19 Surgical Approaches to the Orbit
Abstract
“Surgical Approaches to the Orbit” describes the surgical approaches used in the management of orbital lesions other than those due to thyroid eye disease or orbital wall blowout fractures. Selection of the surgical approach depends on the anatomical location, size, and extent of the lesion; the suspected pathology; and the goal of the surgery. The applied anatomy is largely concerned most with the surgical spaces into which the orbit is divided: extraconal, intraconal, subperiosteal, and sub-Tenon’s. The principles of orbital surgery include thorough knowledge of eyelid and orbital anatomy, orbital disorders, and imaging techniques; familiarity with the surgical approaches, instruments, and equipment; proper illumination and magnification of the surgical field; adequate surgical exposure and meticulous dissection, careful removal and presentation of biopsy specimens; good hemostasis; and good postoperative care. Orbitotomy approaches include anterior, medial, lateral, endoscopic, combined, and transcranial. Optic nerve sheath fenestration for the management of visual loss resulting from papilledema in the setting of idiopathic intracranial hypertension is also described.
19.1 Introduction
This chapter describes the surgical approaches used in the management of orbital lesions. The surgical approaches used to achieve a decompression of the orbit in the management of thyroid eye disease are described in Chapter 20. The surgical approaches used to manage orbital wall blowout fractures are described in Chapter 26.
It is important to ensure that the patient has been properly prepared for surgery before proceeding with an orbitotomy, particularly with regard to the management of hypertension and the use of antiplatelet and anticoagulant agents. If significant blood loss is anticipated from the surgery, the patient’s blood should be grouped and saved and donor blood cross-matched and made available if necessary. A full blood count and platelet count should be undertaken before surgery along with a biochemical profile.
Informed consent should be obtained, ensuring that the patient understands the small risk of visual loss from intraoperative trauma to the optic nerve or from postoperative intraorbital hemorrhage. Additional risks specific to the surgical approach should also be discussed, including infection, bleeding, ptosis, diplopia, sensory loss, pupillary enlargement, cosmetic deformity, hypertrophic scarring, cerebrospinal fluid (CSF) leak, meningitis, and intracranial trauma. The correct side should be clearly marked by the surgeon after checking with the patient, checking the consent form, and checking the orbital scans.
The anesthetist should understand the surgical approach and the requirements for the following:
Head positioning.
Nasal packing.
The use of vasoconstrictive agents.
The preoperative intravenous injection of acetazolamide if indicated.
The intraoperative intravenous injection of steroid (dexamethasone).
Intravenous antibiotics.
Induced intraoperative hypotension.
The potential risk of the oculocardiac reflex.
The potential risk of bleeding.
The anticipated length of the surgical procedure.
The requirements for postoperative analgesia.
Simple anterior orbitotomies can be performed under local anesthesia, usually with intravenous sedation, but the more complex orbitotomies are performed under general anesthesia.
Patients should be kept in hospital overnight for observation and regular checks on visual function after any orbitotomy.
It is essential that the patient’s computed tomography (CT) and magnetic resonance imaging (MRI) scans are available in the operating room. These should be clearly visible on a screen adjacent to the operating table. They should be reviewed before the orbitotomy is commenced and the correct side reconfirmed with the surgical team. The scans may need to be reviewed to confirm the location of the orbital lesion as the surgery proceeds.
The surgical plan should be coordinated with the nursing team in advance to ensure that the appropriate surgical instrumentation is available. A potential change in the surgical approach, depending on the intraoperative findings, should be anticipated and the necessary instrumentation made available. It is also important to liaise with the pathologist before surgery, particularly if urgent reporting of a biopsy is required. The pathologist must be provided with adequate clinical details.
If a multidisciplinary team is involved in the surgical management of the patient, it is important to define the responsibilities of each member in advance. This also relates to the postoperative care of the patient.
Key Points
Key points in the surgical management of a patient with orbital disease:
Patient preparation: control of hypertension, discontinuation of antiplatelet drugs, informed consent, correct surgical site checking and marking.
Communication with the anesthetist.
Communication with the operating department nursing staff.
Communication with the pathologist.
Ensuring all orbital scans for the patient are available in the operating room.
