30. Face and Neck Anatomy
Face and Neck Anatomy
Mastery of the three-dimensional anatomy of the face and neck is essential for safe and effective aesthetic surgery.
Anatomic variation is the rule, not the exception.
Soft Tissue Layers of the Face
The face is anatomically arranged in related concentric layers to create a balanced structure that produces facial movement.
Skin
Superficial fat
Superficial fascia (or superficial musculoaponeurotic system [SMAS])
Mimetic muscles
Deep fat and anatomic spaces (buccal space)
Deep facial fascia (parotidomasseteric fascia)
Deepest plane
The epidermis is composed of keratinocytes, melanocytes, and antigen-presenting Langerhans cells.
The dermis is rich in fibroblasts and type I collagen.
Dermal thickness is variable throughout the face and neck and is related to its function.
Thickness is usually inversely proportional to its mobility.
Eyelid dermis is the thinnest, whereas forehead and nasal tip dermis is the thickest.
Thinner dermis is more susceptible to deterioration and signs of aging.
Subcutaneous tissue 1 , 2 , 4 , 5
Comprises two components
Subcutaneous fat: Provides facial volume
Fibrous retinacular cutis: Binds dermis to the underlying musculoaponeurotic system
Retinacular cutis is the name given to the portion of a retaining ligament as it passes through the subcutaneous layer.
The proportion and orientation of these components are variable in different regions of the face.
Compact subcutaneous fat is present in specialized areas as in the lip and eyelid.
Regions of thick subcutaneous tissue have longer retinacular cutis fibers that are predisposed to weakening with age.
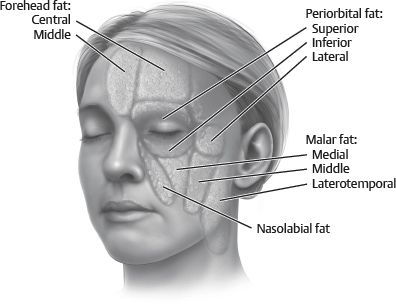
Subcutaneous fat compartments 1 , 2 , 6 – 10 (Fig.30-1)
Subcutaneous fat in the face is partitioned into distinct anatomic compartments and may not age as a confluent mass.
A youthful face has smooth transitions between compartments, whereas aging can lead to abrupt contour changes.
Shearing between adjacent compartments may contribute to soft tissue malpositioning.
Forehead
Central: Located in the midline region of the forehead. Bordered on sides by middle temporal compartment and inferiorly by the nasal dorsum
Perforating vessels from the supratrochlear artery travel through the septum that borders this compartment.
Middle temporal: On either side of central forehead fat. Inferior border is orbicularis retaining ligament, lateral border is superior temporal septum.
Laterotemporal: Connects lateral forehead fat to lateral cheek and cervical fat
Orbit
Superior: Bounded by the orbicularis retaining ligament as it courses around the superior orbit
Inferior: Thin subcutaneous layer immediately below the inferior lid tarsus
Lateral: Superior border is the inferior temporal septum, inferior border is the superior cheek septum.
Cheek
Superficial cheek compartment
Medial: Lateral to the nasolabial compartment. Superior border is orbicularis retaining ligament and the lateral orbital compartment.
Perforating vessels from the facial and infraorbital arteries are found within the medial limiting septum.
Facial vein is found on the deep surface of the medial cheek fat.
Middle: Anterior and superficial to the parotid gland
Perforating vessels of the transverse facial artery course within the middle cheek septum.
The plane between the middle and lateral cheek compartments can easily lead to into the deepest plane and buccal fat pad with associated neurovascular structures.
Laterotemporal cheek: Immediately superficial to the parotid gland, connects temporal fat the cervical subcutaneous fat
The lateral cheek septum is anterior to the laterotemporal compartment and contains perforating vessels from the superficial temporal artery.
Deep medial cheek compartment
Found deep to the medial and middle superficial cheek compartment and inferior to orbicularis oculi muscle
Orbicularis retaining ligament is superior boundary, SOOF is inferior boundary.
Nasolabial
Found anterior to the medial cheek fat overlapping jowl fat
Most medial of the facial compartments
Perforating vessels from the angular artery course within the nasolabial septum.
The volume of the nasolabial fat is preserved.
Jowls
Separate from the nasolabial fat
Adherent to the depressor anguli oris muscle
Bound medially by the lip depressor muscle and inferiorly by membranous fusion of platysma muscle
Tip:
Potential space for fat transfer exists between the periosteum and the deep medial fat (Ristow space).
Tip:
One reason for a prominent nasolabial fold with aging is a pseudoptosis of the nasolabial fat secondary to loss of volume of the deep medial fat compartment and subsequent decreased midface projection of the deep and superficial cheek fat.
Superficial fascia (SMAS) 1 – 3 , 11 – 14
This is an upward extension of the superficial cervical fascia.
The superficial fascial form is continuous throughout the face and neck.
This layer is variably named according to the region and superficial muscles that it invests.
In the scalp: Galea
In the temple: Temporoparietal fascia (also called superficial temporal fascia)
In the periorbital area: Orbicularis fascia
The SMAS is divided into fixed and mobile portions.
Fixed: Firmly adherent, relatively immobile, found in the lateral face over the parotid gland
Mobile: Nonadherent to underlying structures, found directly over mimetic muscles and parotid duct and anterior to parotid gland
Mimetic muscles are responsible for the coordinated movement of the midface and lips and control the size and shape of the mouth. These muscles commonly overlap and are described in four anatomic layers arranged from superficial to deep.
