33. Browlift
Ideal Facial Aesthetics
Forehead
The forehead, including the eyebrows, comprises the upper third of an aesthetically proportioned face.
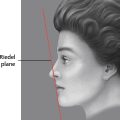
The anterior hairline is typically 5-6 cm superior to the eyebrow level.
Transverse, vertical, oblique, and glabellar forehead skin lines should be subtle and soft and rarely present without facial animation.
Dynamic rhytids are skin lines present with facial animation. These rhytids are amenable to chemodenervation with botulinum toxin.
Static rhytids are skin lines present without facial animation but with sustained facial muscle hypertonicity. Treatment of deep static rhytids may require surgical treatment with redraping of the involved skin.
Ideal Eyebrow Shape and Position will Vary by Gender
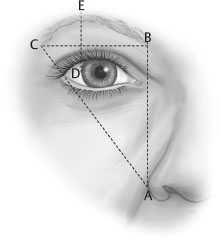
Female (Fig. 33-1)
The eyebrow forms a gentle arch that peaks at the junction of the middle and lateral thirds just above the lateral limbus of the eye.
Eyebrow level is typically 3-5 mm above the supraorbital rim.
Medially, the eyebrow begins at the level of a perpendicular line extending from the medial canthus through the outer edge of the ipsilateral nasal ala.
The lateral end of the eyebrow is positioned slightly higher than the medial end and extends laterally to the level of an oblique line that passes through the outer edge of the ipsilateral nasal ala and the lateral canthus.
The medial end of the eyebrow is club shaped, whereas the lateral end is tapered.
Male
Eyebrow level is at or near the level of the supraorbital rim.
The shape is relatively horizontal with minimal arching or peaking.
Effects of change in position of the eyebrow segments for males and females
The medial eyebrow segment projects an angry appearance when this segment is depressed and a surprised appearance when it is elevated.
The lateral eyebrow segment projects a sad and tired appearance when this segment is depressed and a quizzical appearance when it is elevated.
Anatomy
Soft Tissue Layers of the Forehead
Skin
Subcutaneous tissue
Superficial plane of the galea aponeurosis
Frontalis muscle
Deep plane of the galea aponeurosis
Loose areolar tissue
Periosteum
Galea Aponeurosis
At the origin of the frontalis muscle from the galea aponeurosis at approximately the level of the frontal hairline, the galea aponeurosis splits into a superficial and a deep layer, and these layers encase the frontalis muscle.
In the midforehead region, the deep galeal plane splits again to envelop the galeal fat pad, which extends down over the lower forehead to the eyebrow level.
Deep to the lower third of the galea fat pad in the lower forehead region, the deep galeal plane splits again to form the glide plane space, located under the transverse head of the corrugator muscle as this muscle passes through the galeal fat pad area.
The deepest layer of the deep galeal plane extends inferiorly to the supraorbital rims and bonds with the periosteum over a 2 cm wide horizontal strip just cephalad to the supraorbital rims.
Bony Anatomy, Zones of Fixation, and Retaining Structures
The supraorbital rim is palpable above the upper eyelid and serves as a fixed position from which to assess eyebrow ptosis.
The temporal ridge along the lateral margin of the frontal bone is produced by the temporal fusion line of the skull. The temporal ridge delineates the forehead area from the temporal fossa area.
The soft tissues of the forehead are fused to the underlying bony skeleton in specific areas, and these areas must be adequately released from bone to effectively reposition the soft tissues.
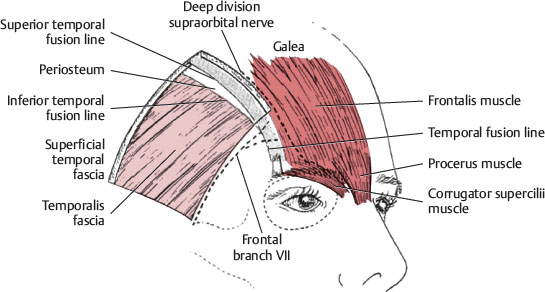
Just medial to the temporal ridge, the layers of the deep galeal plane of the forehead and scalp bond with the underlying periosteum and fuse to bone within a 5-6 mm wide zone of fixation (Fig. 33-2).