19.2 Selection of the Surgical Approach
The choice of surgical approach to an orbital lesion will depend on:
The anatomical location of the lesion.
The size and extent of the lesion.
The suspected pathology.
The goal of the surgery.
19.2.1 The Anatomical Location of the Lesion
Orbital tumors that lie anterior to the equator of the globe are most commonly approached via an anterior orbitotomy. Tumors located posterior to the equator of the globe require a more complex deep surgical approach, which is also influenced by the relationship of the lesions to the optic nerve.
Key Point
A surgical approach to an orbital lesion that avoids crossing the optic nerve should be selected.
19.2.2 The Size and Extent of the Lesion
Most orbital lesions can be managed adequately via a single orbitotomy approach. Some orbital lesions require a combination of orbitotomy approaches; for example a medial transconjunctival orbitotomy can be combined with a lateral orbitotomy, which enables the globe to be retracted laterally. This can greatly improve safe surgical access to large or deep medial orbital lesions.
19.2.3 The Suspected Pathology
The surgical approach is influenced by the suspected pathology of the orbital lesion. For example, an incisional biopsy of a suspected lacrimal gland carcinoma should be performed via a transseptal anterior orbitotomy. In contrast, a suspected pleomorphic adenoma of the lacrimal gland should not be subjected to an incisional biopsy if at all possible but should be removed as an extirpative excisional biopsy via a lateral orbitotomy.
19.2.4 The Goal of the Surgery
In the management of orbital tumors the goals of the surgery are usually to achieve, as safely as possible, an incisional biopsy, an excisional biopsy, and a debulking or decompression of the tumor. In general, infiltrative processes suggest a malignant lesion and require an incisional biopsy to establish a histopathological diagnosis. Well-circumscribed lesions generally suggest a benign lesion that can be removed as an excisional biopsy, such as a cavernous hemangioma. Such surgery not only establishes a histopathological diagnosis but also serves as a curative treatment. Some benign orbital lesions may not be amenable to surgical excision, but a debulking procedure may be beneficial (e.g., a plexiform neurofibroma). A small benign orbital apical tumor located medial to the optic nerve, causing compressive optic neuropathy, may be better managed by means of an endoscopic medial orbital wall decompression than by a more invasive procedure to remove the lesion that carries a risk of visual loss.
19.3 Applied Anatomy
See Chapter 2 for a detailed description of orbital anatomy. This should be carefully reviewed before undertaking any orbital surgery.
19.3.1 Surgical Spaces of the Orbit
Anatomically, the orbital spaces are divided into the following areas:
Sub-Tenon’s space.
Intraconal space.
Extraconal space.
Subperiosteal space.
A good understanding of the surgical spaces of the orbit is essential to select the most appropriate surgical approach and to assist in navigation within the orbit during surgery (Fig. 19‑1).
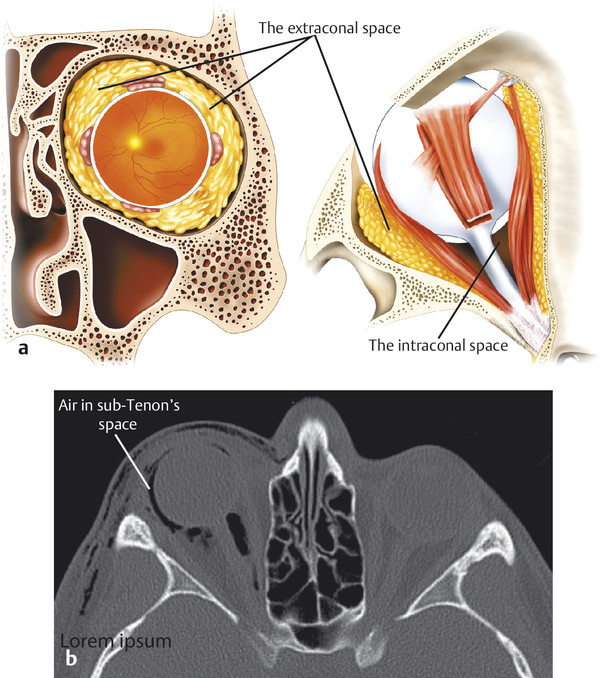
19.3.2 Extraconal Space
The extraconal space contains the following:
The lacrimal gland.
