22 Genioplasty
Pearls
Genioplasty has no effect on occlusion and can thus be considered a wholly aesthetic procedure aimed at modifying the form and appearance of the bony mentum.
Genioplasty is most commonly done as an adjunctive procedure of anterior segmental osteotomy, angle reduction surgery, mandibular shaving, zygomatic surgery, and rhinoplasty to yield synergistic effects in making an aesthetically pleasing face.
Proper evaluation and documentation in the form of facial photography, simulation modeling, and radiographic investigations (panoramic view, lateral and posterior-anterior [PA] cephalogram, and/or 3D computed tomography [CT] scan) are imperative prior to surgery.
The objective is to achieve facial harmony through surgically modifying the mentum and mandibular symphyseal areas, recreating appropriate facial proportions and symmetry of the lower third of the face.
The ideal chin position varies among individuals, and is determined by taking into consideration both the hard and soft tissue cephalometry reference points.
Genioplasty can be performed in two ways: (1) osseous genioplasty and (2) augmentation genioplasty using implants. The authors prefer osseous genioplasty because it provides a more reliable outcome.
Osseous genioplasty is done intraorally under general anesthesia. Horizontal bone cuts are made bicortically with an oscillating saw, taking care not to injure the mental nerve, and the mobilized segment is fixed with pre-bent miniplates.
Although genioplasty is a relatively safe operation with very low complication rates, mental nerve injury, malunion/nonunion, irregularity of bone surface, lip drooping or skin dimpling, chin ptosis, and asymmetry may develop.
Introduction
The chin is vital in creating a sense of symmetry and proportion of the face. The features of importance in the chin include (1) the curvature from the inferior vermillion to the chin tip, (2) the volume of the chin bone, and (3) the position of the chin tip. Interestingly, the chin has a significant impact on the patient socially. Many patients with micrognathia or mandibular hypoplasia reveal a lack of confidence, introversion, and an inferiority complex. In this sense, the role of aesthetic surgeons extends beyond simple aesthetic enhancements and augmentations.
The concept of beauty borrows heavily on the individual’s cultural background and exposure. In East Asian traditions, a round and voluminous chin was preferred as the ideal. Nowadays, however, many female patients want a small face with a V-shaped chin instead of the big U-shaped chin of previous times. Most male patients also prefer a narrower, slightly longer and moderately prominent chin. We can safely assume that this trend will continue to evolve, and surgeons will have to stay current with the times and modify their techniques to suit the requirements of the contemporary aesthetic preference.
Genioplasty, while seemingly a relatively straightforward procedure, has a significant impact on overall facial harmony and attractiveness. This surgery is generally considered an adjuvant surgery, performed to enhance and complement other facial bone surgeries such as sagittal split ramus osteotomy (SSRO), anterior segmental osteotomy (ASO), mandibular angle reduction surgery, and malarplasty.
The most common indications for genioplasty are (1) small chin with class II malocclusions (with or without open bite or bimaxillary protrusion) and (2) big chin with class III malocclusion and an excessively long face. These problems are often a result of congenital syndromes (e.g., Treacher-Collins syndrome) or hereditary malocclusion, chin hypoplasia secondary to childhood osteomyelitis, chin deviation due to soft tissue contractures (e.g., burns), and anterior chin or temporomandibular joint growth center disruptions from trauma.
Historic Background of Genioplasty
Historically, genioplasty is performed in one of two ways: the use of onlay augmentation over the mentum surface, and the repositioning of the chin via osteotomies. G. Aufricht in 1934 described the use of the excised nasal hump as an autograft material “recycled” from rhinoplasty.1 In 1948, K. H. Thoma described the use of titanium mesh for genioplasty. Numerous materials had been experimented with throughout history with varying success, but as implant technologies advanced, so did the outcomes. Some examples of these include acrylic, wax, silastic chin implant (Brown et al 1953), expanded polytetrafluoroethylene (e-PTFE, or Gore-Tex [W. L. Gore]) synthetic implants, ceramics and hydroxyapatite, and demineralized granulated tooth (Auto BT) with BMP.
