Abstract
This chapter discusses in detail the twenty-seven bones, the ligaments, and the tendons that comprise the hand and wrist. Of special importance is the discussion listing the diagnostic requisites for a proper evaluation of wrist injuries, including fractures. In addition to bones, ligaments, and tendons, all other elements of hand and wrist anatomy—blood supply, the fingertip, nerves, skin—are discussed, thus providing a thorough treatment of every component in the anatomical structure.
2 Hand and Upper Extremity Anatomy
2.1 Goals and Objectives
Name the bones in the hand and wrist and identify them on a plain film.
Describe the extensor and flexor zones of the hand.
Describe the blood supply and innervation to the hand.
Be able to diagnose a structural injury based on known anatomy.
2.2 Pertinent Information
2.2.1 Bones and Ligaments of the Forearm, Wrist, and Hand
The hand and wrist has a total of 27 bones. The wrist is made of the distal ends of the radius and ulna, the eight carpal bones, and the proximal ends of the five metacarpals. The carpal bones consist of two rows of four bones each. The proximal row includes radial to ulnar, the scaphoid, lunate, triquetrum, and pisiform (Fig. 2‑1). The distal row includes radial to ulnar, trapezium, trapezoid, capitate, and hamate. The proximal carpal row is considered intercalated because no tendons insert on them and their motion depends on their surrounding articulations. The distal row is connected to each other by short intercarpal ligaments, resulting in negligible motion between them. The extrinsic carpal ligaments connect the distal radius and ulna to the carpal bones. The intrinsic ligaments have their origins and insertions within the carpal bones. When a surgeon wants to enter the wrist joint, he makes a dorsal “ligament sparing” incision, which looks like a radially based “V.” This incision splits the dorsal radiotriquetral (radiocarpal) ligament and the dorsal intercarpal ligament. These ligaments are felt to play an important role in stabilizing the proximal carpal row. Palpable landmarks are the sulcus between the scaphoid and trapezoid, the dorsal tubercle of the triquetrum, and the midpoint between Lister’s tubercle and the dorsal rim of the sigmoid notch (Fig. 2‑2). 1


The two most important intrinsic ligaments are the scapholunate and lunotriquetral ligaments. The scapholunate ligament is made of a thin volar, a proximal, and a dorsal portion. The dorsal ligament is the thickest, strongest, and most critical scapholunate stabilizer. The radioscaphocapitate and scaphotrapezial ligaments are secondary stabilizers of the scapholunate articulation. The “dart throwing motion” is felt to be the most frequently used wrist motion in activities of daily living. The biomechanics is the radiodorsal/ulnopalmar motion of the midcarpal joint and concerns the scaphocapitate and scaphoid-trapezium-trapezoid (STT) ligament. 2
When evaluating for bone or ligament injuries to the wrist, four X-ray views of the wrist are needed: posteroanterior (PA), lateral, scaphoid (PA in ulnar deviation), and 45 degree semipronated oblique. A PA view of the wrist should show three smooth radiographic arcs, known as Gilula’s lines (Fig. 2‑3). Bone articulations normally have apposing parallel surfaces separated by 2 mm or less. A step off or discontinuity of Gilula’s lines, carpal overlap, or unusually wide distances between bones suggests an injury. A normal lateral view shows the radius, lunate, capitate, and third metacarpal lined up vertically. Angles frequently used to evaluate carpal stability are the capitolunate, scapholunate, and radiolunate angles, based on the lateral view (Fig. 2‑4). The capitolunate angle is measured by drawing a line perpendicular through a line connecting the palmar and dorsal tips of the lunate. This is compared to the capitate axis. The normal capitolunate (CL) axis is 0 ± 15 degrees. The scaphoid is represented by a line that connects the two proximal and distal convexities of the palmar aspect of the bone. The normal scapholunate (SL) angle is 47 degrees (range: 30–60). The axis of the radius is found by drawing a perpendicular through its distal third. The RL should be 0 ± 15 degrees. A dorsal tilt of the lunate “spilled teacup” suggests dorsal intercalated segment instability (DISI), found in scapholunate ligament injuries. The scaphoid shift (“Watson”) test is performed by placing pressure over the volar scaphoid while the wrist is moved from the ulnar to radial direction. The unrestrained scaphoid will temporarily shift out of the scaphoid fossa on the radius. A disruption of the scaphoid from the lunate may cause the scaphoid to tilt volarly and the lunate to turn dorsally. This does not always happen, if the secondary stabilizers remain intact. A volar tilt suggests volar intercalated segment instability (VISI), found in lunotriquetral injuries. A disruption of the triquetrum from the scaphoid will cause the triquetrum to turn dorsally and the lunate, still attached to the scaphoid, to turn volarly. 3


When the scapholunate ligament has been disrupted and the proximal pole of the scaphoid subluxes dorsoradially, the forces across the radiocarpal joint are abnormally distributed, leading to degenerative changes over time. The progression of changes involves first the articulation between the radial styloid and scaphoid, followed by the entire radioscaphoid, then the capitolunate joint. This pattern is known as scapholunate advanced collapse wrist. The radiolunate joint is seldom affected because it remains in contact with normal cartilage due to the restraining effect of the short radiolunate ligament. 3
2.3 Wrist and Hand Fractures
The scaphoid (navicular) bone is the most commonly fractured carpal bone. The scaphoid has five articulating surfaces and is nearly entirely covered by cartilage. It is the link between the proximal and distal carpal rows and has multiple ligamentous attachments from where it receives its blood supply. The blood supply enters distally. The proximal pole is dependent on an interosseous blood supply, which makes it vulnerable to avascular necrosis, particularly when fractures involve the proximal third. 3 In the authors’ opinion, these are best referred to an experienced wrist surgeon due to the progressive arthritis and dysfunction that can result from nonunions, known as scaphoid nonunion advanced collapse (SNAC).
