30 Cosmetic Surgery of the Asian Face
Introduction
The rise of Asian cosmetic surgery has been phenomenal over the past 5 years. This has been largely led by the cosmetic surgery boom in South Korea, where 13 in 1,000 population has had some form of cosmetic procedure done, the highest per capita in the world, according to a survey led by the International Society of Aesthetic Plastic Surgeons. 1
It is necessary to define the scope of discussion in this chapter, as there exists broad ethnic diversity within the Asian continent, which houses a population of 4 billion.
Historically, anthropologists and scientists have used the term “mongoloid” to describe the populations of East and Central Asia.
In this chapter, the term “Asian” refers to the population of patients residing in East Asia and Southeast Asia. The discussion in this chapter therefore excludes South Asians, Middle Easterners, and other Asians with Caucasoid features.
This chapter focuses on the most commonly requested surgery for Asians—blepharoplasty—as well as facial bone contouring surgery, which is a surgery that is unique to the Asian population.
Important Anatomical Differences
Skin
Asian skin is generally more pigmented, with a thicker dermis compared to Caucasian skin. The presence of greater collagen density also results in a florid fibroblastic response after tissue trauma, which explains the tendency of hypertrophic scarring and postinflammatory hyperpigmentation during wound healing in Asians.
Facial Bone Structure
In comparison to Caucasians, anthropomorphic studies have shown that the Asian skull tends to be flat, broad, with a wide facial contour, and increased bizygomatic and bigonial width. The square face with a wide jaw is not considered attractive for Asian women, as they favor an oval-shaped face with a small, V-shaped chin, 2 , 3 the Chinese phrase for this is guāzǐ liǎn or melon seed face.
This explains the popularity of botulinum toxin (off-label use) for masseter hypertrophy amongst Asian women. There are limitations to the amount of facial “slimming” that can be achieved with botulinum toxin, hence surgical procedures have been devised to further reduce the width of the mandibular angle. There has been a rise in popularity of facial contouring surgery in recent years, especially amongst Korean women—this is discussed in detail later in the chapter.
Eyes
It is widely quoted that approximately only 50% of Asians are born with naturally occurring upper eyelid creases. 4
Chen 5 has described seven forms of Asian eyelids, the main ones being eyelids without a crease, a nasally tapering crease, parallel crease, or crease with lateral flare. He also noted that Oriental folds are narrower when compared with Caucasians due to a narrower tarsal height (6.5–8.5 mm) and narrower brow–lid distance.
The presence of an epicanthal fold is also a distinctive feature of the Asian eye. It has been estimated to be present in only 2 to 5% of non-Asians, but about 40 to 90% of the Asian population. 6
Johnson described four clinical types of epicanthal folds: epicanthus supraciliaris, epicanthus palpebralis, epicanthus tarsalis, and epicanthus inversus—with epicanthus tarsalis being the most common in Asians ( Figs. 30.1 and 30.2 ). 7


Facial Bone Contouring
Facial bone contouring is usually achieved with zygoma reduction, mandible angle reduction, as well as genioplasty. These procedures may be done in isolation or in combination to achieve an ideal result.
Zygoma Reduction
The procedure can be broken down into three main steps.
Incision and access
Intraoral
Preauricular
Coronal
Combination of the above
Reduction technique
Osteotomy—designs such as “L” or “I” shaped, with or without bone resection
Shaving
Burring
Fixation technique
Mini plates and screws
Suture
Review of Various Techniques
Onizuka 8 was the first author to publish his technique for reduction malarplasty in 1983. He described an entirely intraoral approach to shave the prominent zygoma with a broad chisel. Whitaker 9 described a coronal approach, reducing both the zygomatic arch and the malar prominence with a bur, at the same time, also carrying out temporal augmentation with an implant.
Other authors such as Ung and Lew 10 and Yang and Park 11 have described a combination of shaving the malar prominence through an intraoral incision, and either a single greenstick fracture or multiple osteotomies of the zygomatic arch through a preauricular or coronal incision.
Rhee et al 12 described utilizing only a preauricular incision to perform shaving of the zygoma body, osteotomy of the zygomatic arch, and lateral corticotomy of the arch.
A more popular method in recent times is to create an L-shaped 13 , 14 , 15 or I-shaped 16 osteotomy via an intraoral approach, combined with osteotomy of the zygomatic arch. Kim and Seul 14 first described the L-shaped osteotomy in 2000, which was carried out via an intraoral approach. Two parallel oblique osteotomies enabled the removal of a small 3–8 mm segment of bone and a transverse osteotomy of the arch was done with a curved osteotome through the same intraoral incision.
Ma 12 removed a segment of bone along the short arm of the L about 4–6 mm wide, and fixed the remnant fragment with bicortical screws.
Wang 13 resected a 3–7 mm segment of bone along the short arm of the L, and fixed the fragment with microplates and screws.
Authors’ Technique
The authors’ approach utilizes both preauricular and sublabial incisions. Small preauricular stab incisions are made in the hairline of the sideburns. The soft tissue and periosteum are dissected off the zygomatic arch. A chisel is then used to osteotomize the zygomatic arch.
Next, sublabial incisions are made, and the periosteum is elevated off the anterior face of the maxillary sinus, as well as the body of the zygoma. The authors use an oscillating saw to create an L-shaped osteotomy of the body of the zygoma ( Fig. 30.3 ).
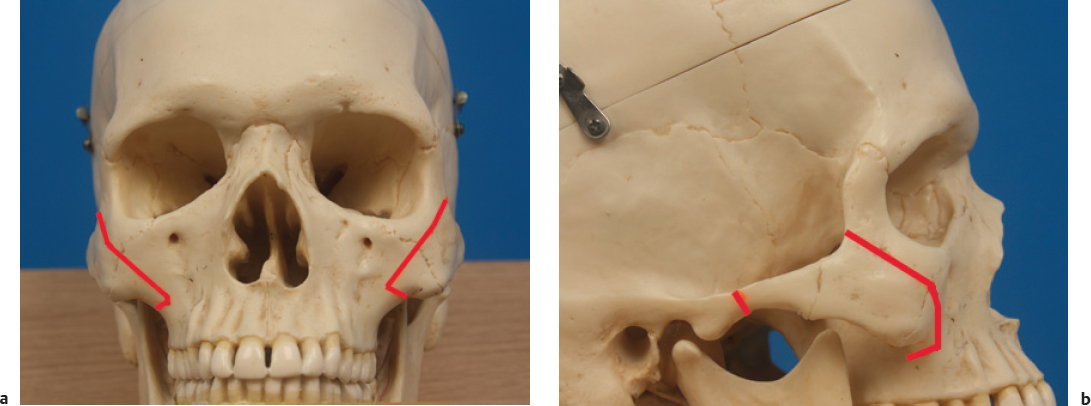
Resection of a 3–5 mm segment of bone along the long arm of the L is done for patients who require it.
The zygoma is then infractured with a mallet. Fixation is achieved with a three-hole miniplate and screws ( Fig. 30.4 ). The preauricular incisions are closed with polypropylene suture, and the sublabial incisions are closed with an absorbable polyglactin suture. Bulky compressive dressings are kept for 3 days, and then replaced with an elastic headband.