The concept of osseous genioplasty was first presented by O. Hofer in 1942. He utilized a three-step technique: segmental osteotomy, relocation, and fixation of the chin bone to the new position.2 Hofer described first creating a horizontal osteotomy of the anterior part (mentum) of the mandible via an extraoral submental incision to correct prognathism and micrognathia (Fig. 22.1a). H. Obwegeser (1957) later described advancement sliding genioplasty via an intraoral approach to avoid visible chin scars (Fig. 22.1b).3
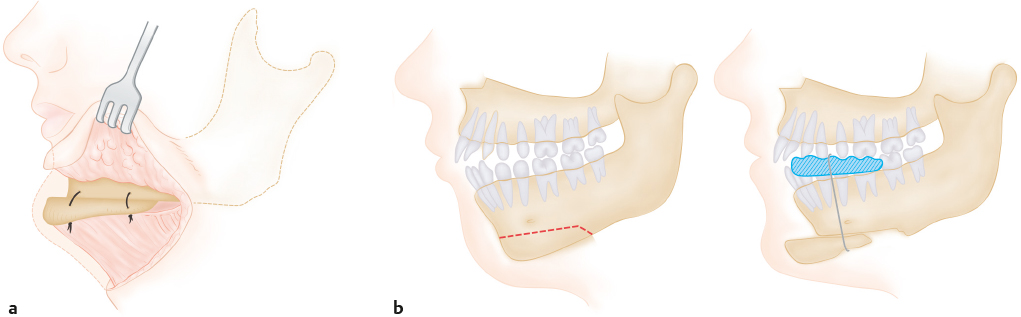
After osteotomizing the lower portion of the anterior mandible, this segment was pulled forward, pedicled on the geniohyoid muscle. He fixed the segment using perimandibular Supramid (S. Jackson) thread over the acrylic splint. Later Obwegeser switched to direct bone wiring. He also described modifications of his technique for asymmetric chins, by modifying the arc of the segment. With the exception of the fixation method, this technique is still widely used today. Further advances in the osteotomy designs in the horizontal, vertical, and sagittal planes resulted in greater control over the final appearance of the chin.
Essential Cephalometric Data for Genioplasty
The important norms for chin position in cephalometric analysis are summarized in Table 22.1 . The differences in cephalometric norms among various ethnic groups have been well documented through various comparative studies.4,5,6 The major difference in chin cephalometric parameters is the length of the lower face. In Koreans, Sp′–Gn (mm) is longer than it is, for example, in Germans (65.91 mm versus 63.27 mm, respectively). Thus, the ratio N–ANS/ANS–Me (79.5%) is lower in Koreans. This value is a useful guide for the calculation of the ideal vertical length of the chin. Other variables also showed significant differences (see Chapter 21, Fig. 21.4 and Fig. 21.5).
Variablesa | Norms (Asian) | Norms (Caucasian) |
N–Me (mm) | 118.8 ±4.5 | 115.7 ±4.5 |
N–ANS (mm) | 52.9 ±2.7 (45% from N–Me) | 52.4 ±3.0 (45% from N–Me) |
ANS–Me (mm) | 65.9 ±4.5 (55–56% from N–Me) | 63.3 ±5.5 (54–55% from N–Me) |
N–ANS/ANS–Me (%) | 80.5 ±5.7 | 83.2 ±6.2 |
S–N–A (°) | 82.0 ±3.9 | 81.1 ±4.1 |
S–N–B (°) | 79.4 ±3.5 | 79.0 ±3.5 |
G–Sn:Sn–Me′ | 1:1 |
|
Sn–St:St–Me′ | 1:2 |
|
aSee Chapter 21, Table 21.1 for a guide to variables. | ||
Patient Evaluation
Patient Consultation
It is important to inquire about the patient’s medical and family history. Sometimes patients may withhold significant details, such as previous filler injection or chin implant surgery, only to be revealed during routine preoperative radiologic examinations. This highlights the importance of a complete preoperative assessment including X-rays. It is also important to listen attentively and take note of the patient’s desires and expectations. The parameters discussed usually include (1) the volume and shape of the chin (small/large, broad/narrow, sharp/oval), (2) positioning of the chin tip on the sagittal plane (protrusion or retrusion), (3) vertical height of the chin (lengthening/shortening), and (4) symmetry (in all three planes).
