21 Aesthetic Orthognathic Surgery
Pearls
Orthognathic surgery is a dual-pronged operation that fulfills both functional and aesthetic goals through repositioning of the maxilla and/or mandible via orthodontic and surgical manipulation. Functional restoration should take precedence over aesthetic considerations.
The psychological impact of orthognathic surgery should be emphasized in the preoperative evaluation. It is recommended that significant others attend the preoperative discussion with the patient.
Understanding of malocclusion is important for proper functional rehabilitation. However, restoring normal occlusion does not necessarily ensure a good aesthetic outcome.
Pure orthodontic compensation treatment is sometimes about moving the teeth in the opposite direction to the surgical movement. Hence, it is important for the orthodontist to be able to recognize which patients will eventually require surgery, and thus avoid a painful detour to a trial of orthodontics that produce no benefit.
Temporomandibular joint positioning should be assessed first as the condylar position is the key reference point of the mandible. Masticatory muscle function and facial nerve function should also be checked before treatment.
High sagittal supraforaminal osteotomy is superior to sagittal split ramus osteotomy not only because it requires a shorter operating time, has less bleeding tendency, and is less invasive, but also because it has the lowest risk of inferior alveolar nerve injury.
Adequate soft tissue protection, meticulous hemostasis, rigid fixation, proper preoperative planning, and good surgical skills are the key tenets for a successful facial bone surgery.
“Aged appearance” can result from the relaxed midfacial soft tissue following LeFort I or bimaxillary surgery, and may require additional aesthetic procedures.
Introduction
“Orthognathic surgery” literally means “correctly (ortho-) positioned jaw (gnathic).” It refers to the surgical correction of abnormal mandible, maxilla, or both. Abnormal dentofacial development or asymmetry may not only result in an unaesthetic face and functional deterioration, but also can lead to psychosocial problems. Thus the objective of this surgery is to restore both function and aesthetics. Functional restoration refers to reinstating the functions of occlusion, mastication, swallowing, temporomandibular joint (TMJ) function, speech, and phonation. Aesthetic improvement involves the re-establishment of facial symmetry and harmony. The former should always be prioritized over the latter. Ultimately, it is hoped that the functional and aesthetic improvement will encourage the resolution of any psychosocial issues.
In the authors’ decades of experience with more than 3600 orthognathic surgical cases, 96% percent of the patients reported that they overcame their inferiority complex following orthognathic surgery. Their new-found confidence could be seen on their faces a month after surgery. Recently, there has been an emerging trend of performing a two-jaw surgery (maxillary Le Fort I operation with mandibular setback) on patients with normal occlusion for purely cosmetic reasons. In the authors’ opinion this is unacceptable. Surgeons must be wary of the commercialization of medicine and of the fine line between ethics and economics, and never lose sight of the sacred nature of their job.
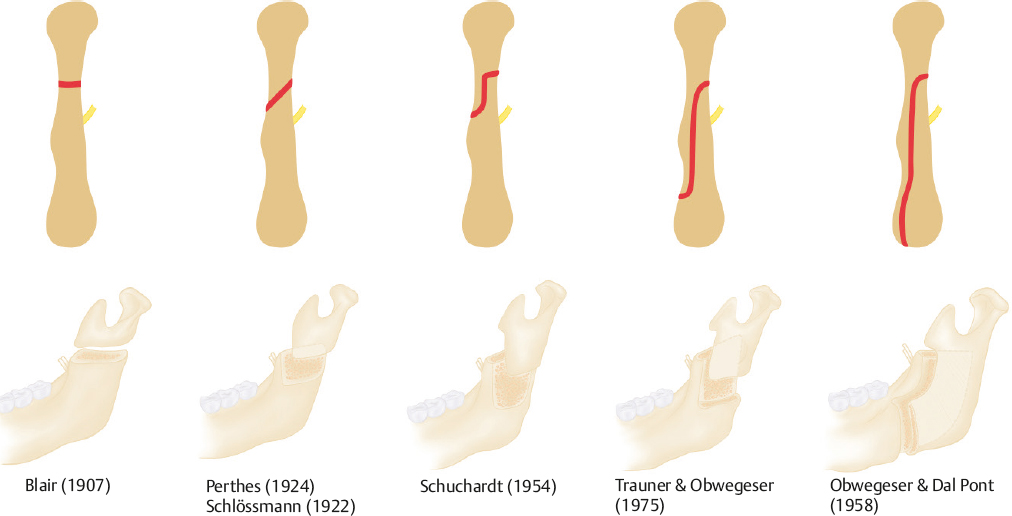
During orthognathic surgery’s history of more than 170 years, many surgeons have tried to set the concept of operation to achieve these purposes.1,2 Technically, the site and design of osteotomy, the approach for the osteotomy (extraoral or intraoral), the method for fixation (with wire or with plates and screws), and the emergence of the bone expansion and distraction osteogenesis techniques are among the innovations (Fig. 21.1).3,4,5 Since 1960 orthognathic surgery has made rapid progress alongside the advancements in technology such as the fixation plate and screw system for rigid fixation. Information technology (IT) development with software and 3D cone beam computed tomography (CT) and printing technology also have contributed to the improvement of analysis and diagnosis.
