22 Neuromodulators in Facial Aesthetics
Introduction
The exponential increase in the use of botulinum neuromodulators (BoNT) for facial rejuvenation has underscored its role as one of the most, if not the most, impactful drugs in aesthetic facial surgery over the last several decades. The use of injectable bioactive agents including neuromodulators and dermal fillers has revolutionized the field of facial aesthetics, vastly increasing the number of nonsurgical, minimally invasive facial rejuvenation options for patients. In 2012, there were 3,257,917 botulinum injections performed, making it the most common nonsurgical cosmetic procedure in the United States. 1 Although BoNT received approval from the U.S. Food and Drug Administration (FDA) for its first cosmetic indication in 2002, the aesthetic and medical use of botulinum toxin long precedes its FDA submission and approval for cosmetic procedures. 2 , 3
As an ophthalmologist in San Francisco during the 1980s, Dr. Alan Scott was the first to investigate the use of botulinum toxin to selectively weaken extraocular muscles in a chick animal model. 2 Continued development of this research eventually led to its approval as Oculinum (sold to Allergan Inc., a small ophthalmology company in Irvine, CA, that eventually changed the name to Botox) for the treatment of strabismus and other neuromuscular disorders around the eye in 1989. During this therapeutic application, unexpected aesthetic benefits were realized and ultimately led to its approval as Botox Cosmetic (Allergan Inc.) by the FDA for the reduction of hyperfunctional glabellar lines in 2002. As thoughtful physicians began exploring other areas of selective neuromuscular activity reduction, clinical applications of onabotulinumtoxinA broadened. Several other botulinum toxin–based neuromodulators became FDA approved ( Table 22.1 ): Dysport (abobotulinumtoxinA; also known as Azzalure [Ipsen]) in 2009 and Xeomin (incobotulinumtoxinA; Merz Pharmaceuticals) in July 2011. Additionally, an onabotulinumtoxinB, Myobloc (rimabotulinumtoxinB; Solstice Neurosciences) was approved in 2000 for the treatment of cervical dystonia. Aside from the injectable forms of BoNT, a topical formulation of BoNT type A (RT001; Revance Therapeutics) has submitted Phase 3 clinical trial data for the treatment of crow’s feet.
1. Botulinum toxin type A
|
2. Botulinum toxin type B
|
This chapter reviews the pharmacology, preparation, pertinent anatomy, and technique of the current clinical applications of BoNT in facial aesthetics and rejuvenation.
Pharmacology
Botulinum toxin is a protein produced by the anaerobic grampositive bacteria, Clostridium botulinum. Originally described as a toxin due to the illness botulism seen with ingestion of large amounts of C. botulinum–contaminated food, they are now better described as neuromodulators given the connotations of the term toxins (most medicines could be considered toxins with improper dosing). BoNT is found in nature as a dipeptide with seven unique serotypes (A through G). Each serotype has a different binding profile that cleaves specific proteins responsible for active transport of acetylcholine into the neurosynaptic cleft. 4 BoNT type A is the more clinically relevant of the seven serotypes and cleaves the SNAP-25, a presynaptic membrane protein, thereby inhibiting fusion of acetylcholine vesicles at the neuromuscular junction. BoNT type B cleaves VAMP, another part of the protein chain on the acetylcholine vesicle membrane, the common biochemical characteristic of BoNT. This inhibition of membrane fusion and subsequent acetylcholine release at the neuromuscular junction results in its neuromuscular blocking effect, causing varying degrees of flaccid paralysis of the postsynaptic muscle. 3 It is through this blocking mechanism that weakened and relaxed muscles decrease the amount of unwanted facial lines and expressions. These effects, though, are temporary as recovery of neuromuscular activity occurs when new neuromuscular junctions are established by axonal sprouting.
Preparation of Product
BoNT is packaged either as a vacuum-dried preparation (Botox, 50 or 100U) or a lyophilized preparation (Dysport, 300U, and Xeomin, 100U) and according to the package insert should be kept cold at 0° to 8°C (except Xeomin, which can be stored up to 25°C). These products need to be re-suspended into a liquid form for injection and the manufacturers recommend using sterile, preservative-free normal saline (0.9% sodium chloride). The amount of saline added varies amongst providers, and patients should understand that treatment effects are determined by the total number of units injected, not the total amount of volume. 5 Due to the fragile nature of BoNT, Botox vials have a vacuum seal to draw in the saline rather than forcefully injecting into the container. Vacuum should be present when injecting the saline and if the vial does not pull the saline into the vial, the sterility of the vial may have been compromised. Neither Dysport nor Xeomin are packaged with a vacuum seal, but a slow injection of the saline will help maintain the quality of the protein. After a gentle swirl of the vial, a very small gauge needle is used to draw up the reconstituted product. It is important not to dull the needle by touching the walls of the vial, which may cause a more painful injection.
