26 Open Ulnar Nerve Decompression at the Wrist
Abstract
Open ulnar nerve decompression at the wrist is a safe and effective procedure for the treatment of ulnar tunnel syndrome. Knowledge of the unique anatomy of the ulnar nerve, as it courses from the wrist into the hand, is discussed in detail. Understanding of this complex anatomy helps in explaining the various clinical presentations, which can help locate the site of compression. Surgical pearls to help identify the ulnar nerve proper and the critical deep motor branch are explained. Useful surgical tips are discussed which help avoid unnecessary dissection and minimize postoperative complications. Finally, expected outcomes and postoperative protocols are discussed.
26.1 Description
Ulnar tunnel syndrome is a common condition with a variable clinical presentation. A comprehensive understanding of the relevant anatomy is crucial to the successful diagnosis and ultimate treatment of this condition. When conservative measures are unsuccessful, open and methodical decompression of the ulnar nerve and its branches in a timely fashion often leads to resolution of symptoms and rapid return of function.
26.2 Key Principles
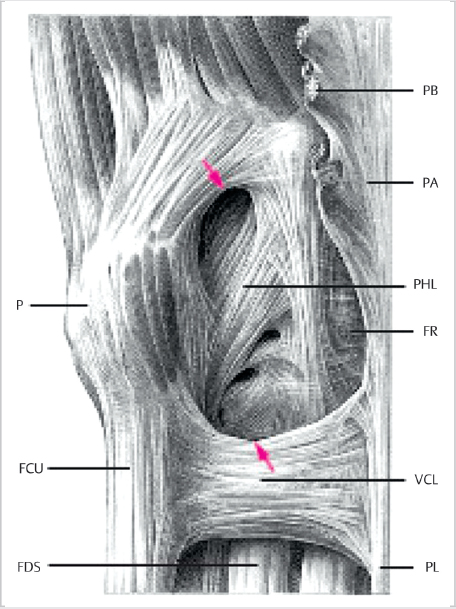
The ulnar nerve at the proximal wrist lies subjacent to the flexor carpi ulnaris (FCU), is relatively superficial, and covered by fascia and skin. The ulnar nerve and artery enter Guyon’s canal, which is a fibro-osseous tunnel formed between the pisiform and hamate hook, as seen in ► Fig. 26.1. The pisohamate ligament forms the floor of the canal, while the roof comprises the volar carpal ligament. Within Guyon’s canal, the ulnar nerve bifurcates into superficial and deep branches. The ulnar artery lies radial and slightly volar to the ulnar nerve. 1 The canal begins proximally at the level of the pisiform with a 6mm oval opening termed the proximal hiatus. The majority of patients exhibit a distal hiatus at the level of the hamate hook, which can be seen as a sickle-shaped tendinous arcade that forms the origin of the flexor digiti minim brevis (FDMB). 2