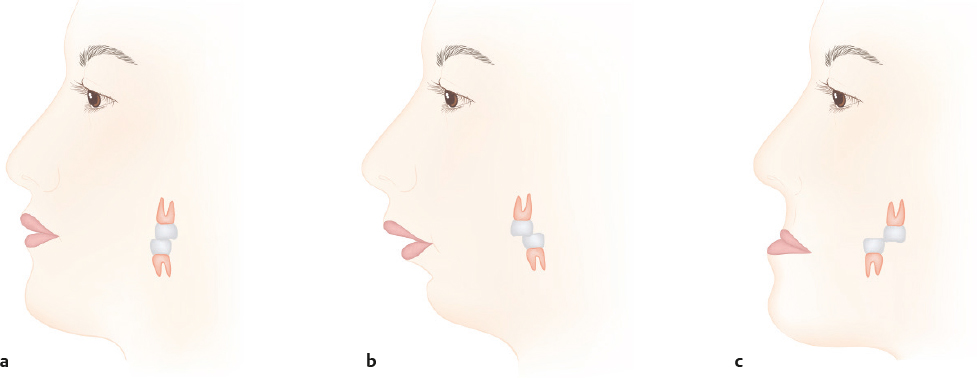
To approach orthognathic surgery, an understanding of the basic concept of occlusion is crucial since restoration to normal occlusion is the overriding priority of all orthognathic surgeries. It is therefore of utmost importance that the surgeon first be well informed on what constitutes normal occlusion. In normal occlusion, the mesiobuccal cusp of the upper first molar is received in the groove between the mesial and distal buccal cusps of the lower first molar. Anteriorly, the upper canine should occlude between the lower canine and first premolar. Angle classified the malocclusion into three classes with respect to the dental alignment and interrelationship of maxillary and mandibular arches and bones (dento-skeletal) (Fig. 21.2).4 Class I malocclusion is defined as having a normal molar occlusion between the upper first and lower first molars but problems with the other teeth, such as rotation or malpositioning. Class II malocclusion involves cases where the lower first molar is occluded distal to the upper first molar. This is subdivided into two divisions: Division 1 is where the upper incisors are proclined, increasing the overjet; division 2 is for cases with retroclined incisors, with reduced overjet. Class III malocclusion describes the lower first molar as being occluded mesial to the upper first molar. According to Angle’s classification, it was found that class I is the most common occlusion pattern across all races. However, Japanese persons were found to have a significantly greater percentage of class II relationships (15%), while class III relationships are highest among the Chinese population (34%).6
The modern interpretation of Angle’s classification is confined mainly to the anteriorposterior relations (on the sagittal plane), omitting information on the vertical and transverse planes. In practice, the ideal occlusion can be described as having (1) class I molar and canine relationship; (2) no crowding, no spacing, no rotation; (3) overjet ~ 2 to 4 mm; (4) correct crown angulation and inclination; (5) flat and slight upward curve of Spee; and (6) upper and lower midlines that are in alignment. Malocclusion should be analyzed with respect to intra-arch and inter-arch problems. Intra-arch problems are related to individual teeth—sagittally and vertically rotated, or transpositioned. Inter-arch problems are related to the intermaxillary problems, which occur on three planes: (1) class II or III malocclusions in the sagittal plane; (2) cross-bite, scissor bite, or midline shift in the transverse plane; and (3) deep bite or open bite in the vertical plane.
