19 Correction of Arm Ptosis with a Medial Bicipital Scar

Abstract
Brachioplasty has undergone a resurgence due to the increased number of patients who present to plastic surgeons following massive weight loss. In this chapter, we present our technique for brachioplasty that addresses the upper arm, axilla, and lateral chest wall as a combined aesthetic unit. This procedure results in a visible scar in the bicipital sulcus that improves over time. Patients must be adequately counseled as to the potential scarring, scar position, and complications. Overall patient satisfaction with this procedure is high.
Introduction
Severe arm ptosis as a result of massive weight loss (MWL) can be a source of significant distress in many patients, especially women. These deformities are not as easily disguised by clothing as other body parts, prompting many patients to seek correction. There is a wide variety in presentation of these upper extremity contour deformities. The majority of patients who present for correction of arm ptosis have significant volume loss with extensive skin laxity of the upper arm. The deformity most commonly involves the arm proximal to the antecubital fossa and may extend further proximally into the axilla. Except in cases of ptosis limited to the proximal upper arm and in patients with excess adiposity and good skin tone, we perform an excisional brachioplasty with an axillary extension to correct these deformities.
Brachioplasty is not a new procedure; however, it has had a resurgence in popularity, given the increasing number of patients who have undergone MWL through either bariatric surgery or lifestyle changes. Aesthetic brachioplasty was initially described by Correa-Inturraspe and Fernandez1 in 1954. Since this first description, many variations have been described to improve scar appearance and location and to reduce the incidence of contracture. Modifications included scar placement in the medial bicipital sulcus and the use of Z-plasties, W-plasties, and L-shaped excisions to minimize axillary wound contracture.2–12 Lockwood6 described suspension of the superficial fascial system (SFS) of the arm flaps to the axillary fascia to minimize tension on the skin, thus reducing the risk of thickened scars and scar migration. Liposuction has also been a useful adjunct to improve the aesthetic outcomes from brachioplasty and, in certain cases, can be used as the sole modality.13
Because the majority of patients present with significant laxity of the upper arm and axilla, our preferred technique is an excisional brachioplasty that extends distally to the antecubital fossa. To correct the axillary redundancy, the re-section is also continued proximally into the axillary region. In our opinion, hemielliptical excisional brachioplasties that limit the incision to the axilla can be used only to correct laxity limited to the proximal one third of the upper arm. Although scar placement remains a matter of debate, we prefer our incision to lie within the medial bicipital groove. In this position, the scar is well hidden and becomes visible only with the patient’s arm in abduction. Liposuction can be a useful adjunct to remove residual fat deposits that lie outside the area of resection. If liposuction is indicated, we perform suction-assisted lipectomy immediately following tumescent injection and prior to the resection.
Indications
The decision as to which procedure to perform must be individualized to each patient and depends on the location and severity of the deformity. The Pittsburgh Rating Scale was created not only to describe the severity of the preoperative deformity of a specific anatomic region, but also to help determine which surgical strategies may be effective to treat a given deformity.14 Patients with a grade I deformity have significant adiposity with good skin tone and tend to be young. These patients would be good candidates for liposuction alone. In cases where it is not clear whether lipo-suction alone will result in skin laxity, liposuction may be performed as an isolated procedure in patients who refuse to have a scar placed on their arm. This is performed only with the understanding that an excisional procedure may be necessary if the patient is dissatisfied with the skin laxity.
Patients with grade II deformities have loose, hanging skin without severe adiposity. Patients with grade III deformities have loose hanging skin with severe adiposity. Both of these deformities require direct excision to contour both the arm and the axilla; however, patients with grade III deformities may also require adjunct suction-assisted lipectomy of residual fat deposits that lie outside the zone of resection to achieve and optimize the final contour. When assessing these patients, it is important to note the distribution and extent of the skin laxity in the arm, axillary region, and lateral chest wall. To properly contour this area, it is important to treat the arm, axilla, and lateral chest wall as a combined aesthetic unit.
Body-contouring procedures involve a trade-off of shape for scar. This concept is best exemplified by brachioplasty in that the scar is very prominent and visible. It is common for this scar to remain thick and red for many months following the procedure before maturing and becoming less noticeable. Preoperative counseling and management of a patient’s expectations are critical to ensuring a satisfied patient. We find it useful to show patients pre- and postoperative photographs at different time intervals to demonstrate the maturation of the scar.
Because brachioplasty is considered an elective procedure, we prefer that patients are near their goal weight, have a favorable body mass index (BMI), and are weight stable for a minimum of 3 months. Brachioplasty is commonly performed during the first or second stage depending on the patient’s priority. At our center, it is rare for brachioplasty to be performed alone. Almost all of our cases (96%) were performed as part of a multiple procedure stage. Patients who present with severe, debilitating arm ptosis may be candidates for an isolated brachioplasty despite a high BMI (>35 kilograms per height in meters squared) if they do not have medical contraindications. These patients must be counseled that their risk for recurrent ptosis is high and that they will likely require a future revision.
