Abstract
Careful physical examination combined with a targeted history is the essential first step in the practice of hand surgery. This chapter describes key elements of history in the hand surgery patient and then proceeds through each component of the hand examination: inspection, vascular assessment, sensation, palpation, range of motion, ligament stability, and musculotendinous function. The core maneuvers of the hand examination are defined and illustrated with photographs and videos. A sample documentation is also provided for a normal hand examination.
2 History and Examination of the Hand
I. History
History of the present illness
First line should include hand dominance and occupation:
Sheds light on acute injuries and stress injuries.
Helps determine time available for recovery from disease/injury or surgery if needed and guides the priority of reconstructive procedures.
Injury history
Mechanism: What (the instrument) and how (slice, crush, tear, etc.).
Posture of hand at time of injury.
Where: Can help determine degree of contamination (factory, toolshed, farm, combat).
When: Helps determine potential ischemia time, likelihood of infection, and options for treatment.
Prior treatment: Tetanus, wound cleansing, antibiotics, tourniquet, and treatment of amputated part(s).
Symptoms
“Where does it hurt?”
Cold part, loss of sensation, paresthesias, weakness, loss of coordination, dislocation, clicking, snapping, and popping.
Classify by: Location, onset, course, severity/quality, alleviating factors, exacerbating factors, associated symptoms, and prior experience.
Effect on daily life, occupation, and hobbies.
Confirm that described symptoms are limited to single body part or associated with active systemic disease.
Pregnancy or last menstrual period for reproductive-age female.
“When did you last eat or drink something?” (trauma patient).
Last tetanus immunization.
Past medical history, with special attention to the following:
Major medical conditions affecting wound healing, (e.g., diabetes mellitus).
Major cardiac, pulmonary, or renal disease.
Rheumatologic disease.
Immunocompromised: HIV, transplant, leukemia, etc.
Past surgical history, with special attention to the following:
Prior operations in region of injury/disease.
Complications with anesthesia or bleeding.
Medications, with special attention to the following:
Steroids.
Immunosuppressants.
Anticoagulants.
Allergies, with special attention to the following:
Antibiotics.
Latex.
Shellfish may raise concern for iodine allergy.
Family history, with special attention to the following:
Heart disease.
Rheumatologic disease.
Dupuytren’s disease.
Congenital conditions.
Complications with anesthesia or bleeding.
Social history:
Occupation.
Hobbies/sports.
Substance use.
Intravenous drug use.
II. Principles of Complete Examination
Basic principles apply:
Be systematic and thorough.
Remove dressings, clothing, and jewelry including from the contralateral side to ensure complete exposure.
Adequate lighting is essential, especially if infection is suspected and erythema must be delineated.
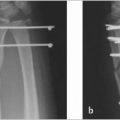
Plain film radiographs in three views (anteroposterior, lateral, and oblique) are useful in most clinical visits and essential in emergency department evaluations.
If anesthesia is required for a complete examination, assess sensation first and motor if possible.
All findings should be compared to the contralateral side.
An experienced examiner may pick and choose the necessary maneuvers, but care should be taken by trainees when skipping portions of the examination to ensure no injury or evidence of disease is missed.
At minimum, a complete examination should include the following:
Inspection
Vascular assessment
Sensation
Palpation
Range of motion
Musculotendinous/neuromotor function
III. Inspection
Injury
Is skin closed and intact?
Degree of contamination
Foreign bodies
Are deep structures visible?
Deformities
Angulation
Malrotation of fingers: Tips should point to scaphoid tubercle when flexed at meta-carpophalangeal (MP) and proximal interphalangeal (PIP) joints
Visible masses
Drawings or photographs are useful for communication and surgical planning (obtain patient permission before taking photographs)
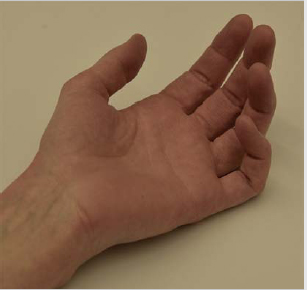
Posture
Resting cascade of fingers (► Fig. 2.1)
Flexion of fingers: Small > ring > middle > index
Motion at rest, e.g., tremors
Swelling
Localized, diffuse within a region, or generalized across body?
Fusiform swelling suggests flexor tenosynovitis
Look for loss of finger creases
Restricted by anatomy?
Palmar inflammation may present as dorsal swelling due to the tightness of the palmar fascia
Apparent delineation along borders of forearm compartments suggesting a possible compartment syndrome
Skin
Scars from prior injury or surgery
Skin color and distribution of color
Erythema suggests infection, inflammation/arthritis flare, or gout.
Delineate borders of erythema with pen or skin marker and note the time.
Streaking may be seen with infection.
Pale color suggests arterial insufficiency.
