19 Zygoma Reduction
Pearls
The aim of zygoma reduction is to reduce the width of the cheekbone, thus changing the boxy flat facial shape into a threedimensional contour and achieving a smooth, feminine facial line.
Bizygomatic width and volume and the position of the zygomatic body are the key variables to be evaluated, and the amount of body ostectomy is determined during the surgery.
The zygomatic body and arch are usually moved medially, posteriorly, and sometimes superiorly during the surgery; the point of maximal malar projection is marked and its new position carefully planned.
In zygoma reduction overall facial shape, including mandible prominence and facial height, should be considered. Caution should be taken for patients with a long face, as there is a risk for the face to appear longer after the surgery.
Reduction malarplasty can be performed solely or in combination with mandible reduction, genioplasty, or forehead augmentation.
Soft tissue plays a great role in reduction malarplasty. In patients with abundant cheek fat, the slimming effect is less obvious and cheek drooping is more probable.
The following five factors are considered high risk for skin and soft tissue sagging: (1) over 40 years of age, (2) abundant cheek fat, (3) thin skin and skin laxity, (4) class II mandible or ill-defined mandible neck line, (5) deep nasolabial fold or jowl.
Introduction
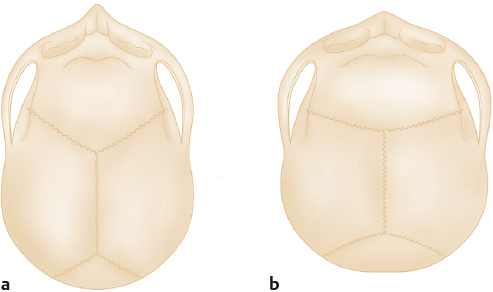
Asian people tend to have a shorter and wider facial contour compared with Westerners. The prominent malar complex combined with the protruding angled part of the lower jaw creates a boxy rather than ovalshaped face. When viewed from below, the flat midface and wide cheekbones also create a boxy appearance. These facial characteristics are typical of the Mongoloid face (brachycephalic face), while the Caucasian face is slim and protruding in an anteriorposterior dimension (dolicocephalic face) (Fig. 19.1). Conventional standards of beauty vary across different cultures and ethnicities. However, aesthetic standards in the countries of East Asia have become more “global” and influenced by Caucasian standards. Asians seek a slimmer face with a threedimensional appearance.
This discrepancy in racial characteristics and changes in beauty standards led to a rise in individuals desiring to change their facial contour and shape. In East Asian countries such as Korea, China, and Japan, facial contouring surgery is very popular and commonly performed to attain a more slender and smooth facial contour. Recently, this trend has spread to other parts of Asia and among the Asians living in Western countries.
However, simply changing the Mongoloid face into a Caucasian face does not guarantee a satisfactory result in Asian countries, because Asians have different aesthetic goals and different cultural backgrounds. For example, prominent high cheekbones are considered a symbol of youth and admired in Western countries. However, the same prominent cheekbones are considered aesthetically unpleasing for Asian women as this feature gives a harsh, strong impression. Therefore, before the surgery, surgeons should be well aware of the goals of zygoma reduction in Asians.
Patients who seek zygoma reduction are those who desire a slim and slender oval face when viewed from the front. People with a brachycephalic face characterized by a flat forehead and midface describe their face as boxy in shape. They desire a threedimensional and voluminous face. People with prominent high cheekbones complain that they look “too strong,” “offensive,” “old,” “tired,” and “masculine,” and they want to change their faces to have a more “soft,” “young,” and “feminine” appeal.
The objectives of zygoma reduction are as follows:
Reduction of facial width for slender facial contour. First and foremost, the aim of zygoma reduction is to acquire a more slender and narrow facial contour. Usually facial width is determined by the bizygomatic distance which links the articular tubercles on the two sides. Reduction or transposition of the zygomatic arch is an effective method to reduce facial width. As the zygomatic body is usually hypertrophied together, reducing only the zygomatic arch may lead to a boxy appearance; thus, combined and harmonious reduction of arch width and zygomatic body is essential.
Change a boxy flat facial shape into a threedimensional contour. Even if facial width is reduced, the face can still appear square.1 Asian faces have a brachyfacial characteristic with a flat suborbital area. When viewed from below, the lack of malar projection results in the suborbital area and zygomatic arch forming a 90-degree angle that lends a boxy appearance. In this case, the face appears flat and two-dimensional, and even wider than it appears from the front. Therefore, changes in the shape and position of the zygomatic body are needed to create a midface fullness that appears more threedimensional and youthful.
Attain a smooth facial line that looks more feminine and young. An angular face line needs to be made soft. In the case where the cheekbones protrude outwardly, the facial line connecting the templezygoma-cheek-mandible angle constitutes a very convoluted line (Fig. 19.2). In the case of Westerners, prominence of the zygomatic body is a symbol of beauty and youthfulness. However, for Asians this prominence results in an obstinate and masculine look, which gives a negative impression. High cheekbones are not an ideal look in Asian cultures; therefore, reduction is needed to make the face soft and feminine. For those over the age of 35, facial soft tissue decreases and skin starts to droop; malar eminence looks even more pronounced and causes grooves in the cheek and temple, gradually resulting in a tired and aged look. Fat injections to such hollow areas can be an easy option, but the result is not predictable or permanent. Zygomatic reduction is a good option for the middle-aged woman who desires a youthful, soft, and feminine facial contour.

