20 Mandible Reduction
Pearls
“Angle reduction” is the old name for this procedure and represents a major misconception regarding what the surgery is for. The purpose of mandible reduction is to make the lower face appear slim in the frontal view and to achieve a smooth contour in the lateral view. Changing the mandibular plane and contouring the whole lower border of the mandible are critical steps. On the other hand, angle reduction with removal of triangular bone will inevitably leave an unnatural lower contour of mandible with a secondary angle.
Because shaping the lateral contour of the mandible alone may result in minimal improvement in the frontal view, surgical techniques to reduce the width of the lower face via burring or ostectomy of the lateral cortex should usually also be done.
The chin plays an important role in creating a beautiful facial line and overall contour; therefore, genioplasty should be considered in continuity with mandible reduction.
The relationship between the maxilla and the mandible in profile view should be observed. In class II, or class III profile, orthognathic surgery is first considered. However, in patients with mild deformity, or in patients who do not want orthognathic surgery, mandible reduction should be planned to prevent the existing problems from deteriorating.
The inferior alveolar nerve is the most important structure during mandible reduction, and it should be carefully examined preoperatively in panoramic view as well as in a computed tomography (CT) scan. It is typically located at least 20 mm away from the upper border of the mandible, which should be kept in mind when designing and conducting the osteotomy. The most common cause of paresthesia is not a direct cut but a blunt injury to the nerve by retractors coming out of the mental foramen. Osteotomy should be conducted at least 3 mm away from the mental foramen.
The incidence of major intraoperative hemorrhage has decreased due to advances in surgical technique and the use of a hypotensive anesthetic protocol. If the retromandibular vein or the facial artery is torn during a procedure, adequate hemostasis with electrocautery may not be easy, and this may lead to excessive blood loss. Application of hemostatic substances and external manual compression for more than 30 minutes can help to stop the bleeding.
Following the completion of surgery, the soft tissues of the cheek and the neck should be checked for any signs of bleeding or swelling. Any sign of swelling or bleeding near the throat is a serious complication and should be treated immediately as it may cause breathing problems.
Introduction
The overall Asian facial structure is typically classified as brachycephalic or mesocephalic, with a widened mandibular arch and broad lower facial skeleton. In countries such as Korea, China, and Japan, these characteristics are often viewed as masculine and unattractive; thus, both men and women often wish to make their faces appear more slim and slender.
The width of the lower third of the face is determined by the width of the mandible itself, which is surrounded by muscles and subcutaneous fat tissues. Generally, the cause of prominent mandibular angle in Asians is the lateral protrusion of the mandibular angle rather than soft tissue contribution such as hypertrophied masseter muscle.1,2 Anthropologic studies have shown significant quantitative facial anthropometric differences among different ethnic backgrounds; one such difference being that Koreans, in comparison to Caucasians, tend to have a more developed lower face.3 In addition, the average bigonial distance in Caucasian women is 105 to 109 mm,4,5 whereas in Korean women the average distance is 118 to 125 mm.3 Since Koreans have a greater bigonial distance and more flared mandibular angle, they often undergo mandible reduction to slenderize the lower facial contour, whereas Caucasians prefer mandible augmentation to correct weak jaw lines.6
Resection of the Mandibular Angle
In 1949 Adams introduced a surgical technique for resecting mandibular bone and masseter muscle via the transcutaneous approach, and Converse performed the same procedure through an intraoral approach in 1959.7 In 1989 Baek introduced mandibular angle reduction for Asian patients via the intraoral approach. In 1991 Yang and Park introduced a surgical technique for contouring the mandibular body and the symphysis with a sequential resection of the bone. Since the late 1990s one-stage, long curved ostectomy has been widely used to contour the mandible.8