Purple/dark red color suggests venous insufficiency or contusion.
Lesions
Small can be meaningful; (e.g., paint gun injury may produce tiny puncture wound but causes tremendous inflammation and destruction in the hand).
Ulcers.
Soft tissue infarcts.
Neoplasms.
Calcinosis.
Perspiration: If present, are there areas that are dry?
Nails
Clubbing: Associated with systemic disease but may also be benign.
Paronychia: Infection of the nailfold.
Koilonychia: Spoon-shaped nails, associated with iron deficiency.
Wasting
Unilateral vs. bilateral: Suggests local or systemic pathology, respectively.
Which muscles?
Thenar suggests median nerve pathology.
Interosseous or hypothenar suggests ulnar nerve pathology.
Measure girth
Observing pediatric patients
Young children who have difficulty cooperating with the examination may be encouraged to play with age-appropriate toys and watched closely.
Alternatively, bouncing a ball back and forth between examiner and child provides abundant information on range of motion, dexterity, and reaction time.
First, ask child to catch with right hand. Bounce to different heights and distances from body. Next, ask child to switch to left hand.
Data gleaned from careful observation can target the necessary provocative tests to confirm or rule out diagnoses.
IV. Vascular Assessment
Vascular system is assessed first in an emergency department evaluation to quickly determine if there is ischemia and a more urgent evaluation and treatment are warranted.
Brief assessment
Skin color (see above): Are digits pink and warm or pale or blue or dusky?
Palpate skin temperature, comparing to other digits and contralateral hand.
Palpate radial and ulnar artery pulses (if not palpable, check Doppler).
Capillary refill should be<2seconds beneath the fingernails.
If ischemia is suspected
Pencil Doppler can be placed on the pad ofeach fingertip to listen for distal pulses.
Pulse oximeter can be applied to a digit.
Fingertip can be pricked with 25-gauge needle. Normal finger will show bright red capillary bleeding.
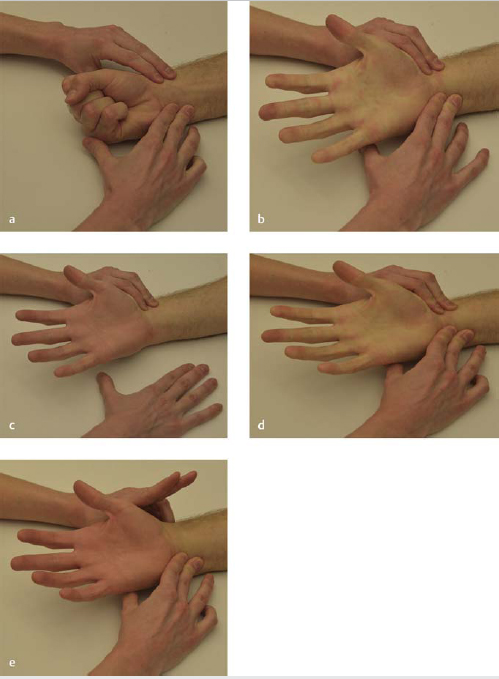
Allen test (► Fig. 2.2, Video 2.1 ):
Assesses for patency of palmar arterial arch.
At least one palmar arch is intact in 97% of patients, enabling the entire hand to be perfused by either the radial or the ulnar artery. 1
Deep arch is usually radial.
Superficial arch is usually ulnar.
Firmly compress radial and ulnar arteries at wrist. Patient makes repeated tight fists to exsanguinate hand and then relaxes fingers. Release pressure on radial artery and watch for blood to return (refill time). Repeat with release of ulnar artery.
Normal = <3 seconds with whole hand being perfused.
Digital Allen’stest
Assesses for collateral flow between ulnar and radial digital arteries.
Compress ulnar and radial side of patient’s fingertip and move proximally to exsanguinate finger. Release the radial side and look for return of blood to entire finger (refill time). Repeat with ulnar side.
Normal = <3 seconds.
V. Sensation
A. First Principles
Sensory examination should be completed before anesthesia (if needed to complete examination).
Based on knowledge of cutaneous innervation by peripheral nerve distributions and dermatomes.
At minimum, light touch and sharp sense should be documented at the radial and ulnar tip of each digit.
Light touch: Cotton swab or examiner’s finger.
Sharp sense: Broken tip of a wooden cotton swab.
Warn patient it should feel sharp but will not hurt.
Apply enough pressure to depress the skin slightly but not enough to puncture or draw blood. Be cognizant of elderly patients with thin, fragile skin.
Stabilize hand holding the cotton swab against the patient’s hand to avoid inadvertently pressing too hard.
Ideally, light and sharp sense should be assessed in proximal and distal areas supplied by each major nerve and compared to the contralateral side.
Carefully delineate and document any areas of numbness or diminished sensation.