Fractures of the carpal bones other than the scaphoid are rare and make up 1.1% of all fractures. The more common of those fractures will be discussed. When initial X-rays are negative, but suspicion is high, a computed tomographic (CT) scan is appropriate. Triquetral fractures are the second most common carpal fracture and come in three varieties: dorsal cortical, triquetral body, and volar avulsion. The most common is the dorsal cortical, which is treated with splinting for 3 to 4 weeks. 4
The trapezium is the next most commonly fractured carpal. The vertical intra-articular fracture is the most common pattern and frequently accompanies the Bennett fracture. Nondisplaced fractures are treated in a thumb spica splint; younger, active patients are best treated with reduction by an open or closed approach to minimize future carpometacarpal (CMC) or STT arthritis. 4
Hamate fractures may involve the hook or the body. Hook fractures are classically described in golfers, baseball players, and racket sport athletes. This may present with ulnar nerve symptoms. A carpal tunnel view on plain films or CT can secure the diagnosis. The blood supply to the distal hook is poor with a healing rate of 50%. Excision is a reasonable treatment option with no adverse effects to grip or motion. Nondisplaced body fractures can be splinted. A direct blow, repetitive trauma, or sudden contraction of the flexor carpi ulnaris (FCU) can cause a pisiform fracture. Splinting can be successful in nondisplaced fractures. Displaced fractures or nonunions can be treated with excision, with no resulting loss of mobility. 4
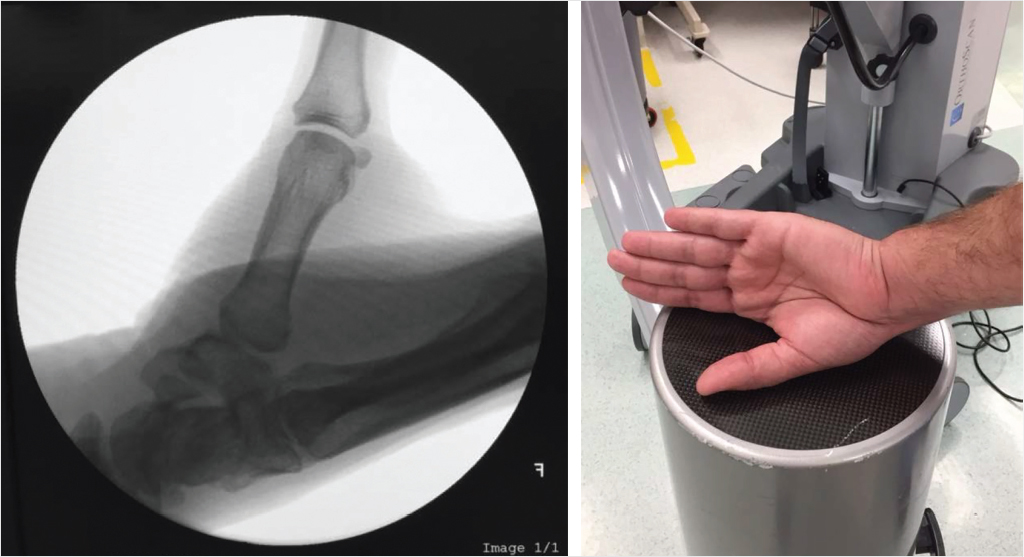
The first CMC joint is unique to humans, allowing opposition and prehension, but hastening the development of arthritic changes. The CMC joint is a biconcave–convex saddle joint, with five articular surfaces and minimal bony constraint. Sixteen ligaments have been described that stabilize the trapezium. Compressive forces magnify greater than 13 times from the fingertip to the trapeziometacarpal joint. Osteoarthritic lesions are first found palmarly on the joint. Degeneration of the posterior oblique ligament has been linked to the development of arthritis when incompetence of the ligament allows abnormal dorsal translation of the metacarpal on the trapezium. 3 The CMC is best viewed by the Roberts technique (thumb AP), where the forearm is maximally pronated and the dorsum of the thumb rests on the X-ray cassette (Fig. 2‑5).