Patient Evaluation
The goal of consultation is to determine what a patient wants (chief complaints) and his or her concerns regarding function and aesthetics. Past medical and dental history (especially orthodontic treatment) is particularly important. The psychological state of the patient should also be evaluated during the interview. If the patient appears to have obsessive-compulsive tendencies, extra care should be taken before the surgery. The psychological impact of orthognathic surgery should be discussed with the patient before surgery. It is recommended that significant others, including family members, also attend the preoperative discussion. In bimaxillary protrusion patients, who have the greatest risk of postoperative “aged face,” it is wise to warn them about the possibility of additional aesthetic procedures because of the increased skin redundancy after surgery.
Documentation of any temporomandibular joint (TMJ) symptoms such as clicking, deviation on mouth opening, and associated headaches should be recorded. In particular, preexisting TMJ dysfunction prior to surgery should be addressed before orthodontic treatment, as the condylar position is the key reference point of the mandible. The range of motion and any deviation on mouth opening should be carefully documented. Masticatory muscle function and facial nerve function should also be checked before treatment.
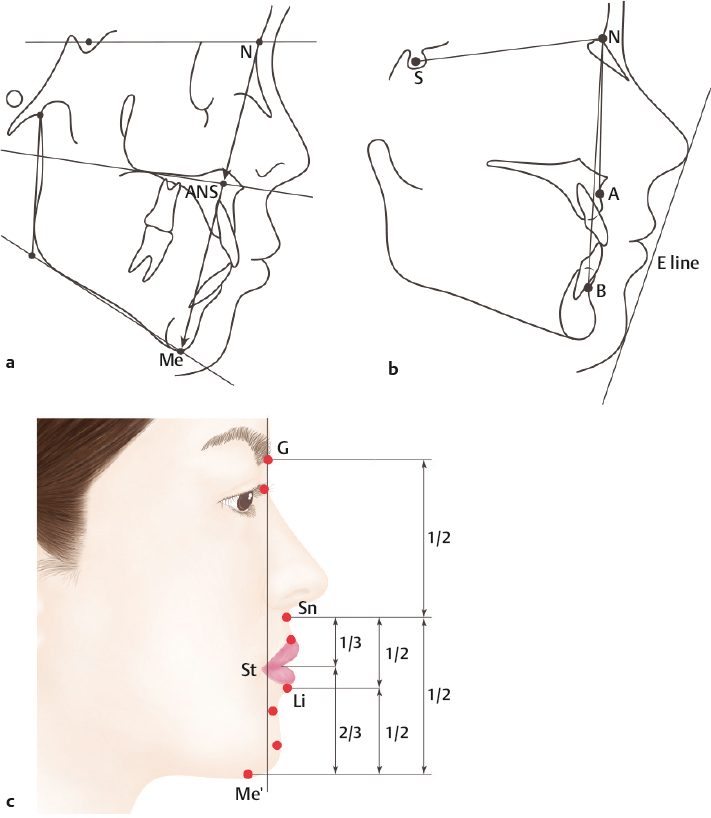
Harmony and symmetry are the key factors determining facial aesthetics, even though it should be recognized that what defines a beautiful face can differ according to sociocultural factors. In the frontal view, the face can be divided equally into the upper third (trichion to glabella), middle third (glabella to subnasale), and lower third (subnasale to menton) (Fig. 21.3a). Vertically the frontal plane is composed of equal fifths (rule of fifths) (Fig. 21.3b).
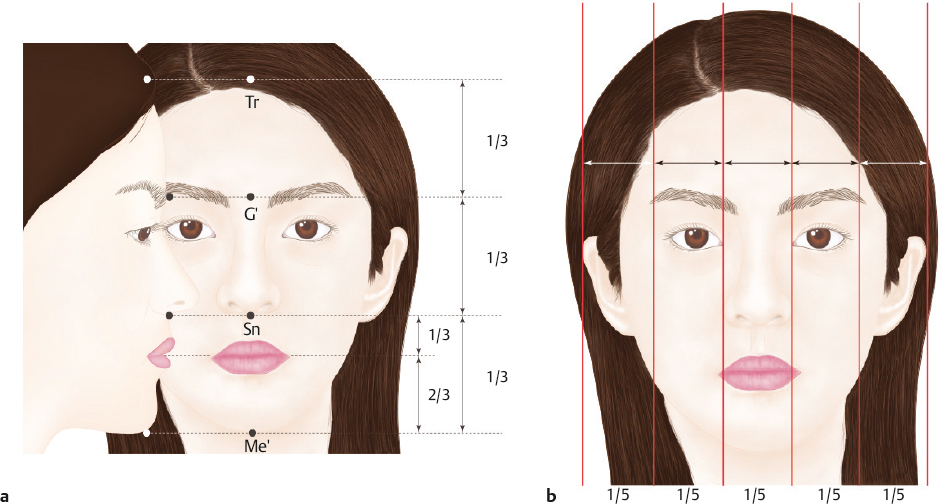
The central fifth is the distance between the medial canthi (which is equivalent to the alar base width). The outer two-fifths is the distance between the outer canthi and the outermost point of the ear. A vertical line from either outer canthus indicates the ideal vertical position of the gonion (mandibular angle) on both sides. The facial height-to-width ratio (facial index) is optimal when it approaches 1.35:1 for males and 1.3:1 for females. The facial height is the distance between the soft tissue nasion and menton. The facial width is defined by the bizygomatic width—the distance between the outermost points of the soft tissue zygomatic arch. The bitemporal width and bigonial width should approximate 80 to 85% and 70 to 75% of the bizygomatic width, respectively (refer to Fig. 19.4).