The branches of the ulnar nerve continue into the hand, with the superficial branch classically described as innervating the palmaris brevis muscle and continuing distally as a pure sensory nerve over the hypothenar muscles (► Fig. 26.2). It then divides into the fourth common digital nerve and the ulnar proper digital nerve to the small finger. Variations and overlap of this “typical” description exist and have been described in the literature. 3 , 4 , 5 The inconsistencies might lead to confusion and delay in diagnosis of certain compressive neuropathies and traumatic injuries. The presence of communications between the ulnar fourth common digital nerve and the median third common digital nerve should be considered when the digital sensory presentation is atypical. The ramus communicans has been described in the literature as being present in 4 to 100% of patients. 4 , 6
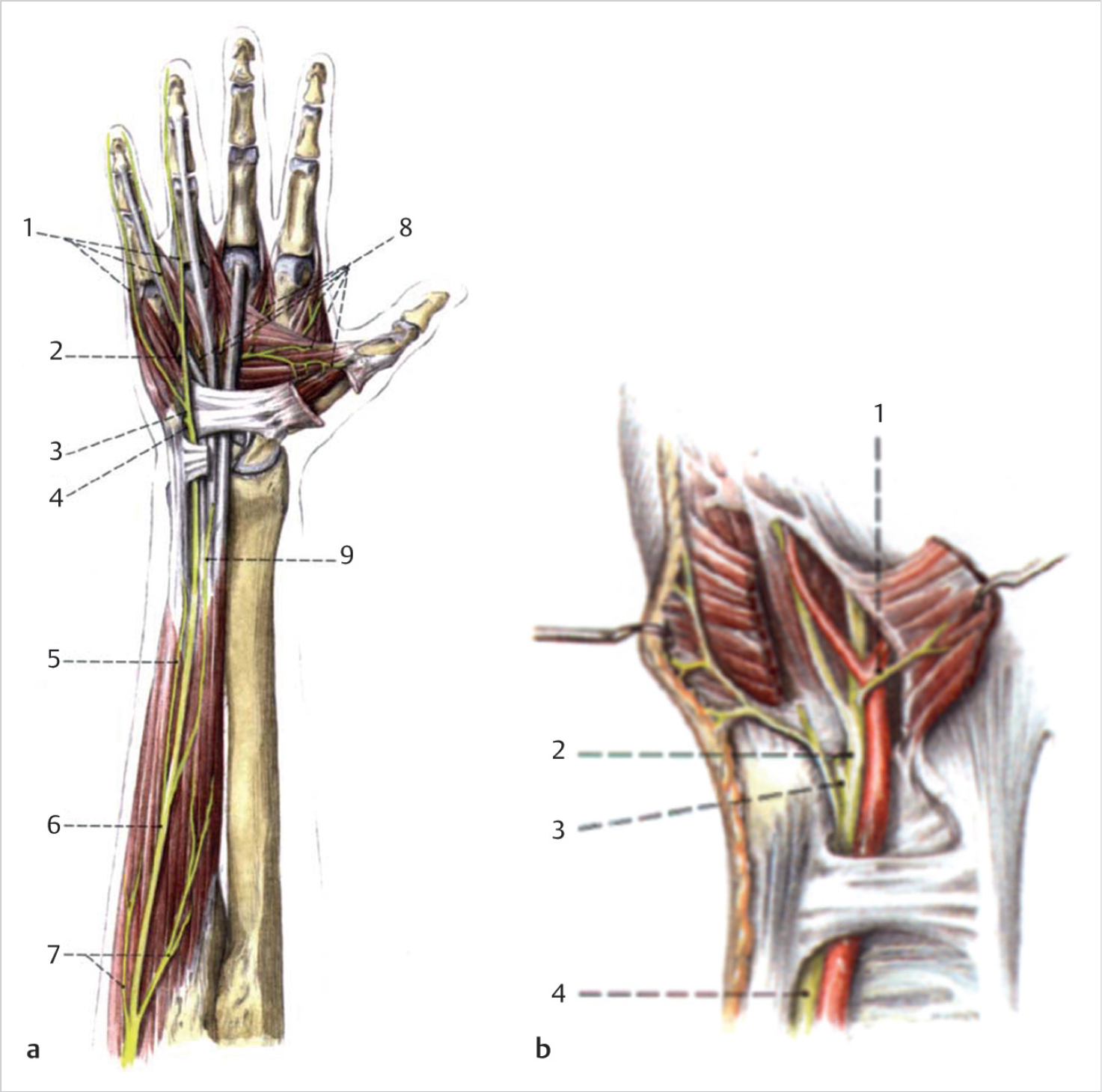
The deep motor branch of the ulnar nerve, accompanied by the deep branch of the ulnar artery, then passes between the abductor digiti minimi (ADM) and the FDMB. This typically occurs just distal to the pisohamate ligament, which serves as an important landmark when isolating the motor branch. The motor branch then perforates the opponens digiti minimi (ODM) and courses radially and deep to curve around the hook of the hamate. It then follows the course of the deep palmar arch beneath the flexor tendons. At its origin, it innervates the hypothenar muscles. As it crosses the deep part of the hand, it innervates all the interosseous muscles and the third and fourth lumbricals. It ends by supplying the adductor pollicis (AP) and the medial head of the flexor pollicis brevis (FPB). It also sends articular branches to the adjacent carpal joints.
