30 Facial Contouring Using Fillers
Pearls
Contouring or augmentation of the facial skeleton with fillers is one of the most subtle but powerful nonsurgical treatments.
An E-plane, which is a line drawn from the tip of the nose to the tip of the chin, is an important guideline for contouring the lateral profile. In the frontal view, a heart-shaped face is the preferred facial contour.
To treat fine wrinkles, volume replacement just under the dermis with soft filler that has lower elasticity is effective.
For structural facial contouring, a larger volume of filler is required in most cases. Hard filler gels such as CaHA filler, PCL filler, and particle type HA filler are preferred.
When a patient is not sure about the proper filler type and its effect at initial consultation, use of normal saline or HA filler is recommended. If the patient is satisfied with the results of filler injection but wants to avoid repeated injections, long standing filler can be applied.
Special caution should be taken when injecting filler into thin-skin areas such as the eyelid, periorbit, and fine wrinkles on the cheek area because of possible nodule formation and color change. In this case, it is better to inject a small amount multiple times or use soft filler by canula.
The forehead, temple, cheek, chin, nose, nasolabial fold, and jaw line are common filler injection sites for facial contouring.
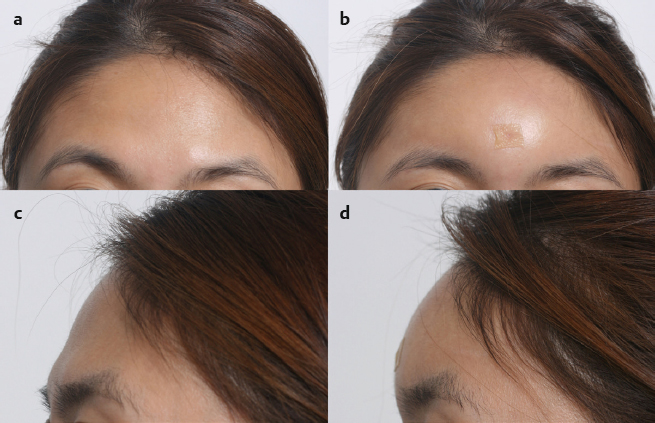
For forehead contouring, 1.5 to 3.0 mL of filler is injected under the muscle layer using the radial fanning technique through one entry point midway between the eyebrows.
Commonly used fillers for nasal augmentation are CaHA filler, Restylane (Galderma), and Perlane (Merz). Submuscular injection using the linear threading technique and subcutaneous injection using the serial puncture technique are usually combined.
In aged patients, more extensive volumetric replacement is needed and other, concomitant lifting procedures such as ultrasound lifting or surgical face lifting would be helpful.
Hydro lifting, in which hyaluronic acid is directly injected into the dermis layer of the skin, is useful in people who have serious dry skin or who want more elastic and hydrated skin.
Introduction
Filler is used in the East Asian face for diverse aesthetic purposes: facial contouring, including augmentation of certain facial areas; treatment of aging lines such as wrinkles and prominent crease1; and dermal hydration. Many Asians have small chins, flat noses, and depressed foreheads compared with Caucasians.2 To augment those areas, insertion of implants such as silicon, Gore-Tex (W. L. Gore), Medpor (Stryker), cartilage, bone, or fat grafts is commonly used. Because many patients want a simple and safe procedure instead of surgeries, filler can be an alternative option to augment those areas.
In most cases, the augmentation results from filler are similar to those from implant surgery except for its longevity. Because filler injection changes the soft tissue structures and not the bony structures, the size and the shape of the facial skeleton and thickness of soft tissues are fundamental consideration factors for successful results. When considering augmentation of certain facial areas, the “esthetic plane” (E-plane) is an important guideline for a pleasing facial profile.3,4 The E-plane is a line drawn from the tip of the nose to the tip of the chin. To have a pleasing facial profile for the average Caucasian face, the lower lip should be 2 mm behind the line, and the upper lip 4 mm behind the line, with variations being normal for patients of different ethnic backgrounds. Many physicians, however, feel that the ideal E-plane of an Asian face is quite different from that of a Caucasian face. For an Asian face, the lower lip and upper lip should be near the E-plane. The jaw is also important to complement the whole face. If the jaw is pulled in or is extending too much, it disrupts the overall harmony of the aesthetic standard. If the patient’s profile appears very convex, the chin and the forehead area can be augmented by fillers; for a concave profile, fillers can be placed in the nose, the paranasal area, and the anterior cheek.
