3 Augmentation Mammaplasty
Breast augmentation with implants has become one of the most commonly performed plastic surgery procedures, and the numbers of procedures are increasing. The Breast Implant Registry in the United States lists a fourfold increase, from approximately 50 000 in 1995 to approximately 250000 in 2005, with a trend toward larger implant sizes. Twenty years ago, the average fill volume was approximately 150mL. Today, the average implant volumes are 250 mL in Germany and 380 mL in the United States.
The media are certainly partly responsible for this trend in promoting the image of the attractive, self-confident, desirable woman as one who is tall and slender but nevertheless possessing voluptuous feminine curves. What is usually kept secret in some countries is literally put on display in others. In Brazil, for instance, it is regarded as being desirable for the breasts to appear obviously artificially enlarged.
It seems unlikely that plastic surgery was involved in creating this need. It is more likely that, over the years, plastic surgery has been able to offer improved products and surgical techniques to meet ademand that already existed anyway. In addition, the high level of medical safety of this elective procedure makes it possible for physicians to take responsible decisions—which are still the highest priority, despite increasingly service-oriented attitudes in the public sphere.
What was previously a technically “simple” operation using an implant that “always” measured 150 mL and was “always” placed in a subglandular or subpectoral position, inserted through an incision that was “always” made in the inframammary or axillary fold, has developed into a far more technically complex procedure, particularly due to the increase in implant volumes. While implant volumes of up to 150 mL usually do not require preoperative planning, larger implants require careful consideration of the resulting change in breast shape. This applies in particular to the level of the inframammary fold, which should be lowered in patients with true breast hypoplasia. Otherwise, the implant would be placed too high on the chest wall, producing high cleavage that would give the breast an unnatural shape.
For this reason, preoperative planning of the type and position of the incision, as well as of the type and position of the implant, is critical for achieving an optimal aesthetic result.
Choice of Implant
Even in the early stages of the development of silicone implants, “anatomically” shaped implants were offered as an alternative to round implants. However, the shape of these implants was not very stable, due to the watery consistency of the silicone gel. The development of a cohesive (highly cross-linked) silicone gel made it possible to create an implant that would permanently retain its shape (although “anatomical” implants have been available on the market for many years). One drawback of using the firmer gel was a less pleasing feel, since it made the implant harder. While there has been progress with regard to the implants available, surgeons still need to familiarize themselves well with the products supplied by all manufacturers in order to select the best option.
Nowadays, plastic surgeons face a very wide range of possible implant sizes and shapes supplied by various manufacturers. Depending on the needs of the individual patient, the appropriate product can (and must) be chosen in order to achieve the optimal aesthetic result. It is therefore essential to develop a surgical plan before the operation. The following questions and requirements should provide a basis for planning.
What is the proposed implant volume? This should be discussed with the patient and decided before the operation. Even if the exact volume cannot be definitively determined preoperatively, an approximate volume should be determined. Given that most patients have difficulty envisioning the change in breast size produced by an implant, most preoperative counseling deals with the issue of appropriate implant volume. A useful rule of thumb is that 200 mL is roughly equal to one cup size. The average implant volume for breast augmentation used in some European countries is 250 mL. It may be useful to have implant sizers on hand that the patient can insert into a thin brassiere underneath a T-shirt to give her a realistic idea of the degree of augmentation that can be achieved. Previewing photos of patients who have undergone the operation is also helpful during counseling.
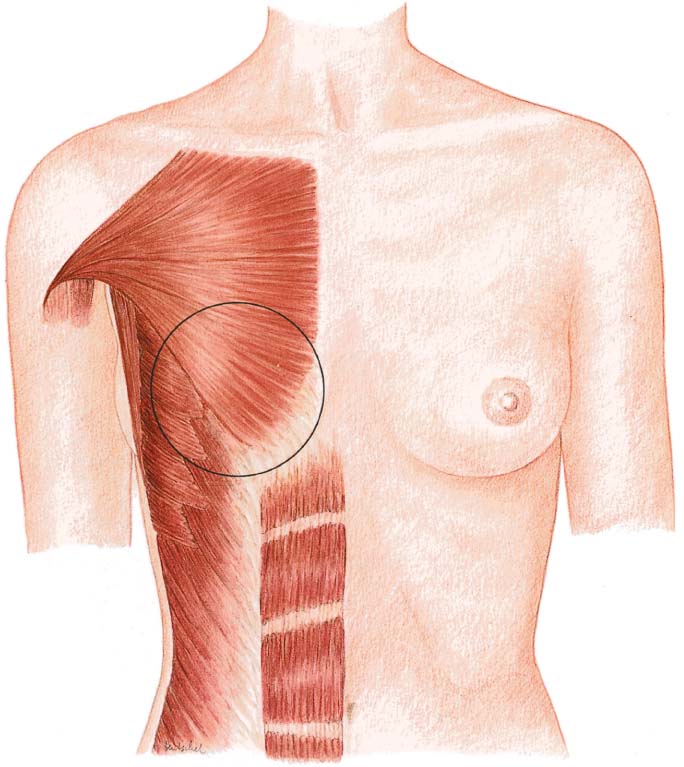
The base of the implant should not be wider than the base of the breast. Otherwise, the implant may develop creases that will become palpable later on, necessitating revision surgery. The base of the breast is measured (with a slide caliper) as the distance from the medial (parasternal) border to the tail of the breast in the anterior axillary line (generally 10–14 cm). Some authors subtract the tissue thickness of the breast from the measured breast base, using the pinch test (normally 2 cm) to determine the maximum implant diameter. This technique cannot always be used, however—especially in small-breasted patients who desire a large-volume implant. Such patients should be advised that the lateral margin of the implant would be more palpable than normal. As a general rule, the diameter of the implant base should be less than or equal to the breast base.