Lip projection is also a determining factor of facial aesthetics. Asians usually have distinctive characteristics of the lip due to a combination of thickness, bimaxillary protrusion, and labioversion of the upper and lower incisors. The ideal upper lip should be balanced with the nose and cheek, and the lower lip should be slightly posterior to the upper lip. The amount of teeth exposure depends on the vertical height of the maxilla. When both lips are in repose, the vermillion of the lower lip should be ~ 25 to 30% more exposed compared with the upper lip. This is especially important for orthognathic surgery for a cleft lip-palate patient. When smiling, the incisors should be at least threequarters exposed yet not exceed 2 mm of gingival show. A gummy smile, or excessive gingival show during smiling, is not a reliable indicator of the adequacy of maxillary height. Finally, facial symmetry can be assessed based on several relationships, involving the midsagittal plane through the nasal tip, midline of the upper and lower incisors, midline of the symphysis of the chin, and the gonion position of either side. Dynamic symmetry can be assessed by observing the level of the oral commissures and teeth exposure on smiling. Occlusal plane canting should also be assessed.
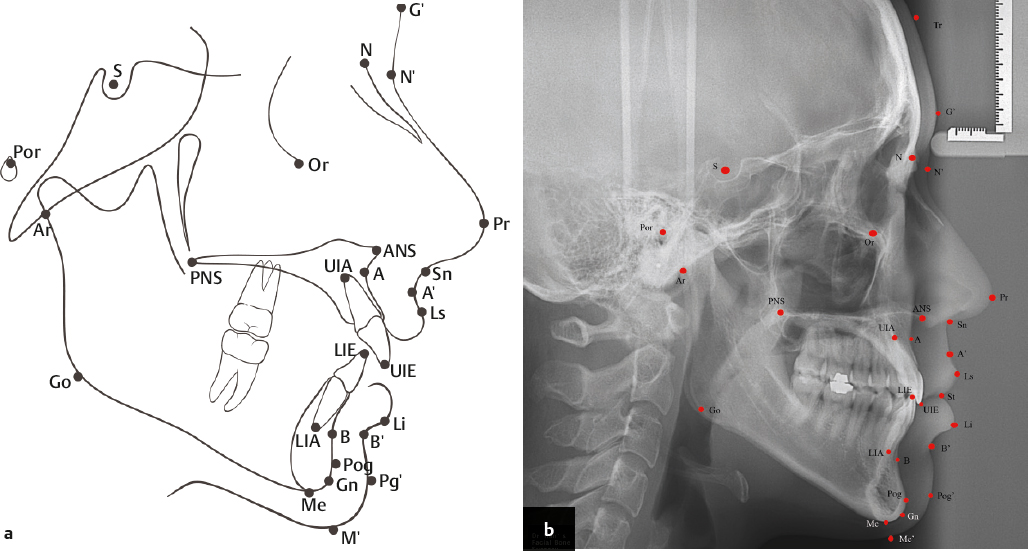
Cephalometric analysis is crucial for identifying the patient’s skeletal and dental problems for corrective surgical planning and postoperative assessment. Standard reference points on a cephalometric X-ray image and basic proportions are shown in Fig. 21.4 and Fig. 21.5 . Cephalometric data analysis reveals that there exists some disparity in certain parametric values between Asians and Caucasians (Fig. 21.6).6,7,8 These differences account for the characteristics features in facial morphology observed in these ethnic groups. Important observations in Asians include (1) more vertical growth tendency (downward growth); (2) upper and lower incisors that are are more labially inclined, giving the lip a more protrusive appearance; (3) facial profiles that are more convex, especially in the middle third of the face (between points A and B); (4) more acute nasolabial angle; (5) significantly shorter distance between the upper lip and E-line (UL–EL) and lower lip and E-line (LL–EL). No statistically significant difference was observed in reference angles like sella-nasion-A point angle (SNA), sella-nasion-B point angle (SNB), A point-nasion-B point angle (ANB), and mentolabial angle across all the ethnic groups (Fig. 21.6).