The oblique muscles.
The trochlea.
Orbital fat.
The superior and inferior ophthalmic veins.
Nerves and other vessels.
The lacrimal gland is approached via an upper eyelid skin crease incision for an incisional biopsy for suspected lymphoma, nonspecific orbital inflammatory syndrome, or malignancy. A formal lateral orbitotomy with bone removal is required for the removal of a suspected lacrimal gland pleomorphic adenoma.
The extraconal fat includes the preaponeurotic fat that is important in the identification of the underlying eyelid retractors. Extraconal fat can be removed superiorly via an upper eyelid skin crease incision. Medial, lateral, and inferior extraconal fat can be removed via a transconjunctival incision.
The anterior portion of the superior ophthalmic vein lies in the extraconal space. This can be accessed via an upper eyelid skin crease incision. In patients with arteriovenous fistulas, the vein is dilated and can provide an alternative access for the insertion of platinum coils in conjunction with an interventional radiologist in selected cases.
19.3.3 Intraconal Space
The intraconal space lies within the recti and their intermuscular septa. The intraconal space contains the optic nerve, intraconal fat, nerves, and vessels. Tumors of the optic nerve lie within this space.
The intraconal space may be accessed via a number of surgical approaches; for example, to perform an optic nerve sheath fenestration, the optic nerve may be approached superomedially via an upper eyelid skin crease incision (the preferred approach), medially via a conjunctival incision with disinsertion of the medial rectus muscle, or laterally via a lateral orbitotomy, with or without bone removal. During a lateral orbitotomy approach with bone removal, the intraconal space is usually accessed by dissecting between the lacrimal gland and the lateral rectus muscle.
19.3.4 Subperiosteal Space
The subperiosteal space is a potential space that lies between the periorbita and the bony orbital walls. The periorbita covers all the bones of the internal orbit. Unlike the periosteum covering bones elsewhere, the periorbita is loosely adherent over the orbital walls, except at the orbital suture lines and along the orbital rims, where it is tightly adherent to the bone. The subperiosteal space is a potential space that can be filled with blood (a subperiosteal hematoma) or pus (a subperiosteal abscess). The periorbita is lifted from the walls of the orbit in a characteristic dome-shaped fashion that is limited by the orbital suture lines (Fig. 19‑2).
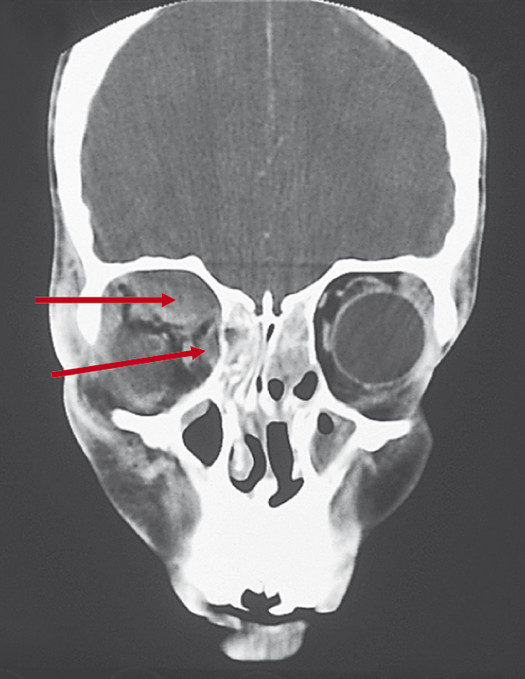
The periorbita is dome-shaped below the roof and along the medial wall of the orbit, assuming a configuration limited by the attachment of the periorbita to the frontoethmoidal suture line.
The subperiosteal space is accessed surgically for the repair of orbital wall blowout fractures, for the drainage of subperiosteal abscesses or hematomas, for bony orbital decompression surgery, or for the insertion of subperiosteal orbital implants in anophthalmic patients. This space can be accessed via a variety of transcutaneous or transconjunctival incisions.
19.3.5 Sub-Tenon’s Space
Sub-Tenon’s space is a potential space situated between the globe and Tenon’s capsule. It is not commonly involved in pathological processes. The space may be enlarged with fluid visible on echography in posterior scleritis, by air (Fig. 19‑1b), or by infiltration by extraocular extension of intraocular tumors (e.g., choroidal melanoma).