Several parameters are used to determine the choice of appropriate implant shape:
— Current breast shape
— Desired change in breast shape
— Desired volume
— The patient’s height
— “Individual” parameters
In principle, it has to be borne in mind that the smaller the actual breast volume, the more the implant and its shape will contribute to shaping the breast. For example, an implant inserted after subcutaneous mastectomy will largely define the shape of the reconstructed breast, whereas even a heavily contoured anatomical implant in a larger-breasted patient will not significantly alter breast shape. In actual practice, anatomical implants with a volume of 150 mL or less generally have little effect, so that in such instances there is little point in using this type of implant. The effects of anatomical implants begin to be visible at fill volumes of about 200 mL. There is no standard “recipe” for selecting the most appropriate implant from the abundance of available products. Nonetheless, the parameters listed above can provide the surgeon with a better idea as to which implant is best suited to a given patient’s wishes.
In true hypoplastic breasts, anatomical implants have the advantage of counteracting excessive fullness of the “upper pole,” whereas round, high-projection implants are better in ptotic breasts because they add fullness to the generally hypoplastic upper quadrants.
Some patients desire a strongly enhanced cleavage, and in these patients round implants are more suitable than anatomical ones. For the most “natural” breast shape, anatomical implants with moderate projection are considered more appropriate.
In taller women, implants should also be longer, thus emphasizing the cleavage as well. In smaller women, implants with a smaller longitudinal diameter may be used.
The desired volume also influences implant shape. After a certain level, greater volumes are achievable only with greater projection, since—as mentioned above—the diameter of the implant base should not exceed that of the breast base.
Individual tissue parameters should also be considered. Even in a large breast, for example, the shape of the implant may contribute significantly to breast shape if the tissue itself is “soft.”
Although the development of different implant types and shapes complicates the plastic surgeon’s task, there is a major advantage in being able to tailor the implant to the individual patient and thus achieve an optimal outcome.
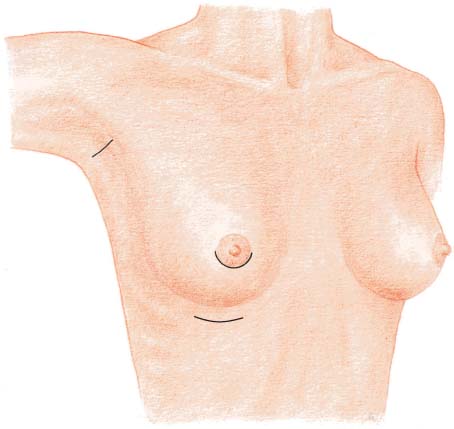
Choice of Incision
Breast augmentation can be performed using an axillary, periareolar, or inframammary approach (in our view, the periumbilical approach is not worthy of discussion). The choice of incision depends on individual patient’s anatomy and wishes, as well as the surgeon’s experience. It is therefore advisable to avoid using just one type of incision.
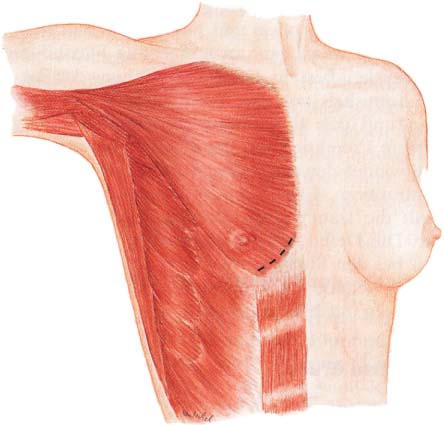
Periareolar Approach
The periareolar incision is highly versatile. If the areola is of normal size, the periareolar approach provides good exposure of the surgical site, with central access to the implant pocket. The pocket can be developed in the subglandular or submuscular plane. The perioareolar incision is also a good option if the inframammary fold needs to be lowered (e. g., if it is high and constrictive). A periareolar incision is also a good choice in patients undergoing a small mastopexy (for mild ptosis).
The perioareolar incision is also recommended in patients with tubular breast deformity.
If the areola is very small, the perioareolar incision may not be large enough. In women with a strongly pigmented areola, a white scar may remain and it is therefore advisable to place the incision closer to the border rather than directly in the areola.
Some surgeons prefer to carry the incision across the areola, cutting around or across the nipple.
From the skin incision, the glandular tissue is cut vertically. Care should be taken that the portion of the gland located below the incision is not too small (which can easily happen if the incision is aimed too far inferiorly), in order to ensure good implant coverage.
Subcutaneous dissection along or around the gland obscures exposure of the surgical site and is not recommended.
After the implant has been inserted, the divided breast tissue should be sutured anteriorly and posteriorly to keep the implant from “prolapsing” into the breast parenchyma.
Related posts:






Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