The five metacarpal bones each articulate with the carpus. A rigid ligament connection exists between the trapezoid and capitate and the second and third metacarpals that allow for very little mobility. Fracture dislocations are rare and tend to involve significant force (Fig. 2‑6). There is greater mobility at the articular surfaces of the fourth and fifth metacarpals, which allows for greater deformity to be accepted when evaluating a fourth or fifth metacarpal fracture. Metacarpal fractures, particularly central ones, are biologically splinted by the intermetacarpal ligaments and interosseous muscles. 5 Patients must be examined for rotational deformity upon digital flexion. If nonoperative treatment is chosen, repeat films must be performed, particularly of spiral or oblique fractures, to verify alignment is maintained. Fractures of multiple adjacent metacarpals are less stable and a lower threshold for surgical fixation is indicated.

Fractures of the metacarpal neck, also known as “boxer’s” fractures, are among the most common hand fractures. This is really a “brawler’s” fracture since a skilled boxer does not tend to have this fracture pattern. The fifth metacarpal is tolerant of the apex-dorsal deformity and up to 70 degrees of angulation may be compensated for in the fifth metacarpal carpal joint. In comparison, only 10 degrees of angulation is tolerated in the second and third rays. The Jahss reduction maneuver involves flexing the metacarpophalangeal (MCP) joint, proximal interphalangeal (PIP) joint, and distal interphalangeal (DIP) joint and using the proximal phalanx to push the metacarpal head dorsally. 5 This may be difficult to do successfully without sedation. It is the authors’ opinion that patients who tend to present with “boxer’s” fractures are usually poor surgical candidates for the same reason they sustained the injury and are often unreliable with pin care, splinting, and follow-up.
Intra-articular fractures of the first metacarpal are known as Bennett’s and Rolando’s fractures. Bennett’s fractures are avulsions of the ulnar metacarpal base. The abductor pollicis longus tendon pulls the shaft proximally, displacing the fracture. A Rolando fracture is a comminuted intra-articular fracture of the proximal first metacarpal. Surgical reduction and fixation is often required for both these unstable fracture patterns. 5
There are 14 phalangeal bones. Nondisplaced distal phalanx and comminuted tuft fractures are most often treated with splinting until tenderness resolves. Minimally displaced, stable, extra-articular fractures of the middle and proximal phalanx may be treated with buddy taping in a compliant patient. Transverse proximal phalanx fractures are unstable and usually best treated with close reduction and internal fixation with a longitudinal pin. We try to minimize open reduction and plate fixation of the middle and proximal phalanx due to the adhesions that can develop between the plate and tendons.
The PIP joint is central to digit function, having up to 120 degrees of mobility. The PIP joint has been described as the “anatomical and functional locus of finger function.” 3 It is a hinge, or ginglymus, joint that resists lateral and rotary stress. The joint has a “ligament-box” configuration that resists PIP displacement Fig. 2‑7. The collateral ligaments originate on the lateral aspect of each proximal phalanx condyle. The proper ligament inserts on the volar one-third of the base of the middle phalanx and the accessory ligament inserts more volarly on the volar plate. The volar plate forms the floor of the joint. Disruption in at least two planes has to take place for displacement of the middle phalanx to occur. Dislocations can usually be treated with reduction and either dorsal splinting or buddy taping. Fracture dislocations or pilon fractures are beyond the scope of this chapter, but can be treated with a variety of options, from extension block splinting to hemi-hamate arthroplasty, depending on the fracture pattern and surgeon experience. 6
The MCP joint (digits 2–5) forms a condyloid joint. The head is narrow dorsally and wider volary, which creates more contact with the proximal phalanx with greater flexion. The collateral ligaments are more taut in flexion (the “cam effect”), allowing less abduction and adduction, compared with full extension. The MP joints are well protected from injury due to their surrounding support structures (flexor and extensor tendons, volar plate, and intervolar plate ligaments) and location at the base of the fingers. 3 Dislocation of the MP joints is rare, but when they occur, they most frequently are a dorsal dislocation of the index finger due to a forced hyperextension. The volar plate is disrupted proximally, the flexor tendons are found ulnarly, and the lumbricals found radially. The radial digital nerve is superficial and at risk of injury during open reduction. 6
