29 Aesthetic Facial Use of Botulinum Toxin in East Asians
Pearls
The treatment strategy behind botulinum toxin type A (BTA) in East Asians, regarding dosages and injection points, should be based on the following considerations: the patient’s muscle mass, muscle shape, and pattern of muscle activity; ethnic differences between East Asians and Caucasians; and aesthetic appropriateness in the context of the patient’s overall facial structure.
Compared with Caucasians, East Asians have relatively wide, round, and flat faces. The use of BTA for the treatment of masseter hypertrophy and enlarged parotid gland, in which a square-shaped face can be smoothed by decreasing the facial width and achieving a “V” shape in the front profile, is popular among East Asians for this reason.
BTA injection for the purposes of widening the palpebral aperture (i.e., the eye opening) by injection of the lower eyelid is contraindicated in East Asians because it may remove the pretarsal bulge. However, East Asians do consider the widened palpebral aperture a hallmark of female beauty (known as the “charming roll”).
Eyebrow “shaping” with BTA, popular in Caucasians, is also not recommended for East Asians because prominently arched brows may look especially unnatural in an Asian face, which is relatively wide.
Asians generally tend to have a smaller mass, and less hyperdynamic activity, of facial muscle than Caucasians. Therefore, lower doses of BTA may be required in East Asian patients compared with Caucasians. Generally, in Asians an initial dose of 3 to 6 U is recommended for forehead horizontal lines and 10 U for glabellar frown lines.
Most physicians use clinical equivalence at a conversion ratio of 1:1 for aesthetic use of onabotulinumtoxinA and other BTA products, except abobotulinumtoxinA, for which the conversion ratio is believed to be 1:2.5 for onabotulinumtoxinA to abobotulinumtoxinA.
The main target of BTA when reshaping a square jaw is the lower central belly of the masseter muscle. Deep injection, sufficient to touch the mandibular bone, is very important to avoid embarrassing facial expression (e.g., an unnatural asymmetric smile caused by superficial injection weakening the rizorius in the anterior part of the masseter). Four to six injection points (IPs) with 5 U per injection site are recommended depending on the patient’s muscle volume.
Injection of BTA into an enlarged or protruding parotid gland can reduce the width of the lower face by blocking the action of acetylcholine as a neurotransmitter in the salivary glands. Deep intraglandular injection at the most protruding part of the parotid gland around the mandibular angle is required with five or six IPs and 5 U per injection site.
The use of multiple intradermal injections of BTA (intradermal BTA), under various names such as “mesobotox,” “dermatoxin,” and “microtoxin,” has been widely adopted in Asia. The treatment is used not only to reduce dynamic facial wrinkles but also to reduce static wrinkles and pore size. An additional action is creating the so-called perceived lifted effect or pseudolift. Thus, intradermal BTA can be considered to produce a full range of antiaging effects.
Introduction
Since Carruthers et al1 first applied botulinum toxin type A (BTA) for the treatment of glabellar frown lines in 1987, BTA injection has gained world-wide popularity as a dynamic wrinkle reduction treatment because of its easy application, convenience, and safety. However, more recently, the application of BTA for aesthetic purposes has gone far beyond simply reducing wrinkles. Its application has been expanded into correction of facial contours caused through disuse atrophy of the masseter muscle,2,3 correction of the body contour through disuse atrophy of calf muscles, and also treatment of focal hyperhidrosis.4
Several papers and consensus publications have provided guidelines for the aesthetic use of BTA.5,6,7,8 However, most of these publications have focused exclusively on Caucasian subjects, except for recent consensus recommendations by Korean experts for the aesthetic use of BTA in Asians.9 This chapter focuses on the ethnic differences between East Asians and Caucasians for the aesthetic use of BTA in terms of anatomy, the applicable dose, injection methods, and indications of BTA, thereby providing some practical suggestions for the aesthetic use of BTA in East Asians.
Patient Evaluation
Each patient should be examined individually. Individualized assessment and treatment are necessary because there is significant variability among individuals within the same East Asian population in the shape and function of many target muscles. Dosages and IPs should be based on the subject’s muscle mass, muscle shape, pattern of muscle activity, and judgment of what is aesthetically appropriate in the context of the individual patient’s overall facial structure. However some critical ethnic differences between East Asians and Caucasians should be kept in mind in developing a treatment strategy for East Asians using BTA.
Differences in Aesthetic Ideals
Compared with Caucasians, East Asians have a relatively wide, round, and flat face. For this reason, East Asians consider a smaller, narrower, and more threedimensional face to be more attractive, and may wish to achieve this ideal using botulinum toxin. One of the most typical examples of this is treatment for masseter hypertrophy using botulinum toxin, which is not popular in Western countries even though it was first developed in Western countries more than 20 years ago.2 This novel treatment with BTA helps those East Asians with a square-looking face to achieve a decreased facial width and a “V” shape to the face in front profile as well. In a similar context, botulinum toxin treatment for the parotid gland is gaining popularity among East Asians as a way of decreasing facial width.