Evaluate the effect of hand and extremity position on symptoms.
B. Advanced Sensory Testing
Two-point discrimination: Static or moving/dynamic
Normal static = 6 mm; based on Merkel cells.
Normal dynamic = 3 mm; based on Meissner corpuscles.
Semmes-Weinstein monofilaments: Pressure perception thresholds
Record the number of the thinnest filament for which the patient can sense the pressure required to bend the filament.
Patient should not feel the touch of the unbent filament on the skin.
Vibration: 30 Hz and 250 Hz tuning forks
Recorded as a threshold.
Temperature: Test tubes containing ice water and water at 40 to 45 °C.
Rarely clinically useful, but may be helpful in documenting return of protective sensation following nerve injury.
C. Cervical Examination
Important to evaluate for cervical root compression or spinal pathology as causes of upper extremity neurologic symptoms.
Presence of cervical pathology does not exclude peripheral nerve compression or injury; e.g., it is possible to have root compression and carpal tunnel syndrome simultaneously (“double crush”).
Axial load test
Assesses nerve root compression.
With head in neutral position, press down on the top of the head with moderate pressure.
Positive = reproduction of radicular symptoms in the upper extremities.
Spurling’s test(► Fig. 2.3, Video 2.1 )
Also known as foraminal compression test, it assesses for stenosis of the vertebral foramina through which cervical nerves pass.
Gently rotate neck approximately 20 degrees to affected side and laterally bend neck toward affected side by about 20 degrees. Then apply gentle axial compression.
Positive = reproduction of radicular symptoms in the upper extremities.

D. Provocative Tests
Tinel’s sign: Paresthesia or pain in the distribution of the nerve being tested when the area overlying the nerve is tapped firmly.
It may be applied to median nerve compression in the carpal tunnel or ulnar nerve compression in the cubital tunnel or Guyon’s canal.
After nerve injury, the most distant point of paresthesia represents the furthest extent of nerve regeneration; Tinel’s sign can be followed as a marker of nerve recovery/regeneration.
Median nerve pathology
Direct compression test (Durkan’s test, ► Fig. 2.4).
Direct compression over the carpal tunnel by the examiner’s thumb for 30 seconds.
Positive = pain or paresthesia in the median nerve distribution.
Phalen’s test(► Fig. 2.5)
Hold wrists in maximum palmar flexion for up to 2 minutes.
Positive = pain or paresthesia in the median nerve distribution.
Ulnar nerve pathology
Elbow flexion test
Assesses for cubital tunnel syndrome.
Supinate forearms and hold elbows in maximum flexion for 60 seconds.
Positive = pain or paresthesia in the ulnar nerve distribution.
Duchenne’ssign
Also known as ulnar clawing or intrinsic-minus.
Ring and small fingers have hyperextended MP and flexed PIP and distal inter-phalangeal (DIP).
Indicates loss of intrinsic function with preservation of flexor digitorum profundus (FDP) from a distal ulnar nerve injury.
Froment’s test
Assesses thumb adduction (ADP).
Patient holds a piece of paper or folder between tip of thumb and radial base of the index finger in a lateral/key pinch. Examiner gradually pulls the paper away, encouraging the patient to keep hold of it.
Positive = flexion of thumb interphalangeal (IP) joint.
Usually combined with Jeanne’s sign.
May also see hyperextension of index finger DIP and flexion of index finger PIP.
Jeanne’s sign
ADP.
Present = patient hyperextends MP joint during lateral/key pinch to “lock” the joint, compensating weak or paralyzed ADP.
Wartenberg’s sign
Assesses palmar interosseous muscles.
With hands flat on table, patient is asked to adduct all fingers.
Present = inability to adduct small finger.
Indicates weak/paralyzed third palmar interosseous resulting in unopposed extensor digiti minimi (EDM).
Pitres-Testut sign
Assesses second and third dorsal interosseous muscles.
With palm flat on table, hyperextend middle finger and deviate it radially and ulnarly.
Present = inability to make this motion.


Related posts:
 8 Fractures and Dislocations of the Distal Radius and Ulna
8 Fractures and Dislocations of the Distal Radius and Ulna
 3 Radiographic Anatomy
3 Radiographic Anatomy
 12 Tendinitis, Tendinosis, and Dupuytren’s Contracture
12 Tendinitis, Tendinosis, and Dupuytren’s Contracture
 15 Extensor Tendon Injury, Repair, and Reconstruction
15 Extensor Tendon Injury, Repair, and Reconstruction
 Private: 20 Vascular Pathology of the Hand and Upper Extremities, including Kienbock’s Disease
Private: 20 Vascular Pathology of the Hand and Upper Extremities, including Kienbock’s Disease
 Private: 25 Fractures of the Pediatric Hand
Private: 25 Fractures of the Pediatric Hand
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