Patient Evaluation
Direct physical examination is the key process to evaluate the patient’s problems and establish a surgical plan. Clinical photos are necessary, as is radiologic examination including frontal view, lateral view, submentovertex view, and Waters’ view. A computed tomography (CT) scan with 3D view is also essential to evaluate the shape of the zygomatic complex.
The volume and position of the zygomatic body, and the bizygomatic width are key variables to be considered. The volume of the zygomatic body determines the amount of ostectomy required during the surgery. If the volume is large, a wider resection of the zygomatic body should be planned. However, over-zealous reduction results in a flat or deficient look. Therefore, keeping an adequate volume of the zygomatic body in the antero-posterior dimension and transverse plane is essential.
The position of the zygomatic body is measured both at its most lateral margin and in its maximal projection. The outer margin of the zygomatic body is observed in conjunction with temple and cheek. To narrow the anterior midfacial width, the lateral margin of the cheekbone should be trimmed or moved inward. If the outer margin of the cheekbone is placed wide, the amount of narrowing and medialization should be maximized and ostectomy should be combined.
The point of maximal malar projection (MMP) is the point where the outer contour of the zygomatic complex protrudes most in the basal threequarters view. If the reduction of the zygomatic body is performed by shaving, or the osteotomy is placed lateral to the MMP, this point stays unchanged while the outer margin of the zygomatic body is narrowed, resulting in an unnatural, box-shaped cheekbone. As stated before, the purpose of reduction malarplasty is not resection of the projection; therefore, adequate projection and position of the MMP is the key postoperative result. The point of MMP is marked and the surgeon decides where to move this point threedimensionally. The amounts of medial repositioning and ostectomy are closely related to the reduction of anterior facial width.
The ideal position of the MMP may vary among different ethnicities; however, the following are two simple methods of determining the ideal position of the MMP (Fig. 19.3).
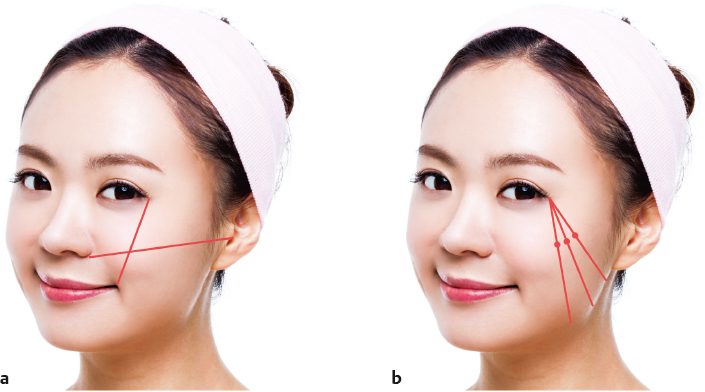
Hinderer analysis. The MMP is determined at the point of intersection of two lines, where the first line connects the lateral canthus and the oral commissure, and the second line connects the nasal alar base and the tragus line. The new location is a point placed in juxtaposition to the crossed lines in the upper outer quadrant.2
Wilkinson analysis. A line is dropped vertically downward from the lateral canthus to the inferior border of the mandible. The MMP is located at one-third the distance from the lateral canthus to the angle of the mandible.3
Once the surgical variables for the zygomatic body are evaluated, the bizygomatic width is measured, and the required amount of arch medialization, which is critical in the reduction of posterior facial width, should be decided. The posterior basal portion of the arch, which is posterior to the osteotomy, cannot be medialized and should be carefully shaved to prevent visible step. Too much arch reduction with the remaining zygomatic body will result in a flat, boxy face. To avoid this outcome and create a full midface contour, the reduction of the zygomatic body and arch should be coordinated and balanced.
There are many variables that need consideration during surgery, and these should be decided by the abovementioned evaluation. Variables of the zygomatic body are (1) amount of ostectomy, (2) amount of medialization, (3) amount of setback, and (4) superior or inferior positioning. Variables of the zygomatic arch are the amount of arch medialization and the shaving quantity of the posterior area of the articular tubercle.
Facial soft tissue is an important aesthetic component in zygoma reduction and should be considered before and during the surgery. If the patient has thin fair skin with minimal cheek fat, the changes after bone surgery will be obvious and the chance of soft tissue drooping is minimal. This patient is a good candidate for zygoma reduction. However, bony step, especially around the orbit, may be visible and the plate may be palpable through the thin skin. Surgeons should take extra effort to ensure a smooth transition between bony osteotomy. If the patient has abundant cheek soft tissue, or thick skin, there is a high risk of cheek drooping. The patient should be informed about the possibility of cheek drooping and appropriate adjunctive measures, including liposuction or lifting procedures. If the patient has a thick malar fat pad, the zygomatic body should be slightly over-corrected to prevent under-correction.
Overall facial shape, including mandible prominence and facial length, should be considered (Fig. 19.4). Zygoma reduction can be performed solely or in combination with mandible reduction. If the patient has a prominent mandible, reduction malarplasty alone may not be able to balance bigonial and bizygomatic width, and combined mandible reduction should be recommended. If a patient has a long face with prominent cheekbones, a reduction in bizygomatic distance deteriorates the excessively narrowed long face and leads to “cucumber face.” It is advisable to focus on the setback of the zygomatic body instead of the medialization of body and arch, and selectively create a soft facial contour.
Related posts:





Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


