19 Dermabrasion, Chemical Peels, and Dermaceuticals
Introduction
Facial skin resurfacing and skin care are burgeoning fields within facial plastic surgery. In 2013, over 2.1 million skin rejuvenation procedures were performed, a 23% increase from 1997. 1 Across all cultures, the cornerstones of youthful, attractive skin include uniform distribution of pigment; smooth, tight skin; and an absence of rhytids. These are the ideals that facial rejuvenation seeks to achieve. Within this chapter, we address two mainstay techniques in facial skin resurfacing: dermabrasion and chemical peels. Furthermore, we will discuss topical therapies utilized in skin care.
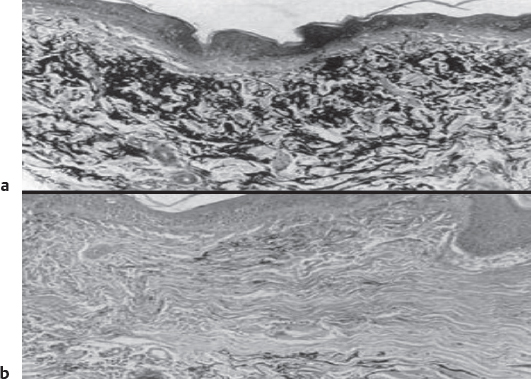
Photodamage and other extrinsic factors cause a number of histologic changes within the skin including degeneration of the elastic network, collagen disorganization, actinic damage, and uneven melanin distribution ( Fig. 19.1 ). 2 , 3 Clinically, these changes manifest as fine and coarse rhytids, uneven skin texture, cutaneous lesions, loss of elasticity, and uneven pigmentation ( Fig. 19.2 ). Facial skin resurfacing is based upon removal of the superficial layers of skin to eliminate these undesirable abnormalities. Re-epithelialization subsequently occurs from adnexal structures within the deep reticular dermis as well as the surrounding epidermis. Dermal remodeling ensues following the inflammatory response caused by tissue injury. Evidence of this remodeling has been shown by increased volume of the papillary dermis and reorganization of reticular dermal collagen. 4 There is restoration of normal cellular polarity and correction of both cellular atypia and melanocytic hypertrophy and hyperplasia ( Fig. 19.1 ). The visible effects are elimination of rhytids, even distribution of pigment, and smoother appearing skin ( Fig. 19.3 ). The face is an optimal location for resurfacing due to the high density of adnexal structures.


Patient Selection
Identifying the appropriate patient for dermabrasion or chemical peels is of utmost importance. This requires careful attention to one’s history and physical exam. The Fitzpatrick skin type classification is frequently utilized to categorize patients ( Table 19.1 ). 5 The Fitzpatrick scheme is helpful because the complications associated with facial resurfacing generally increase with darker skin types. A classification scheme that is helpful in rating patient skin quality and severity of photodamage is the Glogau skin classification ( Table 19.2 ). 3
Classification | Skin color | Tanning pattern | Burning pattern |
Type I | Very white | Never tans | Always burns |
Type II | White | Tans minimally | Usually burns |
Type III | White to olive | Tans moderately | Sometimes burns |
Type IV | Light brown | Tans readily | Rarely burns |
Type V | Dark brown | Tans profusely | Very rarely burns |
Type VI | Black | Tans profusely | Never burns |
Source: Modified from Fitzpatrick. 5 | |||
Dermabrasion is frequently employed in scar revision. Acne, surgical, and traumatic scars may all be addressed with this modality. Dermabrasion is useful in smoothing raised or irregularly bordered scars. Many surgeons routinely utilize dermabrasion 6 to 8 weeks following surgical repair. During this time period of fibrillogenesis, re-injuring the area with dermabrasion can lead to increased epithelial cell migration and subsequently result in a smoother, less conspicuous appearance of the wound. 6
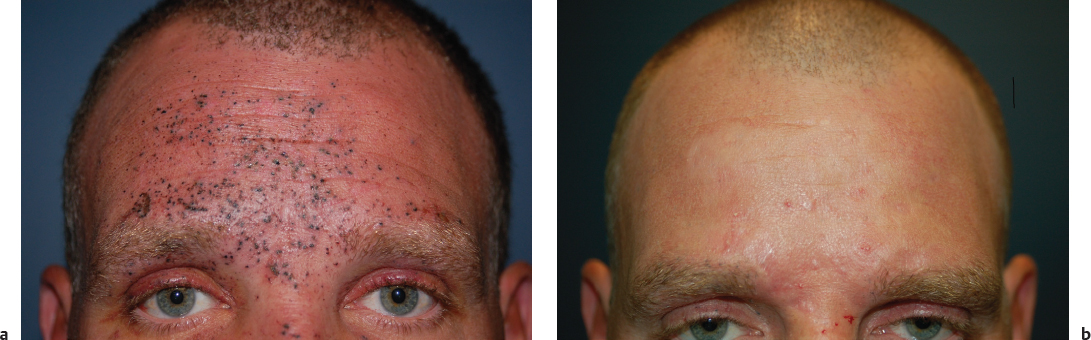
Dermabrasion can also be used to treat signs of photodamage including superficial rhytids, dyschromias, and premalignant actinic keratoses. These changes are often widespread across the face; therefore, modalities such as chemical peels and laser resurfacing, which are less time consuming and easier to maintain uniform depth, have largely supplanted dermabrasion for these indications. More focal abnormalities, such as rhinophyma or benign growths like syringomas, may be treated successfully with dermabrasion. Traumatic tattooing of the face may also be addressed with this modality ( Fig. 19.4 ). Microdermabrasion is an additional technique that is used for treatment of comedonal acne and superficial resurfacing.