Narrowing the Width
The conventional ostectomy, which resects the inferior border of the mandibular angle and body, can bring a satisfactory contour from the side view; however, it fails to show improvement in the frontal facial contour due to its inability to narrow the broad lower face. To achieve the desired appearance of the frontal view facial contour, a variety of surgical techniques were developed. In 1997, Deguchi et al reported that the width of the lower face could be narrowed by a technique that shaves the lateral cortex anterior to the inferior alveolar nerve and splits the angle posterior to the nerve.9 In 2001 Han and Kim effectively reduced the bigonial width through lateral cortex ostectomy without a mandibular angle reduction.10 In 2004, Hwang et al introduced simultaneous utilization of the two different techniques.11
Creating an Ideal Shape and Adding Dimension to a Flat Face
Although the previously mentioned mandible reduction techniques have many advantages, they fail to correct the broad and blunt appearance of the chin. The chin is a major determinant of an attractive lower facial contour. Thus, the authors have reported that narrowing the width and modifying the shape of the chin, in conjunction with mandible reduction, is essential to achieve a slimmer and ovalshaped contour.12,13,14 The authors’ current techniques for a prominent mandible are (1) controlling the slope of the mandibular plane by resecting the mandibular angle and controlling the inferior border of the body via a long curved resection technique, (2) reducing the width of the lower face via burring or ostectomy of the lateral cortex, and (3) narrowing genioplasty according to the patient’s specific demands. Since the authors introduced the technique in 2008, simultaneous performance of narrowing genioplasty and mandible reduction has been widely called “V-line surgery” since the shape of the contoured jaw line looks like the letter V (Fig. 20.1).
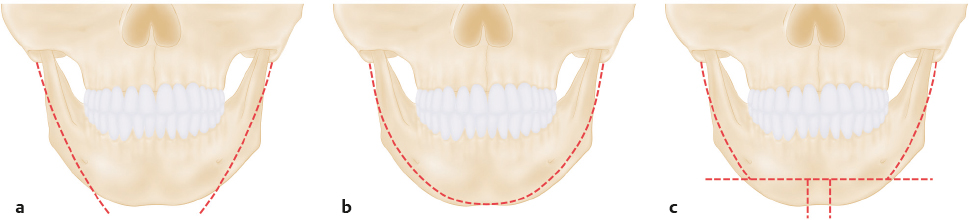
V-line surgery not only narrows the width of the mandible and contours the jaw line, but also reduces the size and controls the position of the chin in both the vertical and anteriorposterior directions, making a smaller and more feminine oval facial contour possible.
On the basis of technical perfection, the establishment of appropriate surgical indications for each technique is mandatory to achieve aesthetically pleasing results. Analysis of the individual’s entire face should come from a thorough understanding of lower facial types. The authors classify the shape of the lower face according to the shape of the chin, which is helpful in establishing the treatment plan (Fig. 20.2).15

Patient Evaluation
Diagnosis
The condition may easily be diagnosed by clinical findings and radiologic examination. The degree of protrusion of the mandible, asymmetry, masseter muscle hypertrophy, and amount of the subcutaneous fat should be evaluated. The degree of hypertrophy of the masseter muscle can be identified by palpating the tightened versus relaxed status of the jaw. Hyperostosis, mostly around the mandible angle, is noted in the radiologic studies. Two-thirds of the cases show mild to moderate increase in bigonial distance due to lateral flaring of the mandible angle. However, the remaining third shows total mandibular hypertrophy and accentuated square contour of the whole lower face.
The shape and width of the lower face in the frontal view can be classified as in Fig. 20.2 . The profile as well as the height of the chin should be taken into consideration. The status of soft tissue including muscle and fat should be considered as well.
Preoperative Evaluation and Surgical Planning
The author routinely obtains a patient’s photographic documentation and radiologic examination that includes panoramic view, skull lateral view, postero-anterior (PA) cephalogram, and 3D CT image. For precise surgical planning and prevention of postoperative asymmetry, threedimensional analysis of the photographs and the radiographs in the frontal, sagittal, and transverse planes is important. Examination of the shape and symmetry and understanding the overall balance of the face are mandatory.
