37. Correction of the Tear Trough Deformity
Soft tissue depressions at the lid-cheek junction represent some of the most challenging, and difficult to correct, age-related deformities of the periorbital region.
The term “tear trough deformity” was first coined by Flowers and refers to the development of visible depression along the medial third of the lower lid. 1
Contemporary use of the term tear trough deformity refers to a variable spectrum of soft tissue deformities across the lid-cheek junction that are a direct result of the interplay of complex, age-related changes that occur in the lower lid and midcheek.
Correction of these deformities may therefore include procedures directed at rejuvenating both the lower lid and midcheek areas depending on their severity.
Terminology
Nasojugal groove: Natural sulcus directly overlying the medial one third of the inferior orbital rim.
“Tear trough deformity” refers to a prominent nasojugal groove.
Palpebromalar groove: Prominent depression at lid-cheek junction inferolateral to nasojugal groove.
It is confluent with nasojugal groove.
Midcheek: Region of cheek medial to a line extending from the frontal process of the zygoma to the oral commissure and from the lower lid to the nasolabial fold.
Prezygomatic part: Overlies the skeleton of the midcheek.
Infrazygomatic part: Covers the vestibule of the oral cavity.
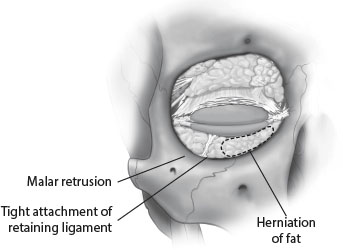
Tear trough triad: Association of several anatomic characteristics giving rise to a prominent tear trough (Fig. 37-1).
Herniation of orbital fat
Tight attachment of the orbicularis retaining ligament along the arcus marginalis
Malar retrusion
Grading System
An objective system for grading the severity of deformity has been proposed by Barton et al. 3
More severe deformities are characterized by changes not limited to the nasojugal groove.
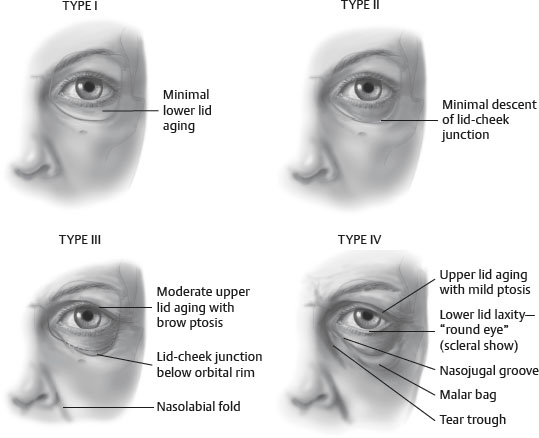
Classification of Midface Morphology
Classification system incorporating the global changes occurring at the eyelid-cheek junction and midface. 4
Anatomic Considerations Contributing to Deformities at the Lid-Cheek Junction
Periorbital and midcheek anatomy has been reviewed in detail in Chapter 22.
Medial Fat Pad
Bulge extends anteriorly in a position superior to the inferiomedial orbital rim.
Visually, this creates an apparent increase in the depth of the nasojugal groove.
Inferior descent is limited by the tight, direct attachment of the orbicularis to the medial orbital rim.
Senior Author Tip:
The medial fat pad can be quite vascular and care must be taken in the dissection of this fat pad to prevent vascular injury that retracts into the orbit, which can result in a retrobulbar hematoma.
Central Fat Pad
Inferior descent over the central orbital rim is not restricted and therefore occurs progressively.
Inferior descent distends the orbicularis retaining ligament (ORL) inferiorly several millimeters.
Inferior descent and distention of the ORL creates an apparent increase in the depth as well as the length of the nasojugal groove.
With increasing magnitude of descent, a sulcus develops lateral and inferior to the central fat bulge—the palpebromalar groove.
Palpebromalar groove creates a visible demarcation of the lid-cheek junction laterally.
Senior Author Tip:
The medial and lateral fat pads are separated by the “arcuate expanse.” This is a fibrous extension from the arcus marginalis inferolaterally extending medially to the medial canthal tendon. It is a retroseptal structure which functions to prevent overaction of the inferior oblique muscle.
Festoons
Can be multifactorial
Skin and skin/muscle festoons can be addressed by redraping the skin and/or skin/muscle in a more anatomic position.
Dermal festoons are more difficult to treat and are related to the interdigitation of the orbitomalar retaining ligament with the subdermal collagen as the direction of the collagen fibers change from circumocular in the eyelid to more vertical in the cheek.
Senior Author Tip:
It is very important to identify festoons and their etiology prior to surgery so that they can be addressed and patient expectations for swelling in this area can be properly addressed.
Related posts:



Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