Whereas dermabrasion is utilized more often in treatment of focal abnormalities, chemical peels, or chemexfoliation, are used for widespread treatment of the face. The most common indications for chemical peels are pigmentation changes and facial rhytids. Lentigenes and dyschromias, including melasma and postinflammatory hyperpigmentation (PIH), may be addressed with superficial and medium-depth peels. Moderate and deep rhytids indicate significant dermal changes and typically require medium and deep chemical peels for improvement. Chemical peels can also be used as an alternative to medical management to treat premalignant lesions and as an adjunct to other treatment modalities used for scar revision.
Contraindications
Processes that impair the rate of reepithelialization, such as connective tissue disorders and immune compromise, are considered absolute contraindications to dermabrasion and chemical peels. Isotretinoin use is another absolute contraindication and should be withheld for 6 to 12 months prior to resurfacing. It induces sebaceous gland atrophy and impairs keratinization, thereby placing patients at increased risk for scarring. Patients with active infectious or inflammatory processes such as oral herpes simplex virus infections and severe acne should be withheld from treatment (until well managed). Previous head and neck irradiation is a relative contraindication.
Patients with darker skin pigmentation (Fitzpatrick IV to VI), in particular, non-Caucasian skin types, should be cautioned about the increased risk of scarring and dyspigmentation. A personal or family history of keloid formation is a relative contraindication. Any patient with elevated estrogen levels is a poor candidate for dermabrasion and chemical peels due to the risk of PIH. Therefore, those taking oral contraceptives or exogenous hormone replacement or women planning to become pregnant within 6 months following the procedure should be cautioned. Photosensitizing drugs also need to be avoided.
Phenol-based peels place patients at increased risk for cardiac arrhythmias as phenol is cardiotoxic and readily absorbed transcutaneously. Phenol is metabolized and excreted both hepatically and renally; therefore, patients with severe hepatic, renal, or cardiac dysfunction are not candidates for phenolbased peels.
One must develop a sense of the patient’s mental preparedness and expectations prior to dermabrasion or chemical peels. Optimal patient outcomes necessitate strict adherence to pre- and postoperative regimens. Lifestyle activities need to be assessed. Patients with habitual sun and smoke exposure should be counseled on the damaging effects that ultraviolet (UV) radiation and smoke can cause in the first several months following treatment. Those patients who cannot abide by these limitations should be recommended for alternative therapies.
Preoperative Measures
Prophylactic measures may help to optimize healing and final skin outcomes prior to resurfacing. This is particularly important for patients at increased risk of postoperative complications (e.g., Fitzpatrick III to VI). UV protection in the form of broadspectrum (UV-A and UV-B) sunscreen with at least sun protective factor 30 is recommended up to 3 months prior to resurfacing. Doing so stabilizes melanocyte activity and prevents prepeel burns or tanning. Sunlight exposure should also be minimized during this time. Tretinoin (Retin-A [Valeant Pharmaceuticals]), 0.025 to 0.1%, hydroquinone (4 to 8%), and hydrocortisone (1 to 2.5%) are topical therapies that may be initiated 6 weeks before the peel. These medications increase the reepithelialization rate, create uniform thickness of the stratum corneum, stabilize melanocytes, improve melanin distribution, and reduce local inflammation. 7 , 8
All patients should be started on antiherpetic prophylaxis. Latent infections may arise even in the setting of a negative history. By adulthood, it is thought the majority of the population is seropositive for herpes simplex virus, type 1. 9 Patients with a negative history are regularly started on acyclovir, 400 mg three times a day, initiated 3 days prior to the peel and continued 10 to 14 days. Anyone with a history positive for oral herpetic outbreaks should be provided 1 g of valacyclovir three times a day for the same duration.
