3 Surgical Techniques
Surgery of Benign Disease—Diagnostic Procedures
3.1.1 Diagnostic Aspiration Techniques
Aims and Methods
The benign or malignant nature of lesions in the breast must be confirmed histologically. Tissue should be obtained as minimally invasively as possible. Three methods are available: core cut biopsy, vacuum biopsy, and open excisional surgical biopsy; all can be performed after marking of the area in question under ultrasound, mammographic, or MRI guidance. The choice of biopsy technique depends ultimately on the size, morphology, and location of the abnormality and on the imaging. The most frequently employed method is ultrasound-guided core cut biopsy. Vacuum-assisted biopsy is used for diagnosis and also for minimally invasive removal of definitely benign masses such as fibroadenomas, papillomas, or lipomas. Open excisional biopsy is today used only in exceptional cases: diffuse abnormalities (e.g., areas of microcalcification), inconclusive core cut biopsy result (suspected false-negative result), and lesion in a difficult location (axilla, close to the chest wall).
Fine needle aspiration can no longer be recommended for diagnosis of solid masses, on the one hand, because cytology provides lower diagnostic certainty than histology, and on the other hand, because it does not allow measurement of hormone receptors or HER2 and accurate histological diagnosis, which today is mandatory prior to treatment (e.g., before neoadjuvant treatment). Breast cysts obvious on ultrasound scanning are exceptions; cyst aspiration is therapeutic and also allows diagnostic cytology. However, if the cyst recurs, solid tissue should be obtained to exclude co-existing ductal carcinoma in situ (DCIS). Punch biopsy is suitable for investigation of altered skin areas.
Indications and Contraindications
Core biopsy is ideal for solid masses clearly seen on ultrasound scanning and for all palpable masses. It is used only for exceptional cases of microcalcification and the biopsy specimen must then be examined by radiography. Vacuum-assisted biopsy is particularly suitable for lesions that are deemed too small for core biopsy, to diagnose areas of microcalcification, for diagnostic biopsy of lesions seen only on MRI, as a method of biopsying intraductal and intracystic lesions, for repeat biopsy when a previous biopsy was inconclusive, and for removal of clearly benign lesions. Open excisional biopsy is indicated only in exceptional cases when the other methods are not feasible technically. Fine needle aspiration is suitable only for aspiration of simple cysts and possibly for cytology of suspect lymph nodes.
Operation Risks and Informed Consent
The operation risks are injury of adjacent organs such as the skin, chest wall, vessels, pleura, and heart, even though serious complications are very rare. The patient must be informed that a representative biopsy is obtained in a minimally invasive breast procedure only when the suspected diagnosis and histology are correlated. Otherwise, further biopsy is mandatory. The most frequent complication is a more or less extensive intramammary hematoma. Skin bruising is not uncommon after needle biopsy.
Operation Planning
Medical history, clinical breast examination
Diagnostic imaging: ultrasonography, mammography as standard; MRI only when specially indicated
Discussion of the suspected diagnosis, the importance of histological confirmation, and the risks of the diagnostic procedure
Choice of technique, imaging medium, and access route (biopsy channel), depending on the anatomy. Contrary to earlier recommendations, the biopsy channel no longer has to be excised in the course of subsequent surgery, if this becomes necessary.
Postbiopsy correlation of the suspected diagnosis with the final histology
Preoperatively, schedule discussion of the result.
Anesthesia and Positioning
Special Instruments
Breast core biopsy device
Breast vacuum-assisted biopsy device
Procedure
Preparation
Ultrasound-Guided Procedures
Preparation of the biopsy device, checking its function. Place the other necessary equipment in readiness: local anesthetic, injection syringe, disinfectant, formalin or pathology container, dressing materials.
Positioning: supine, possible slightly lateral position
First skin disinfection
Operation
Documentation and Anesthesia
Ultrasound imaging of the lesion
Photodocumentation in three planes
Repeat skin disinfection if necessary
Extensive subcutaneous fan-shaped infiltration of local anesthetic. Caution: Infiltration too close to the tumor can impede the sonographic view.
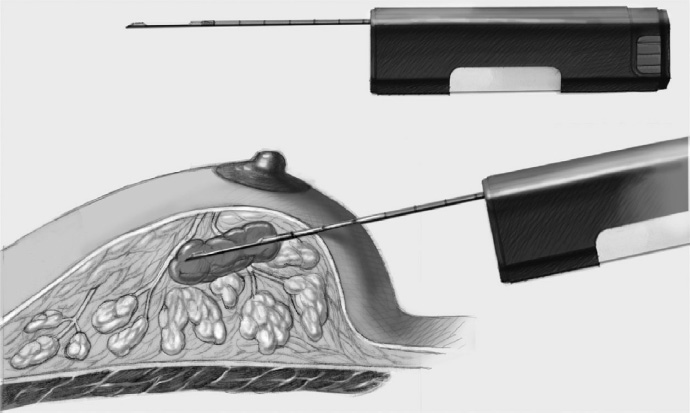
Core Biopsy
After documentation and anesthesia, the biopsy needle (coaxial needle only in exceptional cases) is introduced and positioned before the tumor under ultrasound control, as the needle projects beyond the sleeve of manual devices.
