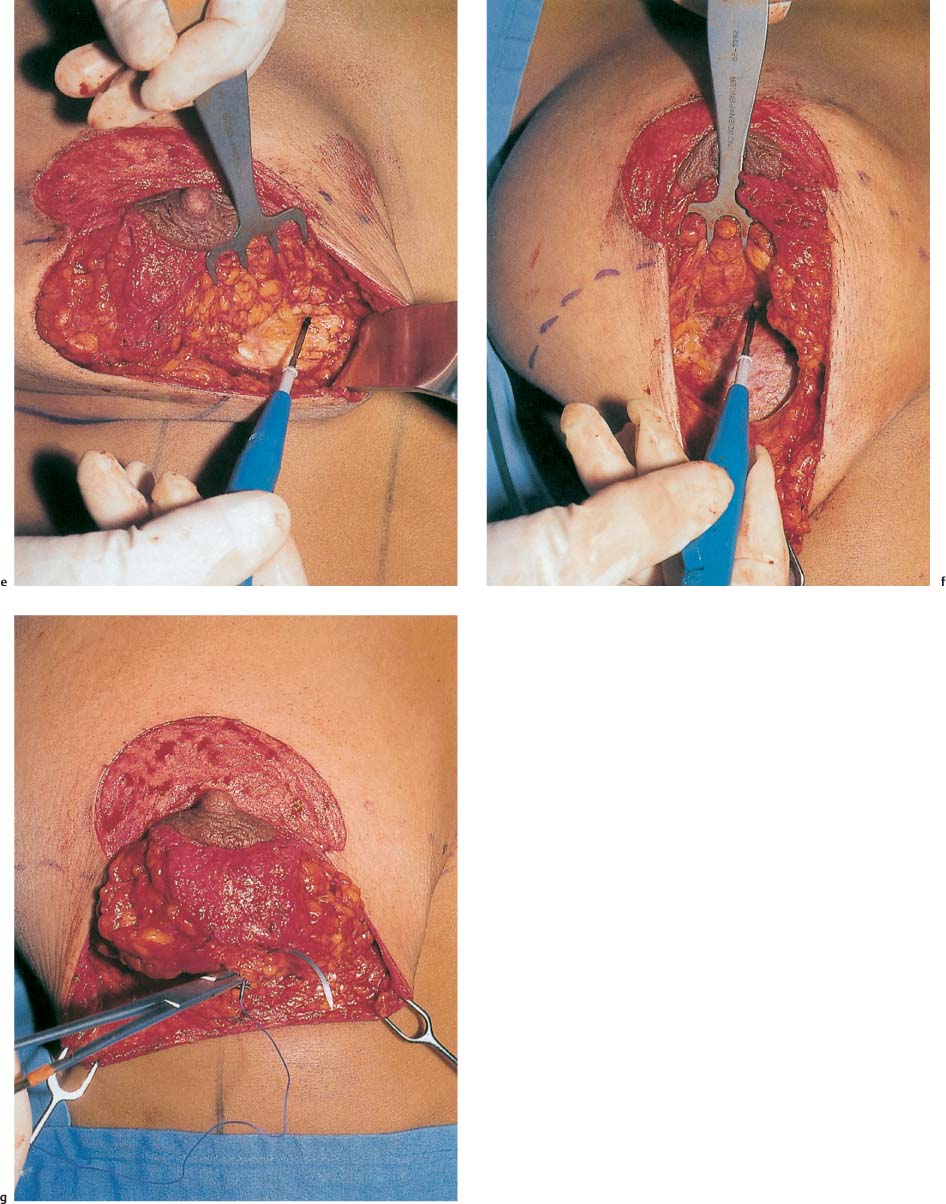
Subcutaneous dissection extends over both inferior quadrants into the inframammary fold. Here the tissue is incised down to the muscle on the chest wall.
