12 Combination Abdominal Wall Hernia Repair and Mid-Body Contouring

Abstract
Incisional hernias are a common complication following bariatric surgery, especially open surgery. Massive weight loss patients, in particular, have been shown to have a higher risk of postoperative incisional hernias. These hernias may have both functional and aesthetic sequelae. Generally, a traditional or circumferential abdominoplasty can be performed in the usual manner, and the incisional hernia can be repaired by the plastic surgeon or the general surgeon after the abdominal flaps are raised. The hernia can be repaired either with or without mesh; components separation can additionally be performed at the time of the hernia repair if it is deemed necessary to medialize the abdominal wall fascia. The combination of incisional hernia at the same time as mid-body contouring has been shown to be a safe and effective procedure.
Introduction
Although there is an increasing trend toward minimally invasive bariatric surgery, there is still a very high percentage of patients undergoing open gastric bypass surgery. Although incisional hernia is not the most common overall complication from gastric bypass surgery, it is still very common,1–4 with reported rates as high as 41%.5 Incisional hernia is considered to be the most commonly encountered technical problem following open gastric bypass surgery.6 Massive weight loss patients are considered to be at a higher risk of incisional hernia postoperatively than patients of normal weight. This is thought to be due to poor tissue quality, malnutrition, and changes in abdominal wall girth.7 There is significant functional disability associated with incisional and ventral hernias in addition to the cosmetic deformity, including pain, discomfort with movement, and impairment of mobility. These symptoms can restrict patients from adequately performing normal daily activities and possibly prevent them from attending work.8 The ideal choice of technique in hernia repair has long been debated. The current standard of care in ventral incisional hernia repair is an underlay mesh repair. This is based on reports that mesh repair has a lower recurrence rate than primary suture repair.9 The underlay position of the mesh has also been shown to be superior.10 The use of mesh in the underlay position allows for a tension-free hernia repair, which is possibly the most important factor in preventing hernia recurrence. In the case of the postbariatric patient, there is usually an excess of fascia, which can be used to plicate and perform a stable, tension-free, primary herniorrhaphy for small hernias, with larger hernias requiring a mesh closure.11 Components separation can be considered for large and recurrent hernias. Concurrent hernia repair during abdominoplasty has been shown to be a safe procedure.7
Indications
The indication to perform hernia repair at the time of mid-body contouring is straightforward and includes the presence of an incisional or ventral hernia in a patient with excess skin and subcutaneous tissue following massive weight loss. Contraindications include an incarcerated hernia that requires emergent repair or a high index of suspicion for strangulation and bowel injury that may require a small bowel resection. The complications associated with an incisional hernia that is not repaired include gradual enlargement, abdominal discomfort and nausea secondary to bowel mesentery stretching through the defect, bowel obstruction with the risk of incarceration and strangulation, respiratory derangements, inability to maintain posture, and, possibly, difficulty with expulsive functions such as coughing, micturition, and defecation.12 The preoperative work-up should include a comprehensive history and physical exam. The patient’s goals and expectations should be discussed thoroughly. Weight loss should have reached a plateau at the time of consideration for abdominoplasty and hernia repair. Smoking cessation should be greatly encouraged, as smoking has been found to be an independent risk factor for complications following abdominoplasty.13 The physical exam’s focus should be on the abdomen, the mid-body skin, and the hernia itself. With the patient in the supine position, the hernia should be assessed for size, evidence of incarceration, and overlying skin changes. It is important to estimate the size of the hernia preoperatively for the purposes of operative planning and ordering the proper-size mesh if one is to be placed. The patient should then be examined in the standing position to evaluate skin laxity and subcutaneous fat. Often these operations are performed with the assistance of a general surgeon, and preoperative consultation should be sought. Components separation has been utilized as an adjunct to many large hernia repairs. The goal of the components separation is to allow greater mobility of the abdominal wall when repairing large ventral or incisional hernias. Studies have demonstrated that the external oblique muscle can be separated from the internal oblique muscle in a relatively avascular plane.14 This can be a useful adjunct to hernia repair that allows native tissue to be utilized for the purpose of reducing tension on the hernia repair and can be combined with an underlay mesh, an onlay mesh, or a biologic matrix.