The mechanism is released.
Photodocumentation of the biopsy needle in three planes
The tissue cylinder is removed and the procedure is repeated to obtain at least three core cylinders.
Ask the patient to compress the wound cavity for about 5 minutes.
Skin dressing
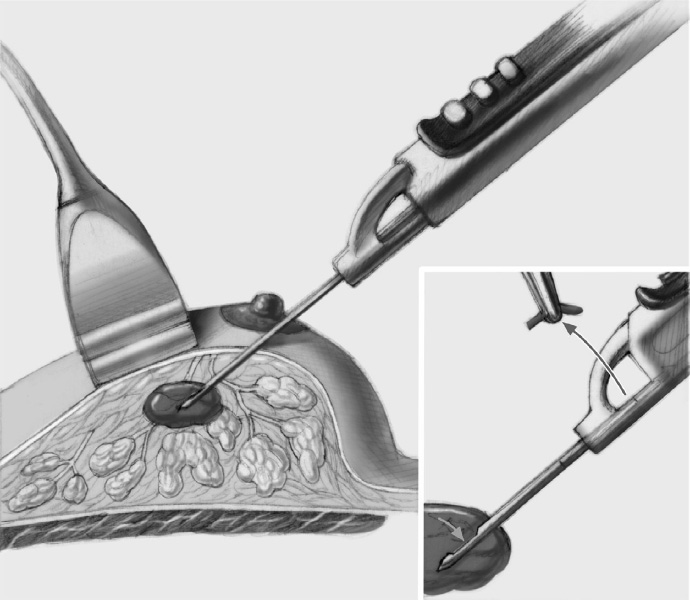
Vacuum-Assisted Biopsy
After documentation and anesthesia a stab incision is made with a size 11 scalpel.
The vacuum-assisted biopsy needle is positioned below the lesion.
Photodocumentation in three planes
The rotating knife is released and the assistant removes the tissue cylinder while the needle remains in the breast.
The planned volume of tissue is removed.
The needle is removed from the breast.
Photodocumentation in three planes
The patient compresses the wound cavity for 10 minutes.
Steristrip dressing
Chest compression dressing with an elastic bandage
Special Technique Diagnostic Aspiration Techniques
Complications
Bleeding: The most important direct complication of the procedure is bleeding, either as a hematoma, which rarely requires surgical revision, or as extensive bleeding, which is a frequent and largely cosmetic problem that resolves completely.
Inflammation: Another very rare complication is postintervention inflammation, with an abscess in an extreme case.
Injuries: Injuries of the chest wall, pleura, and heart have occurred but are extremely rare with cautious ultrasound control taking the tumor location into account. If the location is unfavorable, open excisional biopsy should be performed. Injuries of the surgeon’s free hand, used to stabilize the breast, have also been reported.
Missed biopsy site: Another complication is failure to obtain a biopsy from the actual lesion. If this is suspected and the histological result does not correspond with what is expected, further needle or open excisional biopsy is recommended.
Concomitant and Postoperative Treatment
Correlation between the suspected diagnosis and histology must be considered postoperatively, allowing adequate time for notification of the result. Telephone communication should be avoided, especially in the event of malignant results. Presentation of the case in an interdisciplinary conference is obligatory for planning further treatment. Ideally, benign results should be followed up by clinical and imaging review after 6 months. Malignant lesions should be treated according to existing guidelines and in accordance with interdisciplinary conference recommendations.
Limits of the Methods
While open excisional biopsy was the standard method for diagnosis of breast lesions in the past, and the patient had to decide between a two-stage procedure or uncertainty about the postoperative result (breast conservation versus mastectomy), nearly all breast cancer patients today are informed of their diagnosis before the actual operation takes place, thanks to minimally invasive diagnostic methods. Open excisional biopsy is now required in only a few patients.
3.1.2 Excision of a Palpable Benign Tumor
Aims and Methods
Open excisional biopsy has become much less important due to the development and consistent use of minimally invasive biopsy techniques like core cut biopsy and vacuum-assisted biopsy. Nevertheless, there is a range of benign tumors that are removed by open excisional surgery, following minimally invasive histological diagnosis. Although vacuum-assisted biopsy techniques have shown good results—for example, for fibroadenomas < 2 cm—direct excision, especially of palpable lesions, remains a classic breast surgical procedure.
Indications and Contraindications
A requirement for nononcological excision of a usually palpable breast lesion is secure exclusion of a malignant process. Palpable tumors that are removed this way include fibroadenomas, lipomas, persistent cysts, and definitely benign areas of fibrocystic disease. Malignant breast tumors require entirely different treatment as regards incision, safety margins, secondary resection, and overall treatment plan than do palpable benign lesions. Although some of the surgical principles of simple tumor excision (lumpectomy) will be found in the section on simple breast-conserving treatment, malignant or histologically unconfirmed tumors are the most important contraindication to the techniques described here.