19.4 The Principles of Orbital Surgery
The prerequisites for successful atraumatic orbital surgery include the following:
A thorough knowledge of eyelid and orbital anatomy.
A thorough knowledge of orbital disorders.
A thorough understanding of orbital imaging techniques.
Familiarity with the surgical approaches to the orbit.
Familiarity with the required surgical instrumentation.
Appropriate illumination and magnification of the surgical field.
Adequate surgical exposure.
Meticulous surgical dissection.
Careful removal and presentation of biopsy specimens.
Good hemostasis.
Good postoperative care.
19.4.1 Thorough Knowledge of Eyelid and Orbital Anatomy
It is essential to acquire a thorough knowledge of normal eyelid and orbital anatomy before undertaking surgical procedures in an orbit whose anatomy has been altered by a pathological process. It is imperative to observe and assist at a variety of orbitotomy approaches before embarking on such surgery. If possible, the opportunity to examine the orbital contents from above with the brain and orbital roof removed during a postmortem examination should not be missed. This is particularly helpful before performing any surgery on the orbital apex with a neurosurgical colleague.
19.4.2 Thorough Knowledge of Orbital Disorders
The evaluation of a patient with an orbital disorder is discussed in Chapter 18, which discusses both common and important orbital disorders. A differential diagnosis based on a thorough history, a meticulous physical examination, imaging, and laboratory investigations should enable a decision about appropriate management to be made. For the appropriate management of many orbital inflammatory or neoplastic lesions, a biopsy is necessary. As a general rule, an incisional biopsy is necessary for an orbital lesion that is suggestive of malignancy or inflammation, whereas an excisional biopsy is indicated for the removal of a well-circumscribed orbital lesion suggestive of a benign process.
19.4.3 Thorough Understanding of Imaging Techniques
Spending time with an experienced neuroradiologist reviewing a variety of orbital CT and MRI images on a regular basis is an invaluable exercise.
19.4.4 Familiarity with the Surgical Approaches
Familiarity can only be gained by experience. It is essential to observe and assist at a variety of surgical approaches to the orbit before undertaking this surgery.
19.4.5 Familiarity with the Required Surgical Instrumentation and Equipment
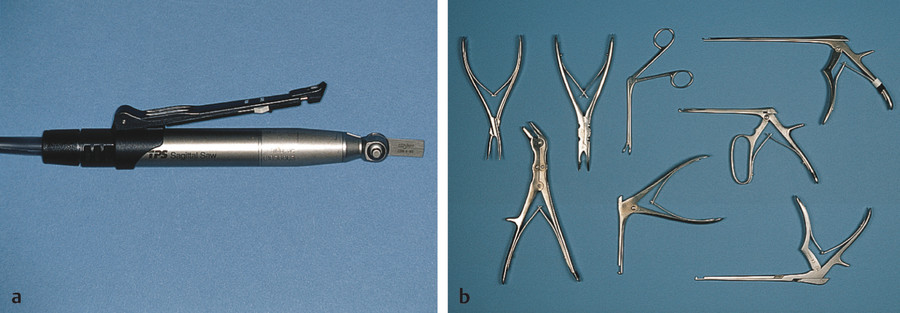
Familiarity with the instruments and equipment is also gained by experience. It is essential to understand the basic assembly of the drills and saws used in orbital surgery and the safety provisions for all members of the team. The drill handpiece should have a safe mode that is activated and deactivated by the surgeon (Fig. 19‑3a). This avoids inadvertent activation of the drill or saw via a footswitch when attempting to use bipolar cautery. All members of the team should wear face guards to protect their eyes and faces from blood and bone fragments. Protection of the patient’s globes from inadvertent injury by the instrumentation is the surgeon’s responsibility, as is adequate intraoperative corneal lubrication using a preservative-free ointment. A variety of burr sizes (both rose head and diamond) should be available. A variety of bone rongeurs are also required (Fig. 19‑3b).