Depressor anguli oris, superficial portion of zygomaticus minor, orbicularis oculi
Platysma, risorius, zygomaticus major, deeper portion of zygomaticus minor, levator labii superioris alaeque nasi
Levator labii superioris and orbicularis oris
Mentalis, levator anguli oris, buccinator
Muscles of the first three layers are innervated by the facial nerve on their deep surfaces, whereas muscles of the fourth are innervated by the facial nerve on their superficial surfaces.
Senior Author Tip:
This is a common test question.
Deep facial fascia (parotidomasseteric fascia) 2 , 3 , 16
In the neck the deep cervical fascia is found along the superficial surface of the strap muscles.
The deep facial fascia is a continuation of the superficial layer of the deep cervical fascia from the neck onto the face.
Branches of the facial nerve within the cheek, as well as the parotid duct, are deep to the deep facial fascia.
As with the superficial fascia, this layer is variably named according to the specific region of the face.
Over the parotid: Parotid capsule, or investing fascia of the parotid
Over the masseter: Masseteric fascia
Superior to the zygomatic arch: Deep temporal fascia
The relationship of the superficial and deep facial fascia:
These layers may either be separated by an areolar plane or firmly adherent to each other.
In the temporal region the frontal branch of the facial nerve and the superficial temporal artery can initially be found in the areolar plane on the undersurface of the temporoparietal fascia (superficial facial fascia). Deep to this plane is the deep temporal fascia (deep facial fascia).
The superficial and deep facial fascia are firmly attached along the zygomatic arch, overlying the parotid gland, and along the anterior border of the masseter.
Tip:
The frontal branch becomes invested by temporoparietal fascia.
Found deep to the deep facial fascia (parotidomasseteric fascia)
As the facial nerve branches continue peripherally, they pierce the parotidomasseteric fascia to innervate the mimetic musculature.
The buccal fat pad, parotid duct, facial artery/facial vein, and zygomatic and buccal branches of the facial nerve are found within this plane.
Contributes to cheek and facial contour
Consists of a central body with temporal, pterygoid, and buccal extensions
Zygomatic and buccal branches of the facial nerve course superficial to the buccal extension.
The parotid duct separates the buccal extension from the central body.
Fascia of the neck 18
Superficial fascia
The deep thoracic fascia covering the pectoralis major and deltoid muscles gives rise upward to the superficial fascia of the neck.
This is contiguous with the superficial facial fascia (or SMAS) above the jawline.
Laterally, the superficial fascia fuses with the investing deep fascia of the sternocleidomastoid and trapezius muscles.
Deep fascia
The investing deep fascia is the most superficial deep fascial layer.
The investing deep fascia is also called the superficial layer of the deep cervical fascia.
It acts as a visual and mechanical barrier during platysma dissection.
No vital midline structures are present in the subplatysmal space while superficial to the investing deep fascia.
Fascia of the infrahyoid muscles
Formerly known as the middle fascia
Superficial layer: Invests the sternohyoid and omohyoid muscles
Deep layer: Invests the sternothyroid and thyrohyoid muscles
Visceral fascia
Pretracheal fascia: Covers larynx and trachea and splits to invest the thyroid cartilage
Buccopharyngeal fascia: Invests the buccinator muscle and dorsal esophagus
Prevertebral fascia
Encases the vertebral column and its associated muscles and forms the floor of the posterior triangle of the neck
Senior Author Tip:
Preservation of the cervical investing fascia is essential to addressing and placating the platysmal bands. To achieve a longer-lasting result without dehiscence, obtain suture bites of both and anterior AND posterior investing fascia (since the attenuated anterior fascia that led to the bands in the first place is insufficiently strong to hold in the long term).
Nerves
Sensory Innervation
Sensation to the scalp, face, and neck is supplied by divisions of the trigeminal nerve (CN V1, V2, V3) and cervical spinal nerves (dorsal and ventral rami), and the auditory canal is given by the vestibulocochlear (CN VIII) and vagus (CN X).
Ophthalmic division (CN V1)
The frontal nerve enters through superior orbital fissure above muscles and divides into supratrochlear and supraorbital branches.
Supratrochlear branch exits orbit medially and courses upward along with the supratrochlear artery to innervate the central forehead. 19 , 20
Supraorbital branch passes through a supraorbital notch or foramen along with the supraorbital artery to supply the remaining forehead and scalp.
The lateral branch of the supraorbital nerve is the major sensory nerve of the scalp and runs along or medial to the temporal crest.
Maxillary division (CN V2)
Sensation to the midface is provided by the zygomaticotemporal, zygomaticofacial, and infraorbital branches of the maxillary division of the trigeminal nerve.
Mandibular division (CN V3)
The auriculotemporal, mental, and buccal nerve branches are part of the mandibular division of the trigeminal nerve.
Auriculotemporal nerve: Travels with the superficial temporal artery and supplies sensation to the temple superior to the ear
Buccal branch: Communicates with the buccal branches of the facial nerve and supplies sensation to the skin of the cheek over the buccinator
Mental nerve: Supplies sensation to the chin and lower lip
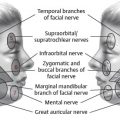
Cervical spinal nerves (Fig. 30-2)
Supply sensation to the entire neck, lower ear, lower posterior face, and posterior scalp
Lesser occipital nerve (C2): Provides sensation over the postauricular mastoid area 21
The greater occipital nerve is a medial branch of the dorsal ramus of C2 that runs up to supply the posterior scalp to the vertex. 22
The great auricular nerve arises from the dorsal rami of C2–3.
Anterior branch: Supplies the skin of the face over the parotid
Posterior branch: Supplies the medial and lateral surfaces of the ear, including the concha and lobule
Senior Author Tip:
The supraorbital nerve and supratrochlear nerve can exit through a true bony foramen (40% and 18%, respectively) or through a notch, which always has a ligamentous floor.
Related posts:




Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