Technique
The procedure begins in the preoperative holding area, where all skin markings are drawn. The markings consist of the standard markings for an abdominoplasty or circumferential abdominoplasty, depending on the procedure being performed. The markings should be tailored to the size of the patient and the amount of skin that is thought necessary to be removed. The patient is then brought into the operating room, sequential compression devices are placed, anesthesia is induced, antibiotics are given, and a Foley catheter is placed. Now, a proper skin preparation with an antimicrobial solution is performed. The operation commences with an incision through the lower abdominoplasty marking, which is carried down with cautery through the subcutaneous tissue to the anterior surface of the abdominal wall fascia. The abdominal wall flap is raised until the hernia sac is reached and exposed, then continued crani-ally to the xiphoid process in the midline and approaching the costal margins laterally. Dissection of the flap is limited laterally as much as possible. A circular incision is made around the umbilicus, and dissection is carried down to the abdominal wall fascia surrounding the umbilical stalk. The umbilicus remains in its place until it is to be reset into the new abdominal wall. There are circumstances in which the umbilicus is involved in the hernia sac, and the surgeon must decide if there will be adequate vasculature to supply it, as well as whether the hernia can be effectively repaired around it. In some instances, the umbilicus must be sacrificed, and a neo-umbilicus can be constructed after the hernia is repaired and the flaps are ready to be set. Great care is taken to ensure adequate hemostasis at all times.
Once visualized, the hernia sac is dissected from the fascia and, in some instances, entered. Any intraperitoneal adhesions or attachments that are interfering with the hernia repair are released. The decision is now made whether to perform a direct primary suture closure or a mesh closure, with or without a components separation. Primary suture repair can be accomplished with running or interrupted sutures. Sutures should be secured 1 cm from the edge of the fascia and advanced in 1 cm increments.8 In the case of a mesh closure, the optimal position of the mesh is in the prefascial, retromuscular space;15 in this case, the mesh lies superficial to the posterior rectus sheath and deep to the rectus muscle. This space exists only in incisional hernias occurring above the arcuate line. The arcuate line is a horizontal line cranial to which the internal oblique and trans-versus abdominis aponeuroses comprise the posterior rectus sheath; caudal to this line, these aponeuroses merge, course superficially, and join the external oblique aponeurosis to form the anterior rectus sheath. The exact position of this line varies among patients, but it is usually found one third of the distance from the umbilicus to the pubis. In incisional hernias occurring below the arcuate line, attempts should be made to place the mesh in the preperitoneal space. Often it is not possible to create these pockets without entering the peritoneal cavity. In this situation, the selection of mesh is important and should include a dual-layered mesh with the intraperitoneal side resistant to adhesions.
A variety of meshes with different properties are available. There are three major types of synthetic mesh: polypropylene, polyester, and polytetrafluoroethylene (PTFE).16 Each type of mesh has specific properties that differentiate it from the other meshes. All three types of mesh are flexible, thus making them more comfortable than older meshes and allowing them to conform well to the abdominal wall. Polypropylene and polyester are both strong and have good tissue in-growth, although polyester’s strength does deteriorate over time. PTFE, alternatively, does not have good in-growth, and therefore is rarely used by itself but rather as the intraperitoneal layer of a combination mesh. These combination meshes usually have two layers: a strong layer susceptible to in-growth, usually composed of polypropylene or polyester, and an intraperitoneal layer that resists in-growth, usually PTFE. This type of mesh is used in hernias that are repaired intraperitoneally. Other combination meshes do exist, but the basic concepts are the same.
Other types of mesh in hernia repair are absorbable and biomaterial meshes. Absorbable meshes are less often used and include polyglactin 910 (Vicryl, Ethicon, Somerville, NJ) and polyglycolic acid (Dexon™, Covidien, Mansfield, MA). Biomaterial meshes include acellular dermal matrices, such as Alloderm® (LifeCell, Branchburg, NJ) and Strattice® (Life-Cell). Both of these types of mesh are resistant to infection and can be placed in a contaminated field. However, they are not as strong, and recurrence rates may be higher. Biomaterial mesh is being used more commonly in elective, clean hernia repairs; however, its long-term success still remains to be studied. We have additionally found both human and porcine dermal meshes to be useful as onlay reinforcements of primary repairs or components separation repairs. Using the above principles, the proper mesh can be selected. The surgeon must also decide on the size and shape of the mesh, as well as some minor differences in the meshes that are usually of only stylistic importance, such as a mesh that contains or does not contain a skirt.