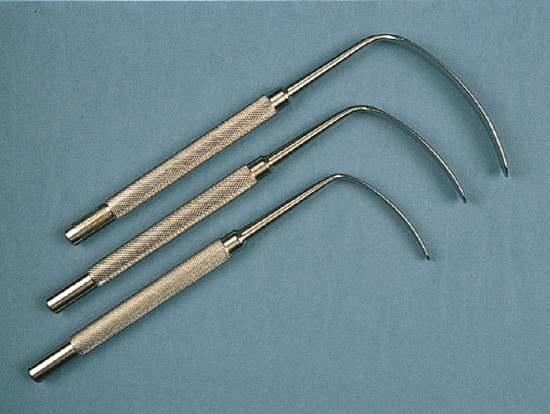
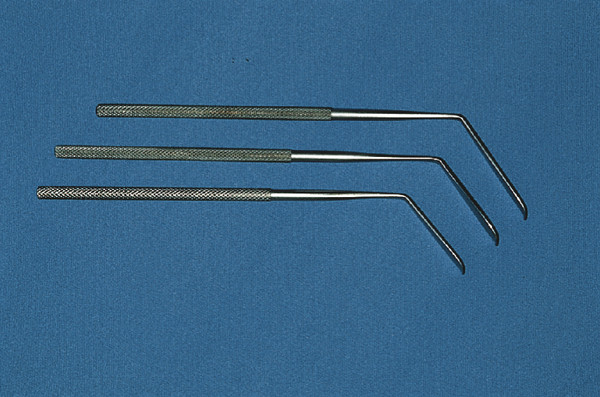
A microplating system and Medpor blocks and sheets are occasionally necessary to reconstruct complex bony orbitotomies, especially where additional bone has been removed to gain improved access to the orbit. A variety of orbital retractors should be available in different sizes (Sewall, Wright’s, and malleable ribbon retractors). The retractors have different purposes and must be used appropriately. Sewall retractors have a sturdy handle that enables the assistant to apply traction by hand (Fig. 19‑4). These are used during subperiosteal dissection in orbital decompression procedures or orbital blowout fracture repairs. These retractors are particularly efficient if used with a sheet of Supramid, which prevents the prolapse of fat around the edges of the retractor. This makes dissection of all margins of a large orbital floor blowout fracture much simpler.
It is essential to appreciate the pressure on the globe that can be generated with these retractors. This is particularly important if the globe’s integrity has been compromised (previous penetrating keratoplasty, penetrating injury repair, peripheral corneal gutter, staphyloma, etc.). Traction on the retractors should be released at regular intervals during surgery and the pupil closely monitored.
Wright’s retractors have more delicate handles and blades that are more appropriate for the retraction of fat around orbital tumors (Fig. 19‑5). These are held with the fingers, in contrast to the Sewall retractors. Malleable ribbon retractors are particularly useful for protecting the globe and surrounding tissues when using the drill and saw.
19.4.6 Proper Illumination and Magnification of the Surgical Field
A comfortable fiberoptic headlight provides excellent illumination of the orbital structures during most orbitotomy procedures. This should be used in conjunction with surgical loupes that provide a comfortable working distance, good magnification, a satisfactory depth of focus, and an adequate field of view. For some orbital dissections it may be necessary to resort to the use of an operating microscope. This allows the surgical assistant and observers (via a video monitor) to see precisely the same deeper orbital structures as the surgeon.
19.4.7 Adequate Surgical Exposure
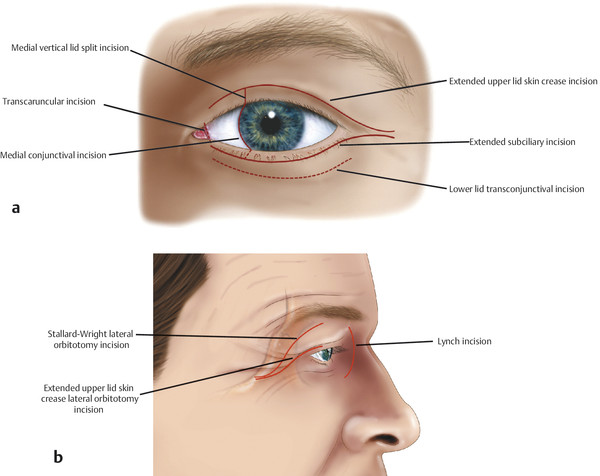
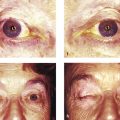
The surgical incision should be of an adequate length. Although incisions are generally selected to achieve the best possible postoperative cosmetic result (Fig. 19‑6), the main consideration is safe and adequate surgical access.