While the other three powder preparations are pH neutral, Myobloc is provided in a solution with an acidic pH of 5.6, and the clinical trials have demonstrated significantly increased relative pain with injection of Myobloc. 6 , 7 Additionally, Xeomin is supplied as a naked protein, without other complexing proteins such as hemagglutinin, which may decrease antibody formation. 8
Potency and Reconstitution of Product
Because the three commonly used and FDA-approved BoNT-A preparations (Botox, Dysport, and Xeomin) are packaged as a dry powder form, they need to be reconstituted. Reconstitution is the preferred term when describing the method of converting a dried product into a solution, whereas words like “dilution” or “diluted” are inaccurate and can lead to confusion and concern when describing preparation of a less potent product. The “unit” (U) of measurement for Botox, Dysport, and Xeomin is a manufacturer-specific proprietary bioassay that originated from their initial mice studies. One unit of BoNT-A corresponds to the dose (LD50) that is lethal to 50% of the mice via an intraperitoneal injection.
Thus, the optimal unit dosage varies amongst these brands, and it is important to know these differences. There are a handful of accepted strategies for reconstitution of Botox, Dysport, and Xeomin, and these relate in some cases to the specific bioactivity or “potency” of each product as they are commercially available in the United States and worldwide. 9 , 10 While some experts argue that dosing ratios are irrelevant and one cannot compare or create relative ratios of potency for dosing, this seems incongruous considering each bottle delivered from the company comes with a FDA regulated and approved number of “units” and this must be constant for each product. Thus, if one carefully examines outcome measures in split-face studies in particular, one may deduce a relative ratio of potency for any of these products. 9 , 10 The primary reason for these ratios are the comfort levels many clinicians have with one product and having some starting point when using another. While there is no firm agreement about exact Botox and Dysport potency ratios, most agree that it is 2.5–3 units of Dysport to 1 unit of Botox and 1–1.3 units of Xeomin to 1 unit of Botox. 11 , 12 , 13 , 14 , 15
In the senior author’s (C.S.M.) practice, the total unit amount in each vial of Botox, Xeomin, and Dysport is reconstituted, drawn up in preset amounts, and stored at the appropriate temperature. The BoNT products are drawn up in insulin syringes with a permanently attached 31-gauge needle in the 0.5 mL or 0.3 mL capacity. The advantage of a barrel integrated needle is that there is no Luer lock syringe hub that can potentially harbor any waste product. Because the syringes are manufactured with the needles, the plunger is made to expel the entire volume that is in the syringe. Though the volume loss in hubs may seem miniscule, if one has a highly concentrated product, any routinely wasted droplets would not be costeffective.
The volume of diluent used to reconstitute the products generally ranges from 1 mL to 4 mL per 100U vial for Botox and Xeomin, with most practitioners adding between 2 and 2.5 mL, and 1.5 mL to 3 mL per 300U vial for Dysport. 8 In the senior author’s practice, a 100U vial of Botox or Xeomin is reconstituted with 2.0 mL of sterile preservative-free normal saline, which will yield 5U/0.1 mL. The 300U vial of Dysport is reconstituted with 1.5 mL of sterile preservative-free normal saline, which yields 20U/0.1 mL. The insulin syringes are measured and marked in insulin units by the manufacturer and 10 insulin units equals 0.1 mL. For Botox and Xeomin, increments of 0.2 mL and 0.4 mL are drawn up into a 50 insulin-unit syringe (0.5 mL syringe) to equal 10U and 20U, respectively. Dysport is drawn up in increments of 0.15 mL and 0.3 mL in a 30 insulin-unit syringe (0.3 mL syringe) to equal 30U and 60U, respectively. These drawn syringes are the senior author’s most commonly used unit amounts, and a small fraction of the preset syringes are of smaller unit amounts for when needed.