In the supraumbilical incisional hernia with the retro-muscular, prefascial approach, the plane is created anterior to the posterior rectus sheath. Attempts are made to close the posterior rectus sheath and the peritoneum beneath the mesh to deter contact between the mesh and the intestines. If this is not possible, then a dual-layered mesh should be used. The dimensions of the hernia should be evaluated, and the mesh should be fashioned to allow at least 4 cm of overlap in every direction. The mesh is then secured with sutures to the rectus muscle and fascia overlying it. Fastening of the mesh to the rectus muscle can be aided by a tacking fixation device, such as AbsorbaTack™ (Covidien). The muscle is then reapproximated at the linea alba overlying the mesh.
Infraumbilical hernias occurring below the arcuate line require a preperitoneal repair in which the hernia sac is dissected and a plane is created in the preperitoneal space, while attempting not to enter the peritoneal cavity. Again, the mesh is fashioned to the correct dimensions with 4 cm overlap and secured with sutures and tacks. Lastly, the mesh can be placed intraperitoneally if the retrorectus, prefascial space, or preperitoneal space cannot be created. Emphasis on the use of a dual-layered mesh cannot be overstated in these cases.
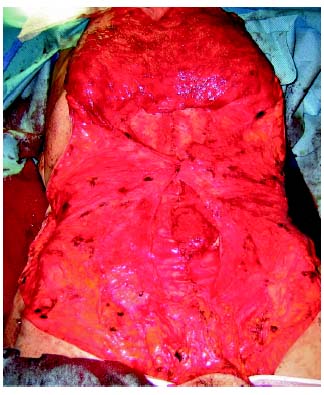
Repair of very large or recurrent ventral or incisional hernias may require the aid of components separation. The technique for performing a components separation involves adequate exposure of the rectus sheath and external oblique fascia ( Fig. 12.1 ). This is already present and is easily accessed through the abdominoplasty flaps that have been raised. An incision is made 2 cm lateral to the edge of the rectus sheath and through the external oblique aponeurosis.17 The external oblique muscle can now be elevated off the internal oblique and advanced medially. This can provide as much as 14 to 20 cm advancement. An additional 2 to 4 cm can be gained by separating the rectus muscle from the rectus sheath. In this way, it is again possible to repair the hernia without the use of a mesh; however, mesh has been used successfully in combination with components separation.18 After the hernia has been repaired, the surgeon may now focus on performing an aesthetically pleasing abdominoplasty ( Fig. 12.2 ). The goals of this surgery include ensuring adequate removal of skin and subcutaneous tissue while preventing undue amounts of tension on the surgical incision. Some patients may have excess fascia or a rectus diastasis in addition to the hernia and may benefit from plication sutures in certain areas, which can also be used to reinforce the hernia repair. We prefer interrupted, figure-of-eight sutures as opposed to running suture for the plication. The operating table should now be placed in 30 degrees of flexion at the patient’s hips. The abdominoplasty can then proceed as discussed in other chapters in this textbook. Two Jackson-Pratt drains are placed through incisions in the mons pubis, secured with sutures, and placed deep to the abdominal flap.
Postoperatively, the patient usually remains in the hospital for 1 or 2 days. The patient should be encouraged to ambulate shortly after surgery, keeping the abdomen flexed. Pain control generally can be obtained with oral medications. The patient is discharged with the Jackson-Pratt drains. They are removed in the office when drainage has decreased to less than 30 cc per drain per day. The patient should be deterred from strenuous activity and heavy lifting for a period of up to 3 months.
Related posts:
 11 Lower Body Lift Combined with Liposuction and Gluteal Flap Surgery
11 Lower Body Lift Combined with Liposuction and Gluteal Flap Surgery
 14 Halfway to a Body Lift
14 Halfway to a Body Lift
 16 Complications and Management Following Mid-Body Sculpting
16 Complications and Management Following Mid-Body Sculpting
 10 Circumferential Abdominoplasty
10 Circumferential Abdominoplasty
 15 Lipoabdominoplasty with Progressive Tension Sutures
15 Lipoabdominoplasty with Progressive Tension Sutures
 13 Circumferential Dermolipectomy of the Lower Trunk: Lower Body Fit
13 Circumferential Dermolipectomy of the Lower Trunk: Lower Body Fit
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