Traction sutures should be carefully placed at strategic positions. These can be supplemented with self-retaining Jaffe retractors.
The patient should be prepped and draped so that the fellow eye can be observed if necessary, ensuring that this eye is adequately protected during the course of the surgery.
19.4.8 Meticulous Surgical Dissection
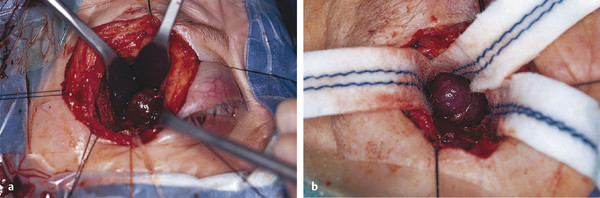
Surgical dissection within the orbit requires a delicate and patient approach. Lesions can often be palpated with the tip of the little finger, which can greatly assist orientation. This can be done at regular intervals if the lesion cannot be easily identified. Gentle blunt dissection should be undertaken using Wright’s retractors in a hand-over-hand dissection technique. Once the surface of the lesion has been exposed, the blunt tip of a Freer periosteal elevator can be used to gently separate the tissues and fat from the surface of the lesion. As the plane of dissection proceeds, the retractors can be repositioned (Fig. 19‑7a). The dissection can be further facilitated by the placement of neurosurgical cottonoids, moistened with saline, into the wound (Fig. 19‑7b). The retractors are then placed over these to prevent the prolapse of orbital fat into the surgical field. This also enables the efficient use of suction with a Baron suction tip, which is applied against the cottonoid to prevent the suction tip from engaging orbital fat. The inadvertent application of suction directly to the orbital fat can cause undue trauma and orbital bleeding.
Careful dissection with blunt-tipped Westcott scissors or Stevens scissors can be used, where required. The assistant should apply countertraction with the orbital retractors, as the surgeon maneuvers the lesion away from the retractors with a cotton-tipped applicator, retractor, or a combined Freer–suction elevator using the nondominant hand. The tissues are gently dissected from the mass with the scissors in the dominant hand. For deep orbital dissection, blunt-tipped Yasargil neurosurgical scissors (curved or straight) may be used. Occasionally, a cryoprobe may assist the dissection by allowing the lesion to be gently pulled in different directions. A cystic lesion or a cavernous hemangioma may be decompressed with a needle and syringe to facilitate safe dissection from surrounding orbital structures. Some thin-walled cystic lesions (e.g., a dermoid cyst or a lymphangioma) can be injected with Tisseel (off-label use) to solidify the lesion to avoid inadvertent rupture of lesion and to facilitate its dissection from surrounding structures. The pathologist should be informed about its use.
19.4.9 Careful Removal and Presentation of Biopsy Specimens
The management of many undiagnosed orbital lesions requires an orbitotomy procedure with an incisional biopsy to obtain an accurate diagnosis. It is essential to ensure that the pathologist is presented with tissue samples that fit several criteria:
Of adequate size.
Representative of the entire lesion.
Undamaged by cautery or surgical instruments.
Appropriately stored.
It may be necessary to provide more than one tissue sample, depending on the appearance of the lesion. Great care should be taken to ensure that the tissue samples are not damaged. It is preferable to use a right-angled 66 Beaver blade to obtain biopsies from a solid lesion. Small cutting biopsy forceps are more appropriate for lesions that are friable. Very occasionally it is helpful to request a frozen section analysis of tissue samples taken from a small orbital lesion if there is any doubt about the adequacy of a specimen. The pathologist can then confirm that adequate material has been obtained. No management decisions, however, should ever be based on the frozen section analysis of orbital biopsies. If frozen section analysis may be required, it is important to communicate this to the pathologist in advance. The pathology requisition forms should be completed before the commencement of surgery and should provide appropriate clinical information about the patient. The tissue samples should be quickly placed into the appropriate transport container to prevent desiccation. If fresh tissue samples are required by the pathologist, it is essential to communicate with the pathologist in advance and to ensure rapid transportation of the specimens to the pathologist.