The orbital ligament is a fibrous band that secures the superficial temporal fascia to the superolateral orbital rim near the lateral end of the eyebrow (see Fig. 33-6).
Over the lower 2 cm of the frontal bone just above the supraorbital rims, the deep galeal plane and periosteum are fused together and fixed to bone, as described previously. Otherwise, the overlying skin, subcutaneous tissue, and frontalis muscle move freely over the orbital rim without direct attachment to bone.
The medial eyebrow segment is less mobile than the lateral segment because of the anchoring effect produced by the supraorbital and supratrochlear nerves that exit bone and pass through the overlying medial frontalis muscle.
Senior Author Tip:
Some authors have described a brow-retaining ligament 7 under the medial end of the eyebrow, but I think no ligaments are present between bone and dermis under the medial end of the eyebrow that restrict movement of the medial eyebrow.
Muscles of the Forehead
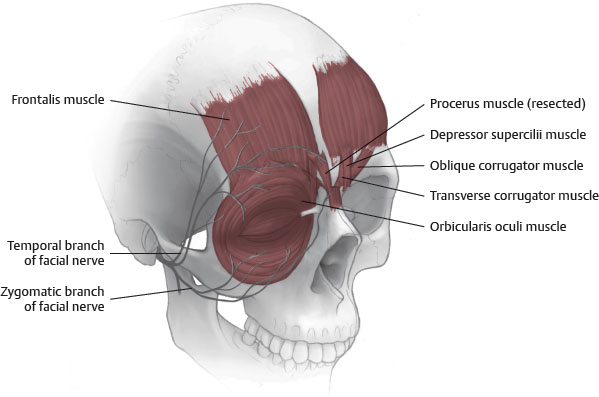
Frontalis
Origin: Galea aponeurosis (at approximately the level of the typical frontal hairline)
Insertion: Primarily interdigitates with the orbicularis oculi and procerus muscles, which insert into the dermis under the eyebrows
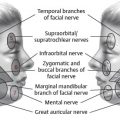
Innervation: Frontal (temporal) branch of facial nerve (CN VII)
Action: Eyebrow elevation primarily produced by suspending the superior orbicularis oculi muscle. Muscle contraction produces transverse forehead skin lines.
Corrugator Supercilii
Origin: Superomedial orbital rim
Insertion:
Oblique head inserts into dermis under the medial head of the eyebrow.
Transverse head inserts into dermis under the middle third of the eyebrow.
Note:
Clinically, the two heads of the muscle are often not clearly delineated, because the fibers sometime rapidly coalesce into a singular corrugator muscle mass.
Innervation:
Oblique head
Zygomatic branches of the facial nerve
Transverse head
Frontal branch
Action: Movement of the medial eyebrow medially and downward, which produces vertical and oblique lines in the glabellar skin
Procerus
Origin: Dorsal surface of the nasal bones
Insertion: Dermis in the glabellar region and interdigitation with the inferior medial fibers of the frontalis muscle on each side
Innervation: Frontal and zygomatic branches of the facial nerve
Action: Medial eyebrow depression, which produces transverse rhytids at the nasal root
Orbicularis Oculi
Origin: Various structures in the medial canthal region
Insertion: Dermis under the medial brow and the lateral palpebral raphe
Innervation: Zygomatic branch of the facial nerve
Action: Flat, circumferential sphincter muscle of the eyelids that primarily provides eyelid closure
The medial orbital portion depresses the medial brow and contributes to oblique skin line formation in the glabellar area.
The lateral orbital portion depresses the lateral brow and creates radial, lateral periorbital rhytids with contraction (“crow’s-feet”).
Depressor Supercilii
Origin: Superomedial orbital rim, where it is often described as a portion of the medial orbicularis oculi muscle
Insertion: Dermis of the medial eyebrow (medial to the dermal insertion of the fibers from the orbicularis oculi muscle and anterior to the dermal insertion of the oblique head of the corrugator supercilii muscle)
Innervation: Zygomatic branch of the facial nerve
Action: Medial brow depression
Vascular Supply to the Forehead
Supply is from branches of both the internal and external carotid arteries
Centrally, supraorbital and supratrochlear arteries arise off the internal carotid artery from the ophthalmic artery.