While the E-plane is a guideline for contouring the facial profile, a heart shape is considered the preferred facial contour by Asians in the frontal view. It is characterized by higher and fuller cheeks, raised nasal profile, and smaller chin contributing to a smooth facial convexity. Traditionally, it is considered ideal when the ratio between the upper, mid-, and lower face is equal or represented as 1:1:1. Recently, however, the “baby face,” in which the lower face part’s ratio is a little short of 0.8, has been receiving attention in the rejuvenation of the Asian face.
Dermal fillers can be an option for treatment of rhytides as well as for facial sculpting. Understanding the aging process is crucial to attain optimal results with facial rejuvenation by filler injection. Facial aging is the result of decreased thickness and elasticity of the skin, absorption of fat, and resorption of the bony skeleton. In addition, decreased adherence between the skin and subcutaneous tissue, muscle alteration, and sagging of soft tissues are present. Thus, just tightly retracting the facial skin through surgical intervention may be inappropriate in some patients because it can produce an unnaturallooking appearance. Replenishing facial volume and filling fine wrinkles with injectable fillers would be a better approach in these patients.
Recently, facial rejuvenation using the hydrofilling effect of hyaluronic acid (HA) filler has been employed for improvement of skin texture. Since the concentration of HA in skin decreases with aging, the skin’s elasticity and ability to hold water are decreased, leading to an increased tendency toward wrinkling and skin laxity, particularly in the facial skin. Because of their hydrophilic nature, HA fillers play a role as a dermal reservoir of hydration, by drawing water into the extracellular matrix in the dermis, resulting in hydration in the dermis and improvement of skin surface roughness and fine wrinkles.
Patient Consultation
During consultation, the patient will be informed of the potential risks with the filler injection. A detailed medical history should be taken, including prior injection procedures. Aspirin or Coumadin (Bristol-Myers Squibb) needs to be stopped before the procedure to prevent bleeding and bruising. Any patients with immunologic diseases such as lupus or scleroderma should take extra precautions as people with facial soft tissue atrophy can have problems.
The consultation and assessment should include the following:
Discussion of the patient’s expectations (duration of fillers, injection amount of fillers, patient’s aim and purpose)
Medical and surgical history, medical conditions, and drug allergies
Radiologic assessment (computed tomography [CT] scans or facial X-rays)
Preoperative and postoperative photography for evaluation and comparison
Computer-assisted simulation if available
In most cases, botulinum toxin and injectable fillers are inextricably linked. Concomitant botulinum toxin injection is beneficial as it prevents unwanted migration of injected filler by restricting excessive muscle movement, and also changes facial shape favorably.5 Therefore, it is essential to help the patient understand the benefits of combined botulinum toxin injection.
Filler Materials
A wide variety of filler materials are currently available, with a seemingly endless flow of new and emerging products. Table 30.1 shows detailed information on filler materials currently available. Among these fillers, the best and the safest products are hyaluronic acid (HA) fillers. There are two types of HA in terms of rheology or its particle shape: One is biphasic HA filler (Restylane) and the other is monophasic HA filler (Juvederm, Belotero). With a monophasic HA filler such as Juvederm, it is easy to inject without lumps or irregularity, but it is hard to use when contouring to form a shape with a narrow base and tall height. With a biphasic HA filler such as Restylane, it is easy to lay bricks (“brickwork”) into a form with a narrow base and tall height, but there is a high risk of lumps or irregularity. Molding is much more difficult with biphasic HA fillers but they can last longer and are more durable than the monophasic HA fillers. Over time, the injected HA gel is slowly absorbed into the surrounding tissues and disappears by a process called isovolumetric degradation.
Similar to HA-based products, calcium hydroxylapatite (CaHA, Radiesse, Merz) is also relatively inert, is very safe, and requires no skin testing prior to injection. In comparison to HA-based fillers, however, CaHA is not recommended for the treatment of very superficial wrinkles and creases. CaHA is more commonly used to augment deep creases and folds as well as contouring the cheek, chin, and forehead. Approximately 9 months after an injection, CaHA begins to undergo gradual enzymatic digestion, with complete disappearance of the aesthetic effect between 12 and 18 months. From the author’s experience, the volume starts to decrease within 1 month after CaHA injection.