Technique
Practitioner experience and an individualized treatment plan will determine the appropriate dose for each patient. Because each patient responds differently, the senior author initially treats each patient with the same number of units in each targeted site. In the next treatment visit, initial response is assessed and the subsequent treatments are tailored to that patient’s response. The reported onset and duration of action of the BoNT preparations are grossly similar with an approximate onset of 3 days and duration of action of approximately 3 months. However, newer studies suggest that the onset and degree of effect can vary between formulations. A split-face study comparing Botox and Dysport for the treatment of moderate to severe lateral orbital rhytids showed statistically greater improvement with Dysport at days 2 and 6 following therapy. 9 Recent studies and reports have noted that Xeomin may have a shorter onset of action compared to Botox. In terms of duration of action, a recent pilot study by the senior author has suggested that Xeomin has a dose-dependent duration of action of up to 7 months. Further studies will be required to determine whether Xeomin and other BoNT type A formulation have the potential indication as a long-acting neuromodulator. Myobloc, in contrast, has a shorter duration of action compared to the BoNT type A preparations. 6 , 7
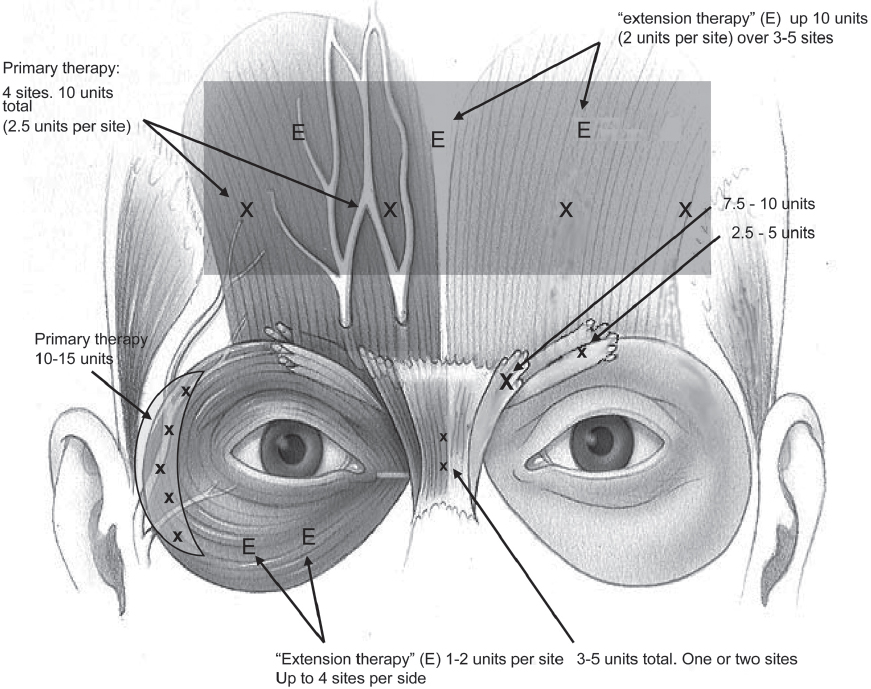
A thorough knowledge of the facial muscular anatomy ( Fig. 22.1 ) is imperative for the understanding of BoNT in facial aesthetics. Although many techniques are utilized, it is clear that an optimal response can be achieved using minimal dosages with proper placement in the muscle groups. However, because of the diffusion effects and favorable safety profile, the variability in injection points and dosages has not been shown to adversely affect patient satisfaction. It is important to know not only the specific muscle locations but also the functional interrelationships of the muscle actions as many act as antagonist-protagonists, such as in the position of the brow ( Fig. 22.1 ). By understanding the facial anatomy, one can use BoNT not just for wrinkles, but also as a treatment to reshape and soften certain facial features that can be associated with frowning, anger, or just simply aging.
History
A full medical history should be obtained at the initial visit prior to injection. Allergies and medications should be documented, and the patient should be counseled on the increased risk of bruising if they are taking any form of anticoagulation. Verbal and written consent should always be obtained after the patient has understood the risks, benefits, expectations, and alternative BoNTs, or any other treatments, available. Allergies or hypersensitivities to any of the formulation ingredients (BoNT type A, sodium chloride, human albumin) are contraindications for BoNT treatment. Neurodegenerative and neuromuscular disorders should be noted, as these are typically absolute contraindications to BoNT therapy as well. Any patient who is pregnant or breastfeeding should not undergo treatment, as this has not been studied. Patients and providers alike should be made aware of any preexisting lid or brow ptosis if present and educated on the risk of exacerbation. Although careful injection technique should minimize risk, there is always the possibility of worsening ptosis.
Physical Examination
A focused examination of the face should be performed, and preexisting rhytids, furrows, and asymmetries should be noted and discussed with the patient. The physical examination is also an appropriate time to assess the patient’s goals of treatment. The degree of improvement that can be reasonably expected following BoNT treatment can be assessed clinically by asking the patient to maximally contract the muscle group that is to be targeted such as the glabellar, corrugator, frontalis, orbicularis oculi, and platysma muscles.
Relevant Anatomy
A thorough comprehension of underlying facial muscular anatomy is critical to the successful and consistent improvement of hyperdynamic rhytids and overall facial aesthetics. Recommendations for starting treatment dosages as well as the starting treatment dosages of the senior author are summarized in Table 22.2 . 19
Related posts:






Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