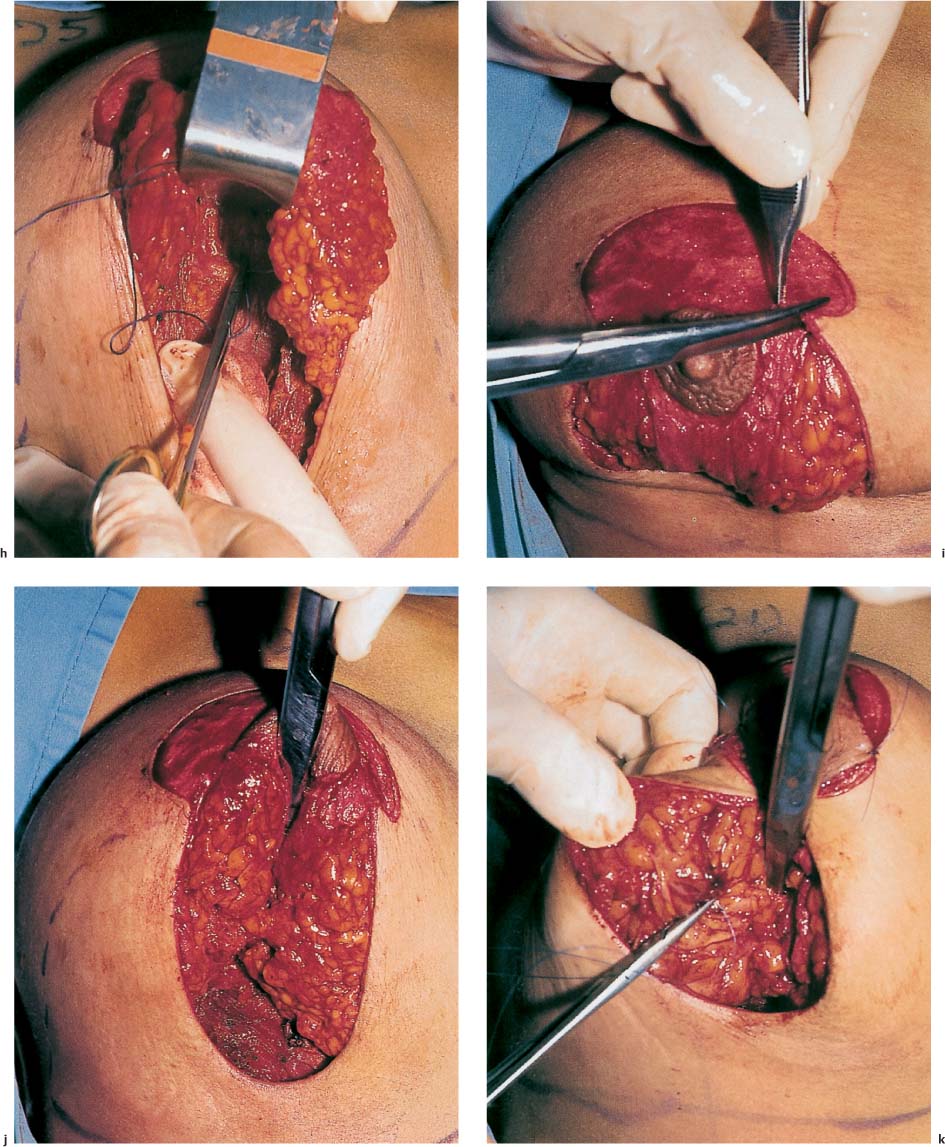
Next, the (already de-epithelialized) superiorly based nipple pedicle is elevated. The length and width of the flap vary depending on the individual findings; approximately 6–7cm length is incorporated below the nipple. After the skin incision, a 2-cm thick layer of the inferior part of the nipple flap is clamped with two ring forceps. A scalpel or electrocautery unit is used (with caution) to lift the flap off the underlying glandular tissue. Dissection then proceeds vertically around the entire flap, slightly beveling away from the flap. The flap is then elevated from the parenchyma obliquely as far as the upper margin of the areola. Depending on the flap length, it should not be more than 1.5–2.0 cm thick, so that it can be moved superiorly without tension. It is important that the superior portion of the flap should be neither too thin nor too thick. If it is too thick, it will impede invagination of the nipple flap. Surgeons sometimes dissect a flap that is too thick, often out of concern about potentially insufficient blood supply to the areola. However, subsequent perfusion disorders are mostly the result of vascular congestion in the pedicle, which is folded under tension, rather than actual hypoperfusion due to disrupted arterial supply. If the dissected flap is too thick and direct excision appears too risky, liposuction of the pedicle can reduce the flap thickness without significant tissue trauma. Athin cannula measuring 2 mm in diameter is used.