A thorough history and physical examination are done with every patient, including an evaluation of nutritional status.15 We have a low threshold for medical consultation as clinically indicated. There are relatively few contraindications to this procedure. Patients with preexisting upper extremity lymphedema are often deferred from surgery because this may worsen their condition. Patients who have had an axillary lymph node dissection or previous radiation to the axilla are counseled as to the increased risk of lymph-edema and may also be deferred from surgery. Active smokers must stop smoking for a minimum of 4 weeks prior to surgery. Smoking cessation is confirmed by urine nicotine testing.
Technique
The surgical goals for correction of the skin laxity of the upper arm and axilla include the following:
Proper scar placement in the bicipital groove
Elevation of the axillary fold
Even resection
Avoidance of overresection
Preservation of the medial antebrachial cutaneous (MABC) nerve
Correction of lateral chest wall laxity
Markings
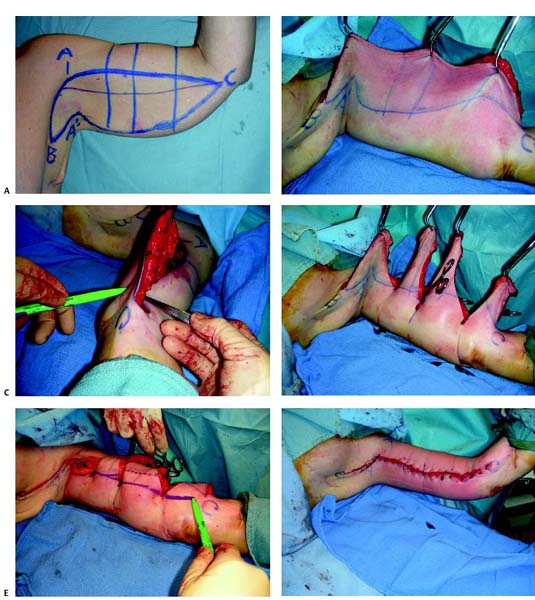
The zones of adherence in the arm are more diffuse as compared with the trunk, and, as a result, there is often circumferential movement of the skin and subcutaneous tissues. For this reason, accurate preoperative markings are required to predict scar placement. The patient should be marked in the standing or sitting position with the arm abducted 90 degrees at the shoulder with the elbow bent at 90 degrees. The brachioplasty markings are shown in Fig. 19.1A . The first marking is the bicipital groove, which represents the desired final position of the incision. We try to limit the distal extent of the incision to the level of the elbow (point C). Placement of the incision in the bicipital groove allows any scar that crosses the elbow to be positioned in the midaxillary line in relation to the joint. This allows the incision to be extended distally, if necessary, without the concern for joint contracture. Caudal traction is placed on the arm to mark the margins of the upper incision line. Under the tension of wound closure, the upper incision is pulled downward to the level of the bicipital groove. The proximal extent of the superior incision line (point A) is set high in the dome of the axilla. To correct the laxity of the lateral chest wall, a line extending from point A is drawn at a 90-degree angle to the superior incision line onto the chest wall. The length of this extension (terminating at point B) is determined by the severity of the chest wall laxity. The next maneuver is to choose a point in the axilla (point A’) that will reach point A and correct the descent of the axillary fold. This point is estimated with a pinch test. Points A’ and B are connected to estimate the posterior extent of the axillary resection. The inferior line of resection is estimated using a pinch test. We do not commit to this lower resection at the beginning of the procedure to minimize the risk of overresection. Although the degree of laxity may be different between upper extremities, symmetry of the marked points and the extent of resection are confirmed. Vertical references are drawn to assist in symmetrical resection.
Related posts:
 17 Brachioplasty with Interdigitation of the Posteromedial Scar
17 Brachioplasty with Interdigitation of the Posteromedial Scar
 18 Brachioplasty with an Inferior Scar
18 Brachioplasty with an Inferior Scar
 4 Anesthesia and Safety Considerations in the Perioperative Period
4 Anesthesia and Safety Considerations in the Perioperative Period
 12 Combination Abdominal Wall Hernia Repair and Mid-Body Contouring
12 Combination Abdominal Wall Hernia Repair and Mid-Body Contouring
 32 Combination Circumferential Abdominoplasty with Medial Thigh Lift
32 Combination Circumferential Abdominoplasty with Medial Thigh Lift
 36 Facial Rejuvenation: Open Technique
36 Facial Rejuvenation: Open Technique
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