Occasionally, the surgeon may encounter a patient having good chin shape, position, height, and symmetry but who requests surgery. In this situation, the surgeon needs to consider the patient judiciously.
The patient’s occlusion is also examined during the consultation. This is especially crucial in patients who have had previous orthodontic treatment or jaw surgeries. Generally, simple genioplasty alone is sufficient for a patient with normal class I occlusion. However, it will not suffice for proper aesthetic correction for patients with class II or III occlusions. In this case, orthodontic treatment or surgery (such as anterior segmental osteotomy or sagittal split ramus osteotomy) should precede genioplasty to correct malocclusion.
Patient Assessment
For preoperative assessment, analysis of facial photographs, including frontal, 45 degrees oblique, lateral, basal, and helicopter views, and smiling and pouting views, is the first step. It is crucial to obtain smiling and pouting photographs since some problems, such as skin dimpling, may appear only during pouting or smiling.
To determine the ideal soft tissue vertical dimension of the lower third of the face, various references may be used, such as (1) the Ricketts line (E-line), (2) the rule of thirds, (3) soft tissue divisions from the subnasale (Sn) to the soft tissue menton (Me′) and from the glabella to the soft tissue menton (see Chapter 21, Fig. 21.5), and (4) the concept of the “zero-meridian” (Gonzalez-Uloa, 1962).
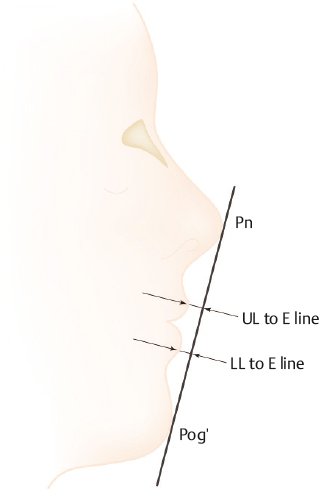
The “esthetic” line, or E-line, can be drawn from the nasal tip (pronasale) to the soft tissue pogonion (Pog′) to evaluate lip position (Fig. 22.2). The mean distance of the upper lip to the E-line is 0.41 mm in Asians and 4.72 mm in Caucasians; while the mean distances for the lower lip are 1.27 mm and 3.14 mm for Asians and Caucasians, respectively.4 Using these measurements, the position of the pogonion can be extrapolated. One pitfall to note is that this method relies heavily on the patient’s having a normally projected pronasale (nasal tip). Usually the pronasale is inadequately projected in Asians; thus, using this point as a reference in such patients can lead to an erroneous conclusion in identifying a retruded pogonion position.
The rule of thirds is also applied in the analysis of facial proportions. The face is divided into three equal vertical sections: The portion from the trichion (Tr) to the glabella forms the upper third, from the glabella to the subnasale the middle third, and from the subnasale to the menton the lower third (see Chapter 21, Fig. 21.3a). Asians are known to have a longer lower third than Caucasians by ~ 2 to 3%. This method of proportional analysis may be used to determine the ideal position of the soft tissue menton (Me′) (Fig. 22.3a). In addition, further analysis of the lower third can be made by studying the positions of the subnasale (Sn), stomion (St), lower lip (LL), and soft tissue menton. The ratio of the distances Sn–St:St–Me′ is 1:2, and that of the distances Sn–LL:LL–Me′ is 1:1 (Fig. 22.3b). In patients with small chins, the Sn–LL:LL–Me′ ratio will be more than 1. Using these ratios of the lower facial third, the optimal position of the soft tissue menton can be calculated.