BTA injection for widening the palpebral aperture (the eye opening) is another typical example of the difference in treatment approaches between Asians and Caucasians. BTA injection can remove the pretarsal bulge and slightly lower the inferior ciliary margin to widen the palpebral aperture.10 However, it is important not to diminish the pretarsal muscular bulge in East Asians, who consider it a hallmark of female beauty (the “charming roll”). They may also believe that the “charming roll” brings the optical illusion of a “big eye” (like doubleeyelid surgery does in Asians with inherently smaller eyes). The roll can even be enhanced by the injection of hyaluronic acid filler. In such a context, BTA injection for widening the palpebral aperture is therefore a contraindication in East Asians.
Anatomic Differences between East Asians and Caucasians
Asians generally have a smaller muscle mass and less hyperdynamic activity compared with Caucasians. Specifically, Asians tend to have shorter corrugator muscles than Caucasians. The smaller muscle mass of Asians seems to come not only from genetic differences11 but also from cultural differences, since Asians tend to use their facial expression muscles less than do Caucasians.12 Moreover, Asians have been described as developing fewer age-related wrinkles than Caucasians. This may be because, in comparison with Caucasians, Asians have a thicker dermis,13 increased fat above and deep to the superficial muscular aponeurotic system, and denser fat and fibrous connections between the superficial muscular aponeurotic system and deep (parotidomasseteric) fascia.14 Therefore, lower doses of BTA may be required in East Asian patients than in Caucasians.
Procedural Techniques
Commercial Products of Botulinum Toxin Type A
Commercially available BTA products in Asia are onabotulinumtoxinA (Botox/Vistabel, Allergan Inc., Irvine, California), abobotulinumtoxinA (Dysport, Ipsen, BoulogneBillancourt, France/Medicis/Valeant, Bridgewater, NJ; also licensed as Azzalure to Galderma, Lausanne, Switzerland), and incobotulinumtoxinA (Xeomin/Xeomeen/Bocouture/XEOMIN Cosmetic); botulinum toxin type A (150 kDa) free from complexing proteins (Merz Pharmaceuticals GmbH, Frankfurt, Germany). Other BTA products that have been approved for use in Asia are Neuronox (Medytox Inc., Seoul, South Korea; also marketed as Botulift, Cunox, Meditoxin, and Siax), Prosigne (CBTX-A; Lanzhou Biological Products Institute, Lanzhou, China) and Regenox (Hugel Pharma, South Korea; also marketed as Botulax and Zentox). Another Korean toxin, Nabota (Daewoong Pharmaceutical Co. Ltd., Seoul, South Korea), is licensed and under investigation in the United States and Europe as Evosyal (Alphaeon Corp., Newport Beach, California).
In each product labeling, the manufacturer states that dosage units are not interchangeable because different assays are used to measure the potency of different botulinum toxin type A products. However, several consensus papers and clinical studies support clinical equivalence at a conversion ratio of 1:1 for aesthetic use of onabotulinumtoxinA and other BTA products except abobotulinumtoxinA.5,8,15,16 Various dose conversion ratios have been suggested for onabotulinumtoxinA and abobotulinumtoxinA. Based on available data and clinical experience, most physicians apply a ratio for onabotulinumtoxinA to abobotulinumtoxinA of 1:2.5 for aesthetic use.17,18
Dilution and Storage of Botulinum Toxin Type A
Lyophilized BTA powder should be reconstituted with preservative-free saline to avoid possible reductions in the potency of BTA. However, some advocates for preservative containing saline insist that it reduces the pain experienced by patients from the injection of BTA without influencing the potency of BTA.19,20 Various volumes of normal saline have been used for the reconstitution of BTA powder, from 1 to 10 mL, with 2.5 mL and 3.3 mL being popular dilutions, with respective concentrations of 4 U/0.1 mL and 3 U/0.1 mL.
Various results have been suggested for the effect of refrigerator storage on the potency of BTA following the reconstitution of BTA. Based on available data and clinical experience, however, most physicians store the reconstituted BTA in the refrigerator for up to 4 weeks.21,22,23
Landmark of Injection
The determination of BTA injection sites should be based on muscular and bony landmarks, rather than on cutaneous ones. The eyebrows are a particularly unreliable cutaneous landmark. This is especially so in older people with eyebrow sagging, and in women, due to their propensity to modify the eyebrow shape by tweezing, plucking, etc. Examination of the overlying soft tissues—fat and skin—may be useful as an adjunct.