With dermabrasion and chemical peels, there is potential for bacterial contamination. Cutaneous flora such as Staphylococcus and Streptococcus species are the common causes of postresurfacing cellulitis. Because of its additional utility in treating acne, the authors initiate prophylactic minocycline, 100 mg once daily, starting the day prior to resurfacing and continuing for 10 days total.
Dermabrasion
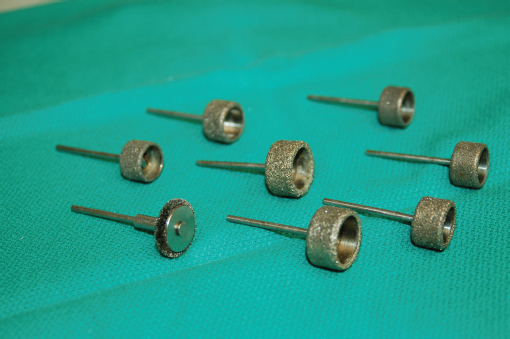
Dermabrasion has been practiced in modern society since the 1940s, when Kurtin first described the use of the mechanized wire brush technique. 10 The technique involves mechanical destruction and removal of the epidermis and papillary dermis. Dermabrasion is most often performed with automatic machines but may also be accomplished with manual techniques. The mechanical handpieces are fitted with either a wire brush or diamond fraise, though many advocate the latter for improved control ( Fig. 19.5 ). 11
Microdermabrasion is a relatively newer technique that allows removal of the stratum corneum. Polyester or nylon bristles or elements such as glass or aluminum oxide crystals are disbursed onto the face at various speeds followed by suctioning the debris with a handheld vacuum. The suction piece can be operated at various pressures to control the particle speed and suction at the surface of the skin. 12 Alternative microdermabrasion handpieces eliminate the use of crystals and their associated complication risks by using a fine tipped diamond handpiece coupled with a suction unit (Parisian Peel [Aesthetic Technologies, Inc.]) ( Fig. 19.6 ).

Operative Management
Anesthesia
Isolated areas may be treated under local and regional anesthesia. Supraorbital, supratrochlear, infraorbital, and mental nerve blocks are often implemented. Treatment of larger areas may require intravenous (IV) sedation. Patients are given 10 to 15 mg of diazepam and 100 mg dimenhydrinate 1 hour prior to the procedure. Midazolam is also provided at the outset of the procedure.
Operative Technique
The mechanical handpiece may be fitted with a wire brush or diamond fraise. The wire brush requires more technical skill and carries an increased risk of complications secondary to a faster cutting speed and less visual and tactile feedback. The handheld diamond fraise allows improved control. Treatment should be conducted in areas roughly 3 to 4 cm2. Some advocate the use of a coolant to the skin to make the surface more rigid and the results of resurfacing more uniform. Avoid nearby loose objects, such as 4 × 4 gauze or towels, as they can easily be taken up in the rotating handpiece, resulting in loss of control and injury to the patient. An assistant should apply outward tension to the skin, thereby keeping the operative surface as flat and taut as possible. This is particularly important along curved regions of the face and areas of thin or loose skin.
To ensure the sanding component is evenly applied to the skin, it should always be oriented perpendicularly to the surface of the skin. Movement of the handpiece should proceed in the direction of the handle, perpendicular to the direction of rotation. If used for scar revision, dermabrasion proceeds in an orientation perpendicular or oblique to the long axis of the scar ( Fig. 19.7 ). Entry into the papillary dermis will violate dermal capillary loops, indicated clinically upon visualization of punctate bleeding. Penetration of the reticular dermis reveals a chamois color and white collagen fibers are seen arranged in parallel, indicating sufficient depth. 11 Penetration deeper into the reticular dermis can injure adnexal structures and cause scarring. Feathering around the periphery helps achieve a smooth transition to untreated areas.

Manual dermabrasion, or dermasanding, is an alternative to the mechanized technique. This method is useful in areas of thin skin and irregular contour (e.g., periorbital, nose). Individual techniques vary; however, one described technique involves initially using a coarse (200-grade) sandpaper until pinpoint bleeding is visualized. This is followed by smoothing the area with a finer (400-grade) sandpaper. 13
Related posts:






Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