It is not appropriate to undertake fine-needle aspiration biopsies of orbital lesions on a routine basis. It can, however, be advantageous to perform an open-approach fine-needle aspiration biopsy for deep orbital lesions from which it would be difficult and potentially dangerous to attempt to obtain a standard incisional biopsy. The surface of the lesion is carefully exposed. An 18-gauge needle (green) is attached to a 5-mL syringe. The needle is placed into the lesion and moved back and forth, while withdrawing on the plunger. The needle is carefully capped and the needle and syringe are sent to the cytopathologist.
Key Point
No management decisions should ever be based on the frozen section analysis of orbital biopsies.
19.4.10 Good Hemostasis
Good hemostasis is an extremely important prerequisite for successful orbital surgery. The fundamental principles underlying the successful achievement of good hemostasis are outlined in Chapter 1. For orbital dissections, some points require emphasis:
Only bipolar cautery should be used within the orbit.
Insulated bayonet bipolar forceps with delicate tips should be used.
The minimum power required for the cautery should be used.
The minimum amount of cautery required should be used.
Gelfoam soaked with thrombin can be applied to the orbital wound during surgery and after removal of the orbital lesion to assist in hemostasis when there is generalized oozing without an identifiable source amenable to bipolar cautery. The Gelfoam is carefully removed before closure of the wounds.
For some orbital procedures a safe degree of hypotension is advantageous. The anesthetist should be asked to restore a normal level of blood pressure after removal of an orbital lesion to ensure that intraoperative hemostasis is adequate before the orbit is closed. It is inevitable that the patient’s venous pressure will rise on extubation. It is therefore reasonable to apply a compressive dressing supported by a bandage at the completion of surgery to tamponade the orbit and to remove this in the recovery room as soon as the patient is awake and cooperative. The anesthetist should be warned about the need to apply the dressing after the completion of surgery so that the anesthetic is not reversed too soon.
19.4.11 Good Postoperative Care
Good postoperative care is essential for a favorable outcome of orbital surgery. The following general points should be observed:
Instructions should be given for the patient’s head to be kept elevated 30 to 45 degrees. If possible the patient should sleep with the head elevated for a period of 2 to 3 weeks postoperatively.
The patient must be instructed to avoid bending, lifting weights, or straining for at least 72 hours, because this raises venous pressure with the risk of provoking an orbital hemorrhage. The patient should be instructed to avoid vigorous coughing and should sneeze through an open mouth.
The dressings should be removed in the recovery room as soon as the patient has recovered from the effects of general anesthesia sufficiently to cooperate with a baseline assessment of visual function and no later than 15 minutes after surgery.
The patient’s visual acuity and pupil size and pupil reactions must be checked hourly for 12 hours.
A cool pack should be applied to the periorbital area intermittently for 24 to 48 hours.
Instructions should be documented that the patient must be observed by the nursing staff at regular intervals for bleeding, pain, sudden or progressive proptosis, and excessive postoperative swelling. Any such problems should be reported to the surgeon without delay.
No opiates should be prescribed routinely for pain management. Any complaint of pain should be followed by an immediate examination of the patient to exclude signs of a retrobulbar hemorrhage.
The patient should be kept on nothing by mouth for a few hours postoperatively as a precaution. If a sudden retrobulbar hemorrhage were to occur, causing an orbital compartment syndrome, the patient would have to be returned to the operating room immediately for the orbit to be re-explored and the source of bleeding stopped. Should this occur, an immediate lateral canthotomy and inferior cantholysis should be performed and medical therapy given to lower the intraocular pressure without delay.
Systemic corticosteroids are usually prescribed for a period of 6 days after surgery unless their use is contraindicated (commencing at approximately 60 mg of prednisolone and reducing by 10 mg per day), and topical antibiotic ointment is prescribed for the wound. The steroid dose should be adjusted according to the patient’s size.
Systemic antibiotics are only used for specific indications, including previous infection, foreign bodies, and exposure of the paranasal sinuses.
Key Point
No opiates are prescribed for pain management. Any complaint of pain should be followed by an immediate examination of the patient to exclude signs of a retrobulbar hemorrhage.
Related posts:




Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