Injection Levels
While intradermal injection has the benefit of less bruising, precise injection into thin dermis, such as that found in the lower eyelid, is difficult. Moreover, intradermal injection is much more painful than subdermal or intramuscular injection. Therefore, it is more realistic to describe the placement of BTA required for deep muscles, such as the masseter and corrugator, as subdermal or intramuscular.
Site-Specific Techniques
Forehead Horizontal Lines
The target muscle is the frontalis (Fig. 29.1). Consideration points are as follows:
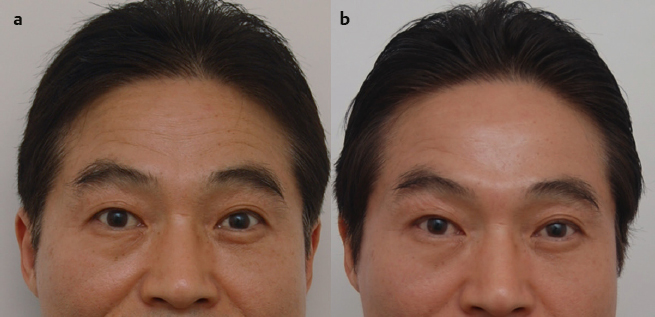
Screening for those at risk of eyebrow ptosis, (e.g., patients with ptosis, or people who congenitally open their eyes with the frontalis) is a prerequisite because eyebrow ptosis is a fairly embarrassing side effect from the aesthetic viewpoint in Asians, who have a wider distance between the eyebrow and the palpebral fissure compared with Caucasians. Typical at-risk patients for eyebrow ptosis are older people (i.e., in their 50s and above); these patients require a low initial dose from 2 to 3 U.
Many Asians require lower doses of BTA since Asians have a smaller muscle mass and less hyperdynamic activity than Caucasians.
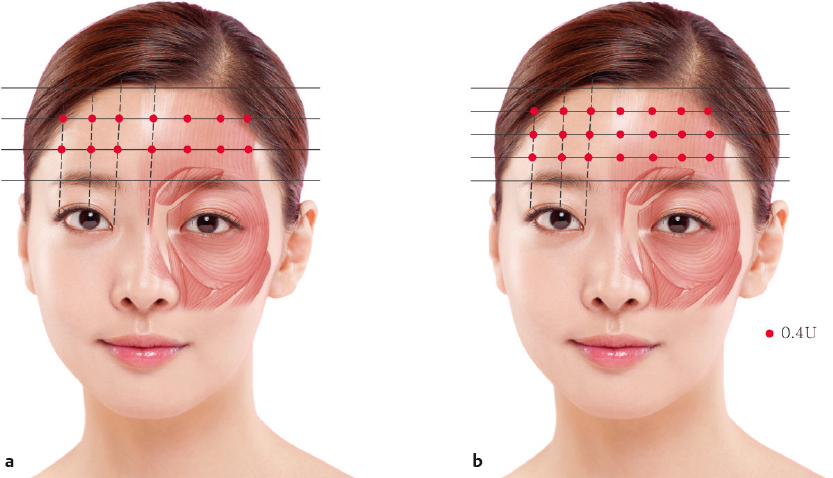
The microdroplet technique at the intradermal level may be of value to preserve expressivity. Generally, two rows of six or seven IPs are recommended (Fig. 29.2a). Alternatives include three rows of injections for people with a high forehead (Fig. 29.2b). Low initial doses from 3 to 6 U are recommended and no more than 12 U in total because of the risk of eyebrow ptosis.
Glabellar Frown Lines
The target muscles are the corrugators and procerus (and sometimes the orbicularis oculi) (Fig. 29.3). The consideration points are as follows:
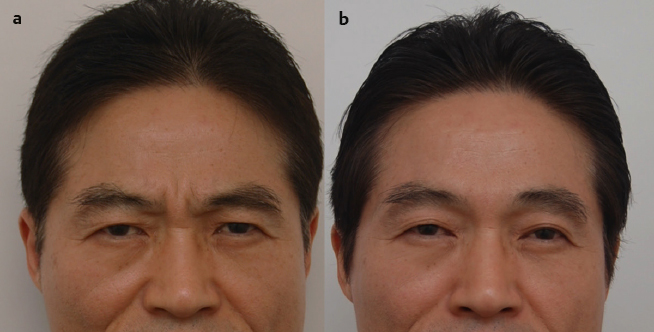
Asians have shorter and narrower corrugator muscles compared with Caucasians.11 Asians also have less hyperdynamic activity than Caucasians12 and consequently require lower doses of BTA. Therefore, a four-point injection pattern (rather than the standard five-point pattern for Caucasians), with injection of the procerus and the medial corrugators (but not the lateral corrugators), is generally appropriate for Asian females. Of course, a five-point injection pattern could be appropriate for Asian males and other subjects with a greater muscle mass. To prevent “samurai eyebrow” (a weird expression especially seen in Asians with a wide face), an additional injection of 0.5 U BTA into the frontalis at 2 cm above the eyebrow in line with a lateral canthal line can be of benefit in subjects aiming to achieve a standard Caucasian pattern.