The next step involves dissecting the central tissue of the gland off the chest wall or pectoralis muscle. Subglandular dissection begins at the level of the inframammary fold. After the tough connective tissue attachment of the glandular tissue has been cut at the lateral border of the pectoralis muscle, dissection continues bluntly up to about the third intercostal space. The gland is raised to its superior margin over a 6–8-cm wide central tunnel. Central dissection allows the breast to move superiorly, as a type of overcorrection.
Excess parenchyma is mainly removed from the central and inferior portions of the breast. Starting at the cutaneous incision lines, the medial and lateral parenchyma is incised down to the chest wall. This also forms the two lateral pillars, which will be approximated later in the operation. Depending on the extent of reduction necessary, the parenchyma may also be resected posteriorly from the lateral pillars. The lateral pillars must be shortened if they exceed 6–7 cm in length. During resection of the central portion of the breast, the breast tissue behind the nipple is also thinned. This technique does not permit reduction of breast tissue in the superolateral or superomedial breast quadrants. This is a potential drawback, especially in patients with a history of cancer. An alternative reduction technique needs to be chosen if parenchymal resection is necessary in the superolateral quadrant.
After sufficient hemostasis, the mastopexy suture is placed. Slowly-absorbing suture material (e. g., Biosyn 0) is used. A deep suture is placed through the pectoralis muscle at the upper border of the breast parenchyma and opposite it at the upper limit of the parenchymal excision, usually at the level of the superior margin of the areola. The opposite suture in the parenchyma should not be placed much lower, as it otherwise leads to indentation of the areola. Correct placement of the suture is checked with the patient in the semisitting position. The superior displacement of the breast should now be clearly evident at the upper pole; if it is not, the elevation of the breast parenchyma has to be corrected.
The nipple–areola complex is moved superiorly by affixing the upper border of the areola with absorbable 4–0 suture material at the upper border of the de-epithelialized skin.
The next step, approximation of the breast pillars, is another important part of achieving proper breast contour and shape. Absorbable 0-sutures are placed through the breast pillars (which have been shortened to 6–7 cm). The sutures are placed through the parenchyma and pulled through the subcutaneous fatty tissue. The desired breast shape can be achieved by adjusting tension on the threads. Overcorrection is desirable. Although inexperienced surgeons are sometimes initially worried about a breast that appears too high with a slope that seems too sharp, such concerns are unwarranted. Fine adjustments in breast contouring can be made using 3–0 suture material.
Preliminary approximation of the skin margins can reveal where subcutaneous dissection may still be needed. Some dimpling is acceptable, and dissection is not always necessary. More pronounced puckering should be released in the subcutaneous tissue with scissors.
Tightening of the skin (and reduction of breast volume) has now visibly raised the breast and thus the inframammary fold. The lower limit of the vertical skin incision should therefore also be fixed to the lower border of the breast so that the final scar is not below the inframammary fold (not mandatory).
Drains are placed inferolaterally or in the axilla. The second subdermal suture is then placed at the lower border of the areola.