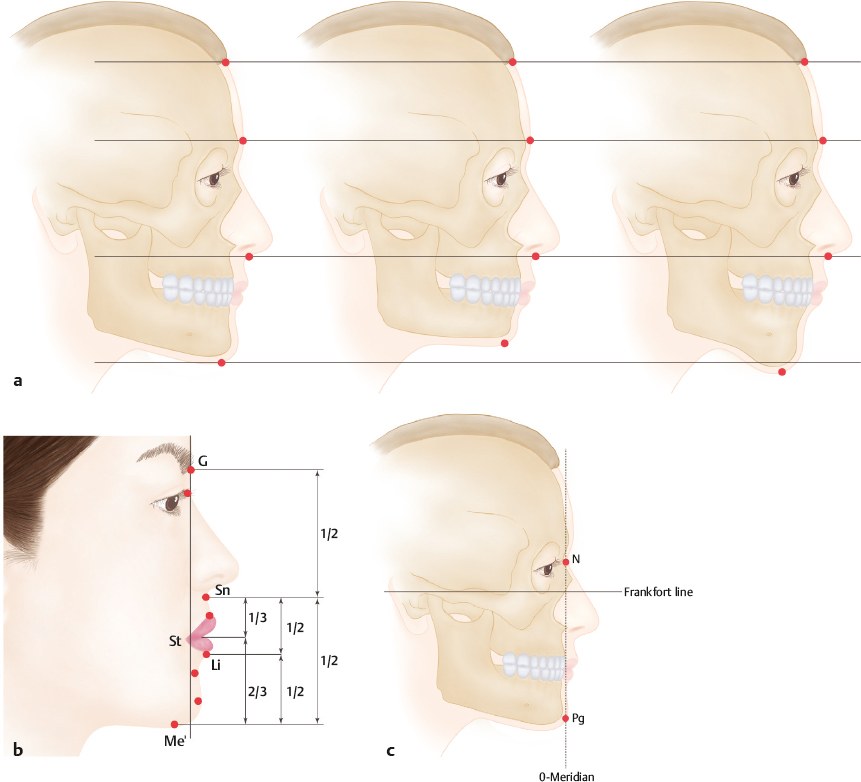
The concept of zero-meridian was described by Gonzalez-Ulloa in 1962.8 From the soft tissue N point, a line perpendicular to the Frankfort horizontal line (FH line), the line from the upper rim of the external auditory canal to the lower rim of the orbit, is drawn. This is known as the zero-meridian. The soft tissue pogonion is located along the zero-meridian (Fig. 22.3c).
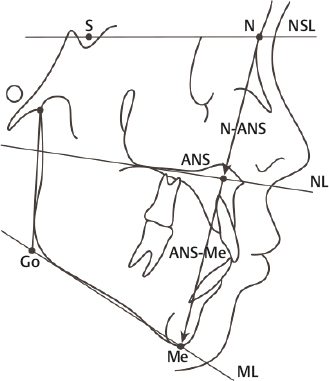
Imaging analysis including X-ray (panoramic view, Cephalo PA, Cephalo Lat) or 3D CT scan is also a necessity. In the planning of the ideal position of the chin tip (Me or Pog), it is useful to bear in mind that proportion is more important than the actual length. Lateral cephalometry is perhaps the single most informative tool in assessing and determining the position of the chin. The anteriorposterior chin projection (Pog) is determined on the sagittal plane by locating it between the SNA and SNB lines. The nasion (N)–anterior nasal spine (ANS)/anterior nasal spine (ANS)–menton (Me) ratio is the most frequently used parameter to assess the adequacy of the vertical height of the chin (Fig. 22.4). These parameters are the norms for reference; however, depending on the patient’s preference, the final chin position may be adjusted to within 6% of this reference figure safely.
In practice, it is important to remember that the soft tissue does not move at the same magnitude as its underlying repositioned bone. For example, a 5-mm advancement of the chin bone usually results in soft tissue advancement of ~ 75% of that. In vertical lengthening and shortening of the chin, however, soft tissue follows bone more closely, on the order of ~ 90%.
Related posts:





Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