Poly-Llactic acid (PLLA; Sculptra, Dermik Laboratories) and poly-caprolactone (PCL; Ellanse, AQTIS Medical) work by providing a delayed longlasting volumizing effect.6 However, multiple treatments (two or three sessions) are needed to achieve complete correction. Actually, Sculptra is not a volumizing filler, but a stimulator. The augmentation or contouring effects of Sculptra are not predictable either; therefore, it is not recommended for contouring purposes.
Procedural Techniques
Anesthesia
The topical anesthetic is not adequate; hence, it is recommended that the surgeon block the nerve locally or use tumescent solution for anesthesia before filler injection. The author prefers both. Epinephrine in the anesthetic solution helps to reduce bruising and prolong the anesthetic effect for a few hours. Lidocaine (mixed with epinephrine) is used for local nerve block. For a midface local block, the needle can be placed through an intraoral approach just above the canine around the infraorbital nerve area. The micro–nerve block technique can be useful for an injection of the lip area. For the micro–nerve block technique, small aliquots of anesthetic solution are injected along the mucosal border of the lip near the gingival sulcus. Micro-blocks have the advantage of not producing a deep regional anesthesia. However, this technique may take longer to perform and the potential for incomplete anesthesia is greater. The author prefers tumescent solution, which is prepared by mixing 100 mL of normal saline with 20 mL of 2% lidocaine and 1 mL of 1:100,000 epinephrine.
Selecting Needles
Dermal fillers may be injected using either a sharp needle or a blunt-tip microcannula (Fig. 30.1). A blunt-tip microcannula (also called a smooth-tip microcannula or a bluntneedle cannula) is a small tube (18- to 30-gauge), with an edge that is not sharp, designed for the atraumatic subdermal injection of fillers. Depending on the inner diameter, it can be used either for fat transfer, or for the injection of fillers such as HA, PCL, PLLA, CaHA, etc.
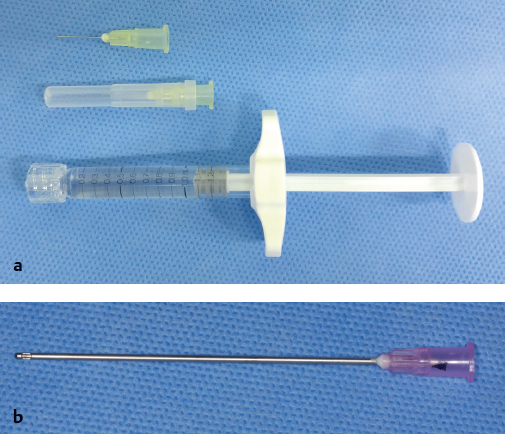
Each physician has specific preferences for injection instruments depending on the type of procedure being performed. For example, needles may be preferred for delicate correction of lines and wrinkles, while cannulas may be preferred for volume correction. Needles have the advantages of extreme precision of movement, the possibility of deep intradermal injection, and convenience when smaller injection volume is required. Disadvantages include pain, bruising, and possible vessel laceration. Cannulas cause less trauma, pain, and bruising and allow a large area to be treated at the chosen injection depth. Specific training is required to master the techniques of injection, and this is considered a disadvantage.
Usually a 50-mm-length, 27-gauge needle is used for the injection of Restylane. The author prefers a 70-mm 23-gauge microcannula since it can also be used to inject Ellanse, Restylane Sub-Q (large-particle HA), and monophasic HA fillers such as Juvederm and Teosyal (Teoxane Laboratories) as well.
Injection Techniques
Linear Threading, or Tunneling
Linear threading is a technique in which the needle is inserted into the skin and the filler is deposited in a linear fashion along the track as the needle is slowly withdrawn. Because this creates essentially a tunnel of filler, this is also commonly called the tunneling technique. Applied with a cannula, this is the most frequently used technique for the augmentation of the nose (Fig. 30.2a).
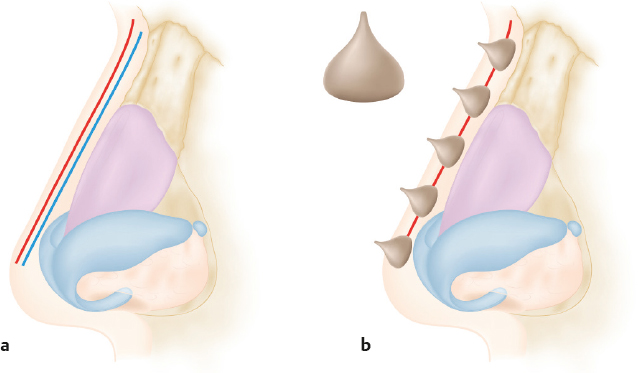
Serial Puncture
Serial puncture involves multiple injections positioned adjacently along the length of the wrinkle or crease. This technique makes many “chocolate Kisses”–like structures on the nose (Fig. 30.2b). It is imperative that these injections remain sufficiently close to form a relatively smooth, continuous line of augmentation (Fig. 30.3). In cases where there is a noticeable separation between the injection sites, posttreatment massage may help blend the filler.