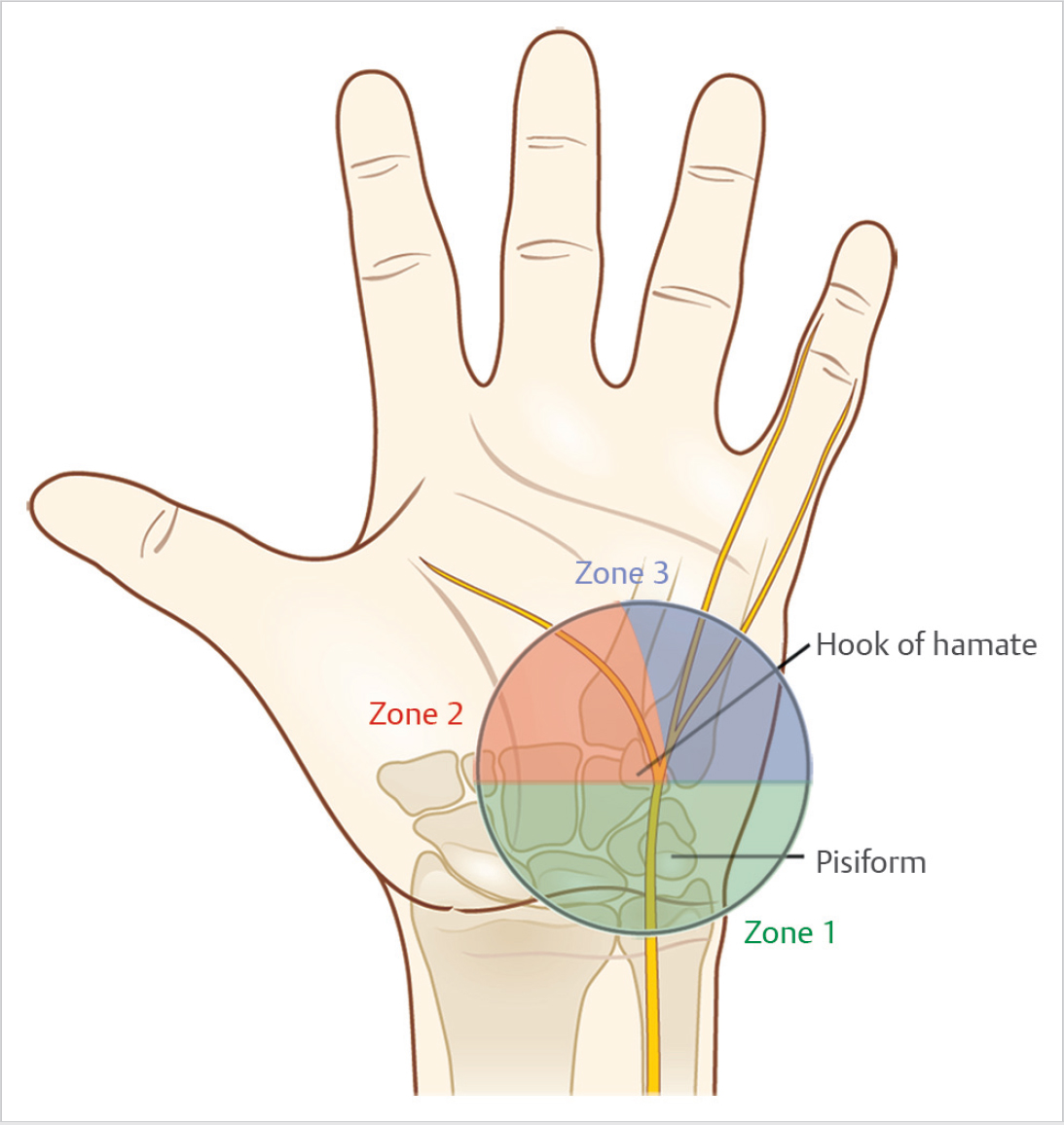
Several clinical presentations of ulnar nerve dysfunction can occur due to compression at the level of the wrist and hand. The presentations might involve isolated sensory loss, isolated motor weakness, or a combination of both. 7 , 8 , 9 The clinical pre-sentation is dictated by the anatomic site of compression (► Fig. 26.3). Guyon’s canal is often divided into three zones: zone 1, zone 2, and zone 3. Zone 1 is the area proximal to the bifurcation of the ulnar nerve, and compression at this level leads to a combined motor and sensory loss. Zone 2 includes the deep or motor branch after it has bifurcated. Compression in zone 2 leads to isolated loss of motor function of the ulnar innervated muscles. Zone 3 encompasses the superficial or sensory branch of the ulnar nerve, and injury at this level leads to sensory loss of the hypothenar eminence, small finger, and part of the ring finger. Zone 3 injury does not lead to motor weakness. We also propose a modification to this well-known classification system to include a newly described Zone 0. This new zone occurs proximal to the take-off of the dorsal sensory branch of the ulnar nerve (but well distal to the cubital tunnel and the innervation of the extrinsic flexor tendon). The clinical picture of a Zone 0 injury would be one of mixed motor and sensory loss, but would also include sensory loss on the dorsum of the little finger and ulnar aspect of the ring finger.