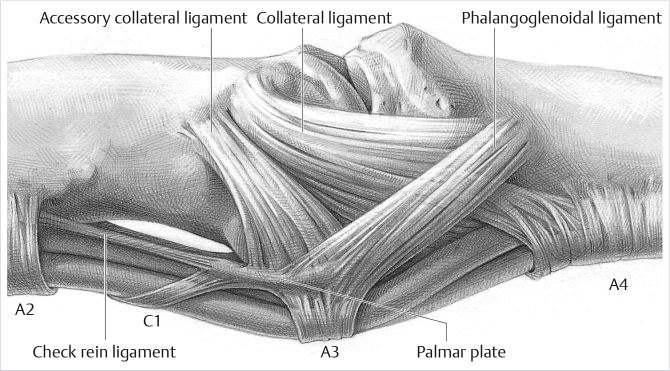
The mobility of the thumb MCP joint is the most variable of any joint in the body due to the curvature of the metacarpal heads. The joint is supported laterally by the proper collateral ligaments that originate from the lateral condyles of the proximal phalanx and insert on the volar third of the proximal phalanx. The accessory collateral ligaments originate from a more volar position on the metacarpal head and insert on the volar plate and sesamoids. The floor of the joint is formed by the volar plate. The proper collaterals are tight in flexion and loose in extension; the accessory collaterals are tight in extension and loose in flexion. Injuries to the ulnar collateral ligament (UCL) are 10 times more common than to the radial collateral ligaments and are a well-known skiing-related injury. The adductor aponeurosis can become interposed between a distally avulsed UCL and its insertion (Stener’s lesion), making adequate ligament healing impossible without surgical intervention. 3
2.3.1 Blood Supply
The hand is supplied by the ulnar artery and the radial artery that originate in the proximal forearm. The ulnar artery continues as the superficial palmar arch and the radial artery continues as the deep palmar arch. An interosseous median artery is a major contributing vessel in 5% of people. An arch is called “complete” when it connects with a branch from another independent artery. The superficial palmar arch is complete in 78.5% of patients; the deep palmar arch is complete in 97% of patients. 7 There are three common digital arteries found at the second, third, and fourth web spaces at the level of the MCP joints. The common digital vessels branch into radial digital and ulnar digital vessels. Up to 98.5 % of extremities have all five digits receiving arterial inflow at the level of the proper digital or common digital artery from both the deep and superficial arches. 3 The ulnar digital artery to the small finger and the radial digital artery to the thumb and index finger tend to be of smaller caliber than the parallel digital artery. This is relevant in a trauma setting when it is more time efficient to concentrate efforts on the larger vessel.
There are consistently four vessels that supply the thumb: the palmar ulnar, palmar radial, dorsal ulnar, and dorsal radial arteries. The palmar blood supply to the thumb arises from the first of four palmar metacarpal arteries, designated as the “princeps pollicis” artery. The princeps pollicis may arise from the first dorsal metacarpal artery, the deep arch, the first palmar metacarpal artery, or the terminal branch of the superficial palmar arch. Several anastomotic connections have been found between the radial and ulnar digital arteries and between the dorsal and palmar systems on cadaveric dissections, which allow for thumb survival after severe vascular injury and provide multiple alternatives in flap designs. 8 Identification of the ulnar artery as the larger artery and originator of the superficial palmar arch led to the conclusion that the ulnar artery is the dominant artery. Subsequent studies found that the radial artery is more important to digital blood flow, with 20% of hands losing pulsatile blood flow to the digits with radial artery compression at the wrist, compared with 5% of hands with ulnar artery compression. 9
The Allen test was originally described in 1929. The patient closes the hand tightly for 1 minute or until blanching of all digits occurs while the examiner occludes both arteries. The patient extends the fingers and one artery is released. The return of color to the hand indicates an intact circulation from that artery. There have been reports of preoperative Allen’s test being poor predictors of postoperative perfusion after radial artery harvest or cannulation. 10 It is the authors’ practice to occlude the radial artery with an Acland clamp and listen for perfusion through the common digital vessels prior to proceeding with a radial forearm free or pedicle flap.
Isolated injuries to the radial or ulnar artery do not usually produce critical ischemia or impaired function. Flow will increase through the intact parallel vessel over time. Reconstruction should be considered for improving nerve recovery, diminishing cold intolerance (particularly in colder climates), anticipating future injuries, or to facilitate healing. 3 If ischemia has been ruled out, reconstruction can be performed in a nonemergent setting.
Related posts:




Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


