30 Endoscopic carpal tunnel release: Anterograde single incision
*Endoscopic Carpal Tunnel Release video is available at http://goo.gl/4Uab7r
INDICATIONS
Uncomplicated carpal tunnel syndrome: diagnosed by positive physical examination findings, electromyogram (EMG), or both, demonstrating median nerve compression at the carpal tunnel.
INTRODUCTION
Endoscopic carpal tunnel release using an anterograde portal is a safe and effective means of releasing median nerve compression at the carpal tunnel for patients with symptomatic median nerve compression. In the early stages of median nerve compression, patients will typically complain of numbness, pain, and paresthesias in the thumb, index, and long fingers. However, the paresthesias may be described beginning as high as the neck and elbow. All other pathology must be ruled out before the diagnosis is made, including, but not limited to, cervical radiculopathy and compression at the elbow. Physical exam findings will typically demonstrate a positive Phalen and Durkan tests in the early stages and, in the later stages, weakness and thenar muscle wasting. Electromyographic (EMG) and nerve conduction studies (NCS) of the ulnar and median nerves at the elbow and the wrist are commonly performed prior to surgery. These tests can define the site of compression and quantify the pathology. Non-operative treatments include bracing and steroid injections. Table 30.1 indicates the necessary equipment.
Standard hand table and drapes | 18- or 24-inch tourniquet and Esmarch |
#15 scalpel | Synovial elevator |
Progressive blunt dilators | 3M Agee Carpal Tunnel Release System |
5-0 nylon suture | Petrolatum gauze dressing |
4 × 4 inch gauze | 3-inch elastic bandage wrap |
ANESTHESIA
High wrist block or axillary block.
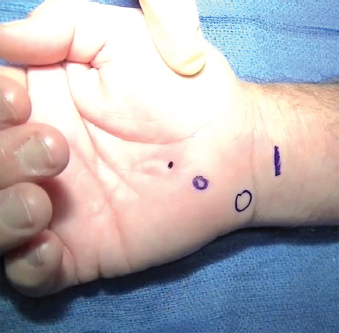
MARKINGS
After appropriately marking the patient’s correct arm (Figure 30.1), the procedure begins with a mark on the patient’s forearm at 1 cm proximal to the distal wrist flexion crease between the palmaris longus and the radial border of the flexor carpi ulnaris. In addition, the pisiform and hook of the hamate should be marked, and the distal end of the transverse carpal ligament should be palpable. All instrumentation should be aimed in the direction of the fourth ray.
Related posts:






Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