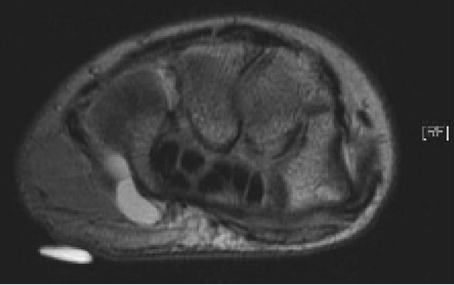
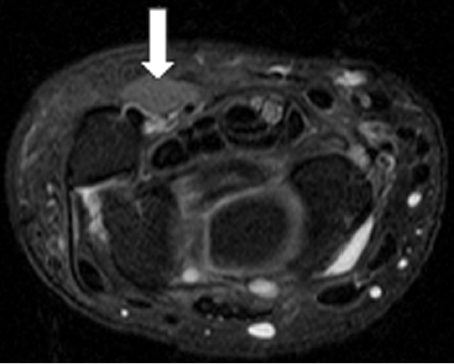
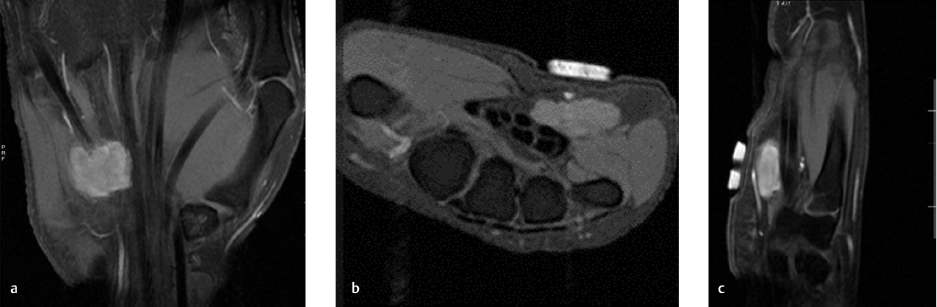
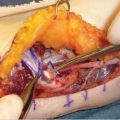
Ulnar tunnel syndrome has been well-described in the literature and might be the result of various causes, including ganglia 8 , 9 , 10 , 11 (as depicted in ► Fig. 26.4), fractures or dislocations of the ulnar side of the wrist, 9 , 12 , 13 anomalous muscle bellies or fibrous bands, 11 , 14 , 15 (as shown in ► Fig. 26.5), hemangiomas, 16 bipartite hamate, 17 giant cell tumors, 18 thrombosis of the ulnar artery, 9 , 11 , 19 osteoarthritis of the distal radioulnar joint and carpal joints, 20 , 21 rheumatoid tenosynovitis, 22 other benign soft tissue masses (shown in ► Fig. 26.6), bicycle racing, and other activities that require either prolonged wrist hyperextension or continuous pressure on the hypothenar eminence. 16 More recently, with the extreme popularity of indoor cycling classes, we have seen an increased prevalence of this condition which is termed cyclers’ palsy.
Related posts:





Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