Frontal Plane
Using the PA cephalogram and 3D CT, the degree of protrusion or flaring of the mandible angle, symmetry, convexity of the body, deviation, and shape of the chin should be examined. The amount of narrowing and lateralization (considering the degree of asymmetry), and the amount of angle and inferior border resection are determined after checking the course of the inferior alveolar nerve. A panoramic view is helpful in determining the amount of ostectomy of the mandibular angle and body, as well as the position of its ostectomy line.
Sagittal Plane
Using the lateral cephalogram, the gonial angle, the mandibular plane–sellar nasion angle (MP-SN angle), and the vertical and anteriorposterior position of the chin should be identified. The ideal gonial angle is within the range of 105 to 115 degrees, and the MP-SN angle is 30 to 40 degrees. After measuring and understanding the accurate balance of the upper and midface, the amount of reduction, lengthening, and vertical/horizontal advancement or retrusion (setback) of the mandible in the anteriorposterior direction will be determined.
Transverse Plane
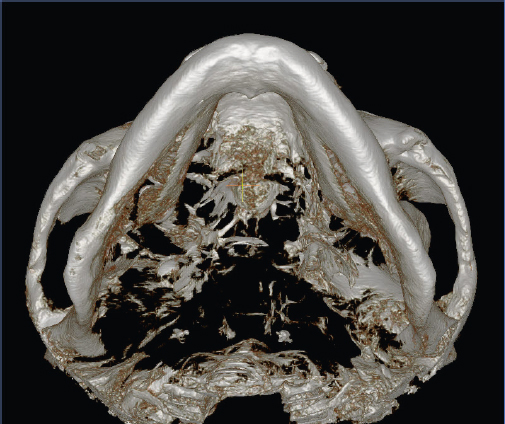
Three-dimensional CT or the cervical-vertex view is used to identify the transverse shape of the mandible (Fig. 20.3). The angle of divergence and convexity of the mandible are observed. In cases with an inward-curled angle with a convex transverse shape, sagittal resection of the body will help to reduce the width of the mandible more effectively.
Consideration in Surgical Planning
The Chin
The term chin refers to both the bone and the surrounding soft tissues. The chin is a very important component in lower facial morphology, and full attention should be given to the procedure of lower facial contouring surgery. In some patients, resection of the mandible alone does not make the face appear slender. This is mainly attributed to a wide, flat chin and a U-shaped lower facial morphology. Therefore, to create a slim and attractive face, reducing the width of the chin and modifying its shape and position is necessary in addition to resection of the mandible. The amount of central resection should be individualized depending on the width of the chin and the patient’s need. In the authors’ practice, resection of the central strip ranges from 6 to 12 mm (average 9.1 mm). In most cases, this amount of resection produces the desired shape and width of the chin. Advancement or setback (retrusion) of the chin should also be considered if a change of profile is required. The ideal aesthetic chin position should be determined in the profile view, considering the positions of the nasal tip and the upper and lower lip. However, critical decisions with regard to the chin position are made when viewing the patient “face to face,” considering the varying perspectives in repose and with broad smile.
Abnormal Skeletal Relationship between the Maxilla and Mandible
The relationship of the mandible with the maxilla should be understood, because not all patients have a normal intermaxillary skeletal relationship. In cases with protruding mandible showing class III occlusion, or those with relative underdevelopment of the lower jaw showing class II occlusion, orthognathic surgery may be needed to improve this disorder. If mandibular contouring surgery is to be done without correcting class II or class III skeletal problems, certain characteristics should be considered to avoid aggravating the intermaxillary problems. In cases with prominent mandible showing a skeletal class III relationship, a long jaw line may appear more accentuated if the angle is resected too much during mandible reduction. Therefore, the angle should be conservatively resected and sagittal shaving should be properly performed to minimize aggravation of prognathic appearance. In patients with a retruded mandible showing a class II profile, excessive resection of the mandible angle causes a more obscure cervico-facial line. Therefore, conservative mandible resection and maximal sagittal shaving of the body of the mandible, combined with advancement genioplasty are recommended. In a long face, angle resection should be performed in a limited way to prevent the aggravation of steep mandibular plane.
Related posts:






Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