Complications
Most surgeons would now avoid using the coronal incision with its attendant risks of alopecia and longer operating time. The intraoral and preauricular incisions would be the main approaches for most authors currently, as the scars are hidden, with quick access to the zygoma.
The main concern for the intraoral approach is that of cheek drooping due to dissection of the masseter muscle; as such, it is important to limit the dissection and detachment of the masseter from the zygoma.
The criticism of using shaving alone as a reduction technique is insufficient reduction as well as periosteal proliferation, causing a high recurrence rate.
Breach of the maxillary sinus mucosa will almost always occur when performing the L-shaped osteotomy; however, sinusitis has rarely been reported. There have been isolated case reports of chronic sinusitis 17 and mucocele 18 occurring after reduction malarplasty.
Despite the proximity of the facial nerve to the zygomatic arch, to the best of the authors’ knowledge, there has been only one published report 19 of facial nerve palsy. This patient also had iatrogenic lateral rectus muscle injury, orbital fracture, and limited jaw opening.
Other reported complications include asymmetry, numbness in the distribution of the infraorbital nerve, hematoma, and malunion.
Mandible Angle Reduction
The main aims of mandible angle reduction surgery are to reduce bigonial width, increase the gonial angle, and increase the mandibular plane angle.
Incision and access
Intraoral
External (usually postauricular)
Combined intraoral and external
Reduction
Ostectomy of the angle
Lateral corticectomy of the ramus
Ostectomy of the posterior aspect of the ramus
Review of Various Techniques
Idiopathic masseter muscle hypertrophy was first described by Legg in 1880. The earliest reports of management of a wide jawline were in the 1940s. Gurney 20 described his method of hypertrophic masseter resection in 1947. Two years later, Adams 21 described the resection of the medial portion of the masseter muscle and simultaneous mandibular angle through an external approach.
It is now widely acknowledged that a wide, square jaw is not only due to masseter hypertrophy, but also due to the underlying skeletal structure of the mandible, 22 , 23 and this is especially so in Asians.
It is important to note that in the assessment of the patient, the surgeon must consider both the gonial angle on lateral view, as well as the bigonial width on frontal view, as the surgical techniques to address each are different.
The early techniques were that of ostectomy of the angle, but as it was found that ostectomy of the angle alone was insufficient to address bigonial width, the addition of corticectomy or sagittal split procedures became more common for suitable patients. Baek et al, 21 in 1989, first reported using intraoral incisions to resect prominent mandibular angle using an oscillating saw, along with resection of the medial aspect of the masseter in some patients.
Later, they refined their contouring method by including tangential osteotomy for patients with lateral flaring of the angle. 24 They also moved away from excision of the masseters, finding that doing so caused more bleeding, swelling, as well as a risk of facial nerve injury.
Pu et al 25 described using either an intraoral incision to perform ostectomy for a flared or wide mandibular angle on frontal view, or a postauricular incision to address retroprotrusion of the ramus on lateral view. Shao et al 26 described a combined method of a long, curved fullthickness ostectomy to correct the incline of the mandibular plane angle, as well as a mandible corticectomy to reduce bigonial width.
Multistage angle ostectomy was described by Ying et al 27 in 2011 to achieve a smooth, natural jaw contour from the lateral view. The first cut is made from the mandibular notch to the ascending ramus. The following cuts are made more anteriorly and progressively less inclined to create a smooth inferior mandibular border.
Related posts:






Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