Operation Risks and Informed Consent
The most important complications of these low-risk operations are wound infection, secondary bleeding, the need for revision, ugly scars, and suboptimal cosmetic results. Specific risks include recurrence, even with benign lesions, especially if resection is incomplete, and the danger of finding malignant areas in the final histology, which requires further surgery with appropriate oncological precautions.
Operation Planning
Medical history, clinical examination (inspection, palpation)
Imaging: breast ultrasonography. The need for mammography in addition must be decided on the basis of the patient’s age and the certainty of the ultrasonic diagnosis.
Histological confirmation by core cut biopsy, usually under ultrasound control
After confirmation of the histological diagnosis, detailed discussion and planning of further treatment with the patient: open excision versus vacuum-assisted removal; if the tumor is not clearly palpable, pre- or intraoperative marking under ultrasound control should be planned.
Consent to the procedure
Anesthesiologic preoperative investigations depending on the patient’s age and local practice
Thrombosis prophylaxis according to potential risk. Low molecular weight heparin is not usually necessary with an ambulant procedure.
Antibiotic prophylaxis: first or second generation cephalosporin, single dose
Easy surgery: usually takes less than 1 hour; surgeon and one assistant
Anesthesia and Positioning
Special Instruments
Breast set: dissecting scissors, electrocautery knife, electrocautery needle, skin hooks, Roux hooks, electrocautery scissors if necessary
Procedure
Preparation
If a tumor is not palpable with certainty, immediately preoperative or intraoperative ultrasound-guided or radiographically-guided needle marking is indicated. Experience has shown that tumors that can just be felt through the skin can often no longer be identified by palpation after loss of the skin “abutment.” In case of doubt, preoperative marking or intraoperative ultrasonography is advisable.
As a bladder catheter is not inserted, a visit to the toilet is advisable before transport to the operating room.
Identification of the patient (in the pre-op room and operating room): file and patient match; patient confirms the side of operation according to the entry in the file or preoperative marking.
Intubation or laryngeal mask
Positioning: semi-seated versus lying flat; both arms abducted
Skin preparation, sterile draping: thoracic access
Operation
Skin incision: incision of the skin and subcutaneous fat should be cosmetic, as far as possible around the areola.
Radial incisions are often, though not always, poorer cosmetically. They lead to scar hypertrophy and scar distortion. Tumors in the center of the lower half of the breast are an exception: a circular skin incision and removal of tissue can often result in the nipple being pulled downward.
The same applies for tumors in the axillary tail: depending on the extent of the resection, the incision can be curved over the lesion, segmental, or over the lateral line of the breast. Thus, an incision in the anterior axillary line or along the inframammary fold is possible.
A periareolar incision is most favorable cosmetically. Even somewhat more peripheral tumors can be removed through this incision after tunneling under the skin.
Tumors located low in the inferior part of the breast can be reached by an incision in the submammary line, which combines the best cosmetic scar with a short operative access route.
Following skin incision, dissection in the breast proceeds as far as the surface of the tumor. If the tumor has been marked, dissection is toward the wire with its tip in the tumor. The principle of intramammary dissection of benign tumors is as little trauma as possible.
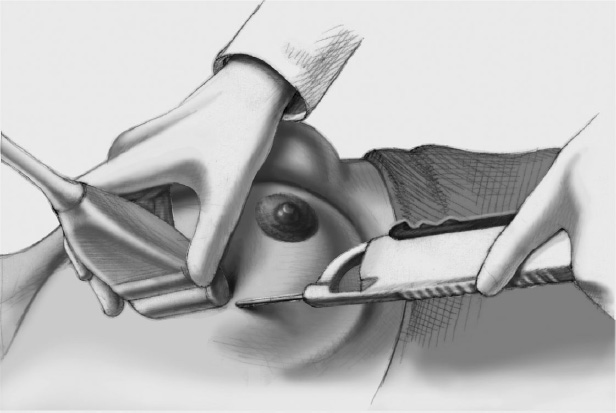
A sharply demarcated tumor (fibroadenoma) is exposed by spreading with scissors, grasping with a clamp and delivering it from its bed. Although most dissection in breast surgery is performed by electrocautery today, blunt spreading of dissecting scissors is suitable for atraumatic dissection of benign solid lesions. With electrocautery dissection there is a risk of cutting into the lesion, thus losing the smooth tumor surface.
Especially for a fibroadenoma, the most common benign tumor, blunt digital dissection is also possible after the surface has been identified and the lesion has been partially dissected; very variable degrees of “ingrowth” into surrounding tissue are observed.
Removal of the tumor in full is always desirable, both with fibroadenomas and in the case of lipomas, which are often but not always encapsulated from the surrounding fat.
After removal of the tumor, the wound bed is palpated for further induration and inspected carefully for bleeding, which is stopped by electrocoagulation. Insertion of a suction drain is not always necessary.
With smaller tissue defects, it is not necessary to approximate the breast tissue. Larger wound cavities should be closed by a few interrupted absorbable sutures, and this may necessitate mobilization of breast tissue.
The wound edges are approximated by interrupted subcutaneous sutures (3–0, 4–0) burying the knots, and the skin is closed by a continuous intracutaneous suture.
Related posts:





Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


