29. Periorbital Anatomy
Skeletal and Surface Anatomy
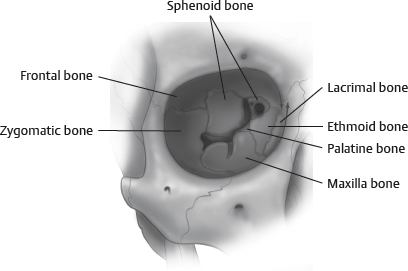
Key Skeletal Landmarks of the Periorbital Region
Superior orbital rim: Fixed landmark to assess brow position
Inferior orbital rim: Position relative to anterior surface of globe; important in determining positive versus negative vector of orbit
Temporal ridge: Delineates lateral border of forehead from temporal fossa
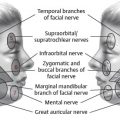
Supraorbital notch: Delineates location of supraorbital neurovascular bundle
Eyebrow Surface Anatomy
Upper Forehead Arranged in Well-Defined Layers
Skin
Subcutaneous tissue
Galea aponeurosis
Loose areolar tissue
Periosteum
At origin of frontalis muscle, the galea splits into a superficial and deep layer to encase the muscle.
The deep layer splits again at the midforehead level to surround the galeal fat pad, and again caudal to the fat pad to form the glide plane space of the brow.
The subgaleal space, deep layer of the galea, and periosteum fuse in the lower forehead and are firmly attached to the frontal bone.
Movement of the brow is produced through the action of brow elevators and depressors and is enhanced by the presence of the galeal fat pad, glide plane space and subgaleal space.
The periosteum of the frontal bones is reflected at the arcus marginalis to become the periorbita of the periorbital bones. The arcus marginalis is a thick condensation of periorbita as it enters the orbit.
Eyelid Surface Anatomy
Protects the eye from injury and excessive light and prevents desiccation of the cornea.
Provides nutrients to the avascular cornea, distributes oil throughout the tear film, debrides the ocular surface of foreign matter, and secretes antiinflammatory substances onto the cornea
Promotes drainage from the lacrimal system
Consists of two lamellae:
Skin/orbicularis oculi
Tarsoconjunctival layer
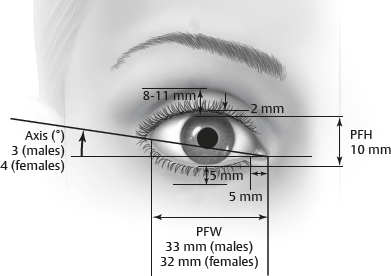
Palpebral fissure: Aperture between upper and lower eyelids (Fig. 29-3)
8–12 mm vertically, 28–30 mm horizontally
Upper lid margin rests 0.5–1.0 mm below the upper limbus.
Lower lid margin lies at the level of the lower limbus.
Skin
Eyelid skin is the thinnest on the body.
Minimal subcutaneous fat
Adjacent brow and malar skin are notably thicker.
Surgical incisions within the skin of the eyelid generally heal with almost imperceptible scarring.
Age-related changes in the skin include decreased type I collagen and increased dermal collagenase activity.
Muscles
Frontalis
Originates from the galea aponeurosis and inserts into the dermis of the lower forehead
Interdigitates with procerus and orbicularis at its insertion
Elevates brow, produces transverse forehead rhytids
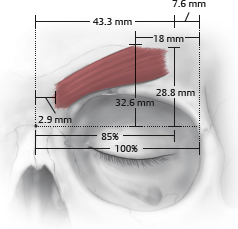
Corrugator supercilii (Fig. 29-4)
Corrugators start 3 mm lateral to midline and end about 85% of distance to lateral orbital rim. 3
Oblique head: Originates from the superomedial orbit and inserts into the dermis of the medial brow
Transverse head: Originates from superomedial orbit and inserts into dermis superior to the medial third of the medial brow
Depresses and medializes the medial brow, produces vertical glabellar rhytids
Lies deep to frontalis muscle
Depressor supercilii
Originates from superomedial orbit and inserts into the dermis of the medial brow, medial to the insertion of the orbicularis
Lies superficial to the corrugator
Depresses the medial brow
Procerus muscle
Originates from fascia covering lower part of nasal bone
Inserts onto glabellar dermis
Depresses the glabella
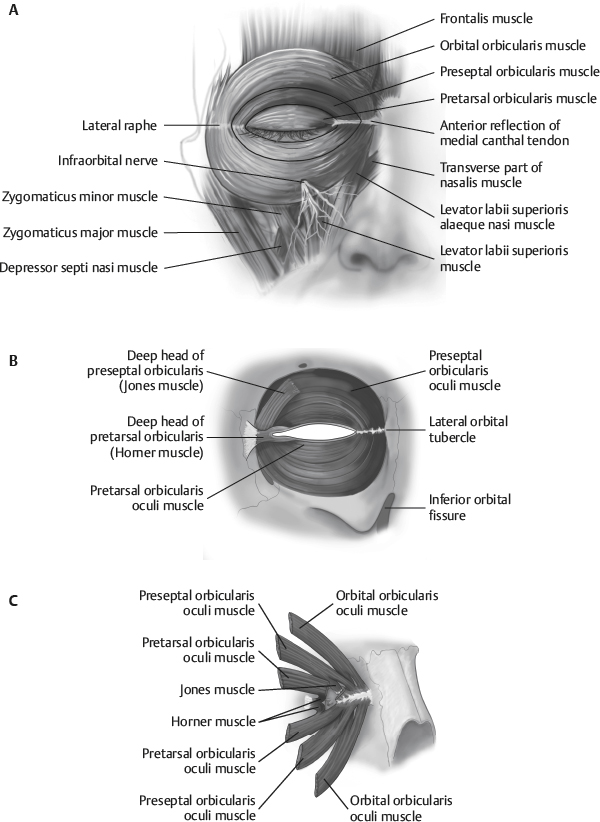
Orbicularis oculi (Fig. 29-5)
Encircles the periorbital region
Primary constrictor of the lids
Innervated by the facial nerve (CN VII)
Runs on the deep surface of the muscle
Pretarsal fibers lie over the region of the tarsal plate.