Laterally, frontal branches of the superficial temporal artery arise from the external carotid artery.
Vast communications exist between these vessels of the forehead and those of the posterior scalp, providing rich vascularity.
Sensory Innervation
Supratrochlear Nerve
A branch of the ophthalmic division of the trigeminal nerve (V1)
Emerges from its bony foramen within the medial orbit along with the supratrochlear artery
Pierces the medial end of the corrugator muscle and supplies sensation for the medial forehead skin on each side
Supraorbital Nerve
A branch of the ophthalmic division of the trigeminal nerve (V1). The supraorbital nerve trunk emerges from its bony exit point, the supraorbital notch (or foramen), along with the supraorbital artery.
The supraorbital nerve trunk divides into a superficial and deep division.
Superficial division
Pierces the frontalis muscle after dividing from the supraorbital trunk and travels cephalad, first within the frontalis muscle and later in the subcutaneous plane to the frontal scalp level
Supplies sensation to the dermis of the forehead skin and anterior scalp on each side
Deep division
After dividing from the supraorbital trunk, the deep division initially runs superolaterally over the surface of the periosteum.
When the deep branch is almost at the temporal ridge, it turns cephalad and runs parallel with the temporal ridge to the scalp, remaining within 0.5-1.5 cm medial to the ridge.
Along this course, this branch progressively passes up through the plane of the deep galea to terminate in the dermis of the frontoparietal scalp.
The deep division passes across the forehead and provides only a few tiny branches to periosteum in this part of its course.
Note:
Coronal incisions made through the galeal plane always transect the deep branch at the level of the incision.
Caution:
The deep division can also be injured over the lower forehead during dissection in the subgaleal plane, because this nerve moves from the surface of periosteum into the deep galea plane at a level approximately 2-3 cm above the orbital rim.
Tip:
In about 10% of patients, the deep division of the supraorbital nerve exits the frontal bone from a foramen lateral to the supraorbital notch. This foramen is usually just medial to the temporal ridge and just superior to the laterosupraorbital rim. Surgeons must be prepared for the presence of the aberrant course of the deep division and prevent inadvertent transection, which would produce dysesthesia or anesthesia of the ipsilateral frontoparietal scalp.
Patient Evaluation
History Should Include
Age
Gender
Bleeding tendency in the past
Medications, including herbal medicines
Other medical comorbities
Patient’s expectations for skin smoothness and eyebrow shape and position
Analysis of the Forehead Should Include
Eyebrow position, shape, and symmetry
Presence of dynamic and/or static rhytids
Presence of upper lid ptosis or dermatochalasis
Hairline
See the Surgical Techniques section for descriptions of techniques mentioned here.
High hairline typically describes a brow-to-hairline distance of >5 cm in women and >6 cm in men. In these cases, an anterior hairline technique to prevent further elevation of the hairline should be considered.
Low hairline typically describes a brow-to-hairline distance of <5 cm in women and <6 cm in men. For these cases, a coronal incision should be considered to allow elevation of the hairline.
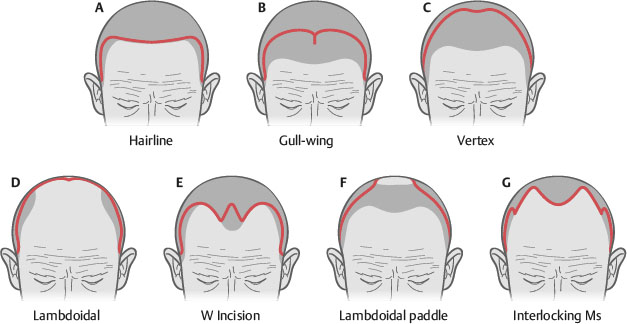
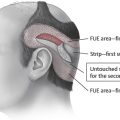
Atypical hairline patients are often challenging, with thin or balding hair. Often, small incisions for endoscopic-assisted procedures or custom incisions are made for these patients (Fig. 33-4). For males who have residual hair in the temporal scalp area, the limited incision procedure is often appropriate.
Guyuron and Lee 12 have published a treatment algorithm based on forehead elongation, forehead lines, and brow ptosis (Fig. 33-5).
Related posts:



Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