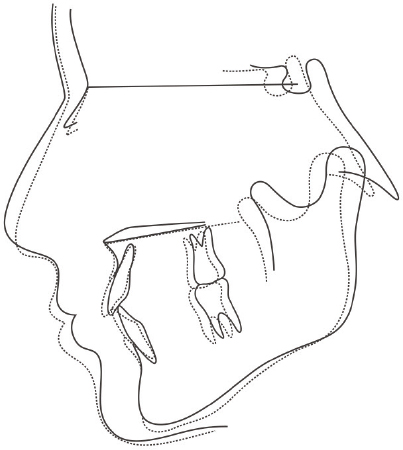
With the advent of new technology such as cone beam computed tomography (CBCT) and 3D processing software, we are currently on the verge of transitioning from the 2D era into 3D. But cephalometric analysis is still useful today and forms the foundation of our understanding of the facial metrics. A dental model is also important in providing information on the arch form (arch width and arch length), teeth position, upper and lower molar relation, and teeth inclination. It also gives a rough simulation of postoperative upper and lower jaw relationships.
Surgical Techniques
In patients with slight malocclusion and no cosmetic concerns, it is reasonable not to offer any treatment. But in cases of skeletal discrepancy of the facial bones, surgery might be the most useful modality of treatment. For Asian patients, the authors prefer Le Fort I osteotomy, high sagittal supraforaminal osteotomy (HSSO), anterior segmental osteotomy (ASO), and genioplasty. Table 21.2 summarizes the appropriate operations for the respective diagnoses.
Typically, the orthognathic surgery is performed under general anesthesia with nasotracheal intubation. Intentional hypotension and perioperative antibiotic coverage in most cases is mandatory.
Surgery of the Mandible
Sagittal Split Ramus Osteotomy (SSRO)
Among the various techniques of mandibular osteotomy proposed so far, sagittal split ramus osteotomy (SSRO), after the Obwegeser–Dal Pont method, is the most widely adopted technique. It is generally indicated in horizontal mandibular excess or deficiency, or cases of mandibular asymmetry.9
First, mark the midline that runs from the glabella along the nasal dorsum, down the philtrum and the midline of the upper lip and upper incisors, through the midline of the lower incisors to the midline of the symphysis. This line is helpful as a reference during and after surgery.
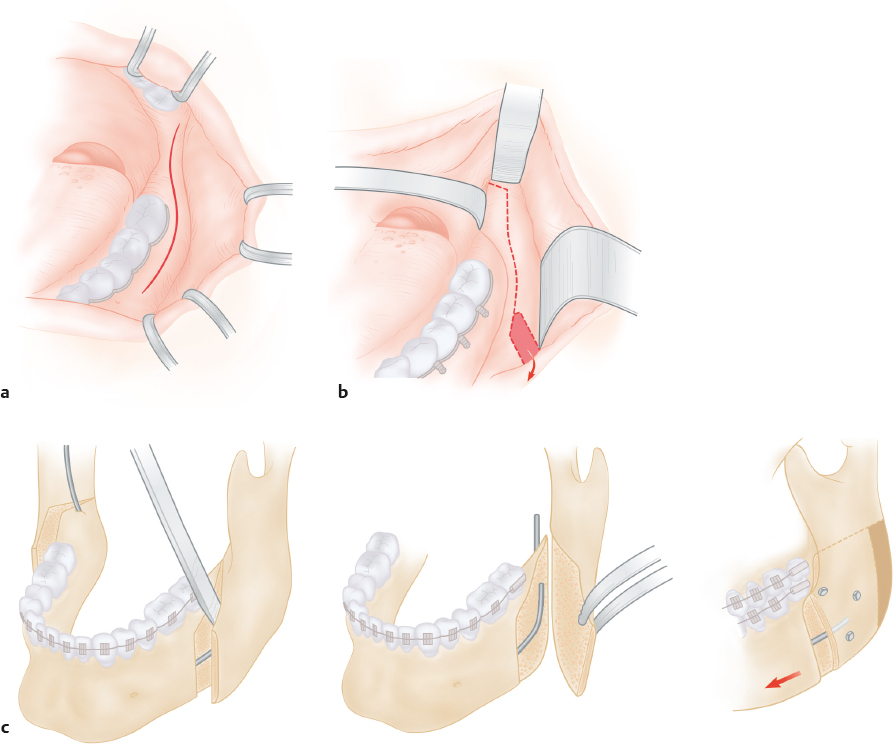
Mucosal incision starts from the buccal vestibule of the lower first molar and continues along the anterior margin of the ascending ramus laterally (Fig. 21.7a). Meticulous soft tissue dissection to the periosteum with proper hemostasis will guarantee safe bone surgery. The buccal fat pad located at the upper part of the ascending ramus should be kept unless it will constantly spill into the surgical field for the rest of the surgery.