Responsible for involuntary blink
Preseptal fibers overlie the orbital septum.
Assist with blink
Both voluntary and involuntary fibers
Orbital fibers overlie the orbital rims.
Produce voluntary, forceful closure
Note:
Age-related changes in the orbicularis oculi are secondary to muscle relaxation and increasing ptosis.
Note:
Changes result in visibility of the inferior muscle border with formation of a malar crescent 4
Muscle of Riolan: Portion of the pretarsal orbicularis comprising the “gray line” in the eyelid margin. Promotes secretion from the meibomian glands.
Horner tensor tarsi muscle: Portion of the pretarsal orbicularis attaching to the posterior lacrimal crest. Encircles the canaliculi and promotes lacrimal drainage.
Jones muscle: Posterior preseptal orbicularis muscle fibers that insert on the posterior lacrimal crest and promote tear drainage.
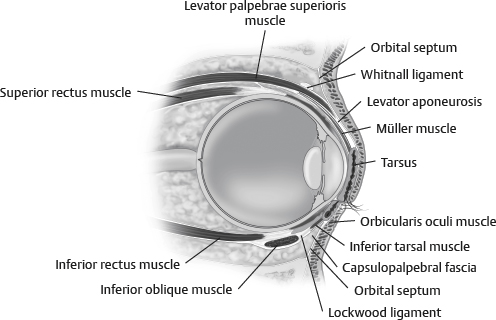
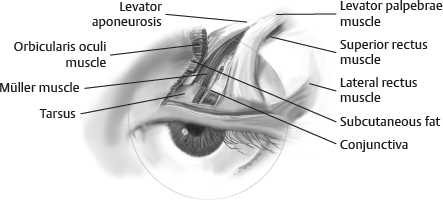
Eyelid retractors
Upper lid (Fig. 29-6)
Levator muscle
Origin at the posterior orbit on the annulus of Zinn
Insertion onto the superior tarsal border
Insertion through the orbicularis onto the subdermal skin at the lid crease (in whites, lower insertion or none at all onto subdermal pretarsal skin in Asians)
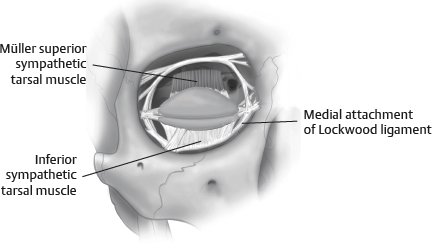
Müller muscle (Fig. 29-7)
Innervated by the sympathetic nervous system
Arises from the inferior surface of the levator approximately 10-12 mm above the upper border of the tarsal plate and inserts onto the superior edge of the tarsus
Loss of function results in 2-3 mm of ptosis.
Levator palpebrae superioris
Innervated by the superior division of CN III
Originates from the lesser wing of the sphenoid above the optic foramen at the annulus of Zinn and extends forward to insert onto the superior edge of the tarsus; also, attaches to the posterior lacrimal crest through the medial horn of the levator tendon, the lateral orbital tubercle, and the pretarsal skin forming the eyelid crease
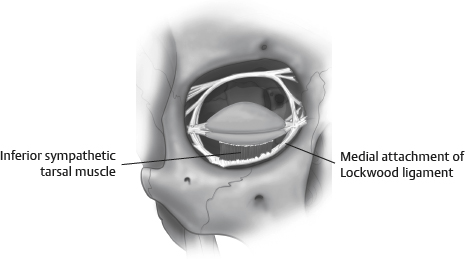
Lower lid
Inferior tarsal muscle is analogous to Müller muscle in the upper eyelid (Fig. 29-8).
Innervated sympathetically and may result in 1 mm of lower eyelid retraction when sympathetic defects are present
Arises from posterior border of capsulopalpebral fascia and inserts onto the inferior border of the lower eyelid tarsal plate
Related posts:



Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