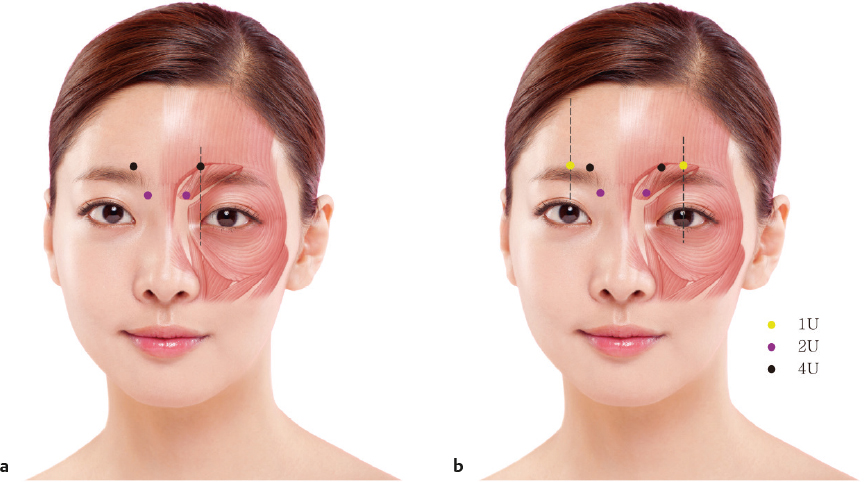
Stretch tests will help to identify subjects for whom the combination of BTA with a soft tissue filler, versus BTA alone, is the most appropriate strategy. Intramusclular injection into four IPs should be used (2 U in two IPs in the procerus and 4 U in two IPs in the medial part of the corrugator) (Fig. 29.4a). The standard Caucasian pattern for glabellar frown lines requires an additional 1 to 2 U at the midpupillary line for the lateral part of the corrugator (Fig. 29.4b).
Occasionally, an additional injection of 1 U at the lateral canthal line immediately above the eyebrow is necessary for those patients with a hyperactive orbicularis oculi.
To avoid ptosis, one of the most serious and uncomfortable adverse effects of BTA, take the IP for the corrugator head above the bony orbital rim by palpating the bony rim, and then inject it slowly with a nondominant finger, compressing the bony orbital rim so as to prevent the spread of BTA into the orbital part below.
Lateral Canthal Rhytides (Crow’s-Feet)
The target muscle is the orbicularis oculi (Fig. 29.5). Consideration points are as follows:
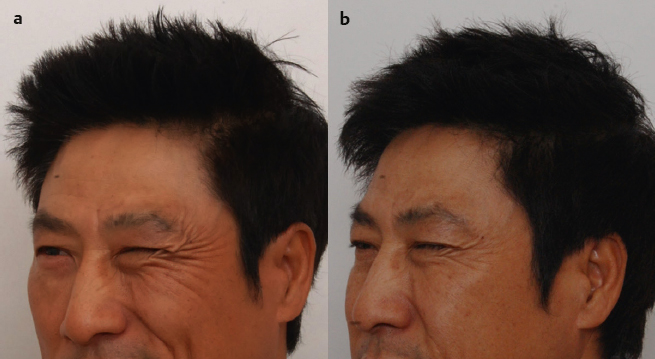
It is important to preserve the expression lines at the lateral canthal lines to some extent to maintain a natural look.
It is also important, prior to injection, to distinguish between orbicularis activity and zygomaticus activity as the cause of wrinkles around the lateral canthal area. Horizontal lines under the eyes and descending lines at the lateral malar area are caused by zygomaticus activity and, consequently, are not indications for BTA. This should be communicated in advance to patients prior to treatment so that expectations are appropriate.
Following BTA for crow’s-feet, Asians with prominent zygoma and abundant premalar fat above the nasojugal groove tend to readily show more prominence of the lateral malar area, which Asians generally hate. In these patients, injection at a lower part is unnecessary; alternatively, a lower dose (i.e., only 0.5 U of BTA) is required.
To avoid bruising, subdermal injection technique is useful for this treatment area as the area has abundant underlying vessels. At least three IPs with 2 to 3 U per IP should be used, with an optional one or two IPs, depending on the wrinkle pattern (Fig. 29.6).

Related posts:





Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