The wound is then closed and excess skin tightened. First, a running subcutaneous suture with 2–0 or 3–0 absorbable suture material is placed in the lower border of the wound and breast, in order to secure it here and pull the skin superiorly over the gland. One or two more evenly-spaced stitches are placed along the margins of the skin to secure it to the breast. Excess skin should be as evenly distributed as possible to help improve the postoperative results and aid healing. Finally, an intracutaneous suture with absorbable 4–0 suture material is placed. Afterward, the areola is sutured in layers, with subdermal and intracutaneous sutures.
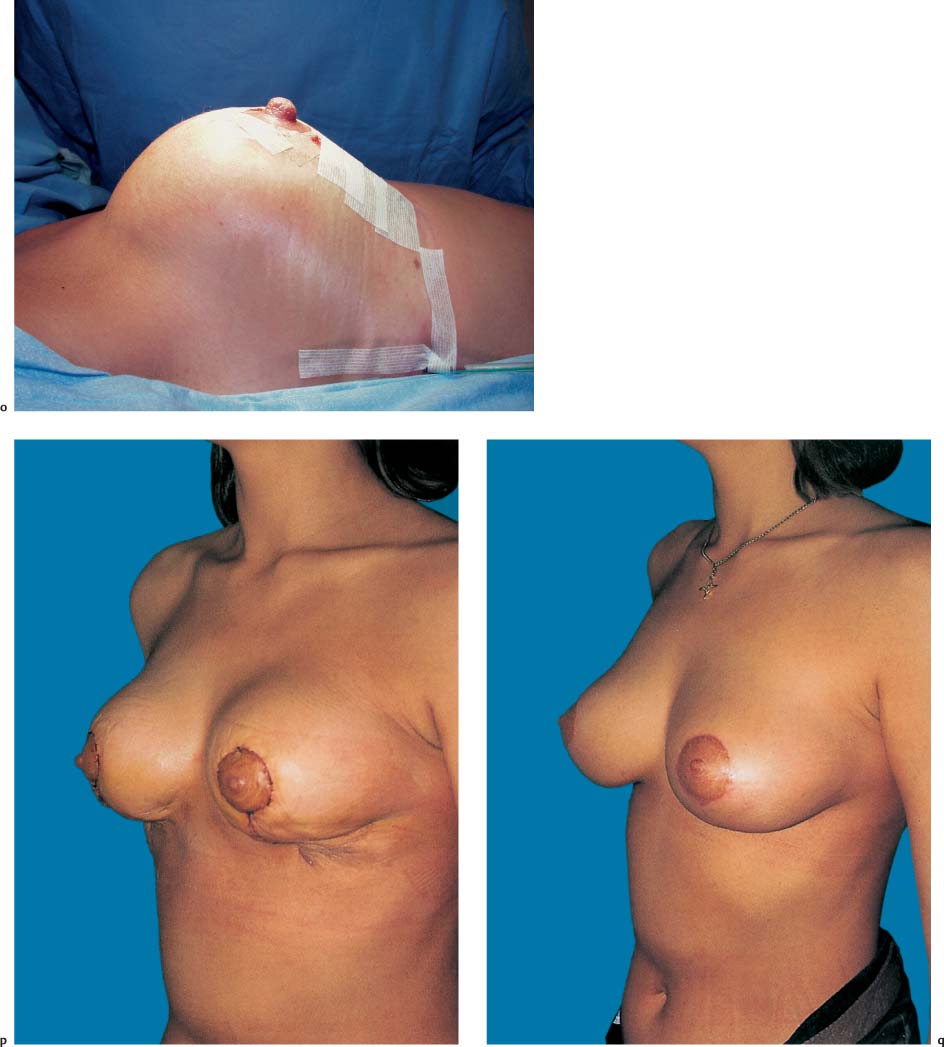
At the conclusion of the procedure, the upper portion of the breast is rounded, and the lower part below the areola is flat. The breast thus appears to be upside down on the chest wall.
A sterile, elastic pressure bandage is applied around the chest. It is removed after 1–2 days and replaced with a compression brassiere, which is worn continuously for 2–3 weeks.
Related posts:





Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