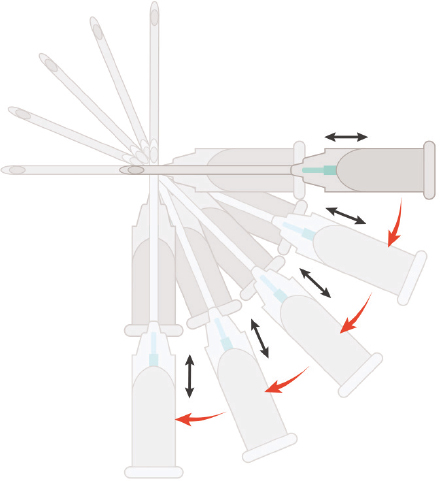
Fanning Technique
The fanning technique is performed for augmentation of a wide area such as the forehead, malar, and jowl regions (Fig. 30.4). Radial fanning is an extension of the linear threading technique.7 The filler is deposited in a linear line as the needle is withdrawn with a fan shape movement. Before the needle is actually removed from the skin, it is redirected and advanced along a new radial line. Multiple strokes will be needed to prevent irregularity after injection.
Self-Pistol Technique
The injection area is drawn with a pencil and the insertion points are selected in the center of the area to be augmented. After bolus injection under the fascia, molding is applied by simple compression on the injected area. This method is commonly used in temporal depression. Assessment is easy because it is not necessary to pre-inject with lidocaine solution in this technique.
Facial Contouring
Forehead
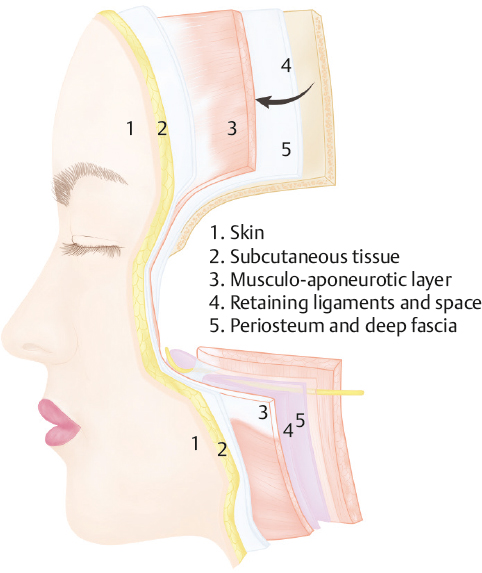
There are five layers on the forehead, composed of skin, subcutaneous tissue, aponeurosis, loose connective tissue, and periosteum, collectively called SCALP (Fig. 30.5).8 When injecting fillers to the forehead, the target layer differs according to the purpose of filler injection. To treat wrinkles, injectable fillers can be introduced to the dermal and the subdermal layers. However, to change the forehead contour, a deeper injection into the supraperiosteum and submuscular layer is preferred. In filler injection, a deep injection has a lower risk of lumps and irregularities. To prevent migration of filler gels, botulinum toxin is injected together with the filler in most cases.
When using a blunt needle, the entry points should be made before an injection. The author prefers to make one entry point midway between the eyebrows.9 Occasionally, the author makes one entry point at the center of the forehead (Fig. 30.6) since the midline approach is safer by avoiding damage to the blood vessels. Some doctors prefer to make two entry points on each side of the eyebrow, but this is not safe due to risk of injury to the supraorbital nerve and blood vessels. Also, the entry points on the eyebrow have a high risk of bacterial contamination from hair follicles of the eyebrows. For forehead contouring, 1.5 to 3.0 mL of filler is injected using the radial fanning technique. The fanning method is appropriate for placement of the product in the supraperiosteal layer instead of the subdermis or subcutaneous tissues because the bone can be a guide to control the injection depth.9 For contouring of the Asian forehead, CaHA and PCL fillers are preferred and 3 mL is used for the first session. Molding immediately after filler injection is easy and essential because it is hard to mold after the filler has settled down. For molding, a roller is used in this region.
Related posts:





Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