The periosteum is incised with diathermy and elevated off the ascending ramus, retromolar area, and first molar region laterally and buccally. Elevation of the periosteum is also done medially between the sigmoid notch and lingula around the mandibular foramen. Periosteal elevation should extend up to the posterior margin to allow instruments to be inserted and to protect the soft tissue at the posterior margin during osteotomy. Prior to elevation of the lingual periosteum of the ascending ramus, infiltration of epinephrine and lidocaine is helpful to avoid accidental rupture of nutrient vessels emerging from the bony foramen. After soft tissue protection is ensured, bone cutting begins with a 3.1- or 4-mm round bur at the anterior border of the ascending ramus. The cortex at the anterior border is removed carefully up to the first marrow bleeding point. At this point, infiltration of epinephrine/lidocaine is performed again before continuing the next step.
Lingual cortex osteotomy is done with a 2.7-mm round bur. Soft tissue protection is ensured with a narrow channel retractor or broad curved periosteal elevator. Special care should be taken not to injure the inferior alveolar nerve and vessels. The authors usually keep the dissection area narrow to avoid damage to the vessel and nerve at the mandibular foramen. The lingual cortex osteotomy is carried to the posterior border of the ascending ramus.
Buccal cortex osteotomy should be designed depending on whether the objective is to achieve setback, advancement, or transverse rotation of the mandible. This can range from a vertical osteotomy near the first molar area to an oblique line running from the second molar to the mandibular angle. Once again, adequate protection is necessary to avoid injury to the facial artery and the marginal mandibular branch of the facial nerve.
After the cortex of the anterior ramus border has been removed as described earlier, the authors create several guide holes in the medulla (Fig. 21.7b) down to the posterior border with a 1.8-mm round bur. Care is taken to avoid the inferior alveolar nerve and vessels by staying close to the buccal cortex, especially at the mandibular body and angle area. Ramus splitting is completed by joining these guide channels with a 2-mm chisel (Fig. 21.7c). The separation should be performed gently and precisely, taking care not to cause unwanted fracture of any segment.
The tooth-bearing segment is referred to as the distal segment while the segment bearing the condylar head is the proximal segment. Once the proximal and distal segments are separated, the mandibular body can move freely. With the prefabricated occlusal splint wired to the upper teeth, the free-moving mandibular distal segment can be easily adapted to the upper teeth and splint. Intermaxillary fixation (IMF) is then performed with the maxillary and mandibular teeth occluded in this new position. The authors generally prefer elastic rubber bands over wires for this purpose.
The new mandible position is checked with the midline drawn preoperatively to ensure facial symmetry. The condylar head is checked to make sure it is in a good and stable position in the glenoid fossa. Once everything is confirmed to be in position, osteosynthesis is performed. There are two methods of osteosynthesis according to the level of fixation. The first, rigid fixation with utilization of titanium plates and screws or lag screws, results in absolute stabilization of the two bone segments. There is no movable gap and primary bone healing occurs with minimal callus formation. The second, nonrigid fixation with wires, permits intersegmental mobility. The wire’s main action is to limit distraction of the two segments while secondary bone healing takes place. Despite being nonrigid, this form of fixation is accepted as being functionally stable. The authors’ preference is the rigid fixation technique because it is less painful and shortens healing time. In addition, rigid fixation can shorten the IMF time. Once osteosynthesis is done, the IMF is released to check for normal occlusion as planned. The wound is then irrigated with normal saline, and a final check for hemostasis is done before closure with 4–0 silk. A 4- to 5-cm silastic drain is anchored on each side.
Related posts:





Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


