18 Liposuction of the Face and Neck: The Art of Facial Sculpture
Introduction
The use of suction-assisted lipectomy (SAL) to address changes associated with aging of the face and neck has undergone significant changes since liposuction was initially described. In the early 1970s, Schrudde 1 discussed the concept of “lipoexeresis.” This was performed using a curette to achieve contouring of certain body areas, primarily local adiposity of the thigh and knee. He also described the use of lipoexeresis as a technique for removal of submental fat in facelifting in a later paper in 1980. 2 This description was followed by Fischer and Fischer’s 3 and later Kesselring’s 4 suggestion of placing a tube connected to a suction device through small incisions in a covered field to access fat deposits. A subsequent paper by Ilouz 5 described the technique of injecting hypotonic saline into the proposed surgical site and then using a blunt-tipped cannula with a high vacuum for fat aspiration and lipolysis in the context of body contouring. Adiposity of the face and neck, however, has been a significant hurdle that over the years has thwarted achievement of the ideal surgical result, largely due to the multifactorial nature of aging changes seen in this anatomical region. Liposuction with extraction of fatty deposits was first performed as an adjunct to facelifting procedures, resulting in significantly improved aesthetic outcomes. 6
Building on these concepts, cervicofacial liposuction today can be used in isolation as a primary sculpting and rejuvenation procedure or in combination with other procedures aimed at rejuvenation of the face and neck. Localized adiposity can be met with much consternation by the patient who has gained weight as he or she has aged. Formation of a double chin, loss of definition along the jawline, and an increasingly obtuse cervicomental angle are some of the changes that can lead a patient to seek consultation with a facial plastic surgeon for liposuction. It is important to remember, however, that these changes in the neck should be viewed in the overall context of the aging process. Many factors, including the quality and laxity of the skin, and changes in the underlying bony and muscular structures, can contribute to aging in this region and warrant a thorough evaluation and graduated plan for optimal outcomes. In appropriately selected patients, however, liposuction can achieve dramatic results to restore a more youthful neck and facial contour. In contrast to earlier direct and open methods, suction lipectomy offers important advantages of minimal scarring, reduced tissue trauma, shorter recuperative periods, and well-concealed incisions. In light of these developments, some authors feel that liposuction has revolutionized aesthetic surgery. 7 , 8 , 9 , 10 , 11 The use of smaller cannulas, tumescence of adipose tissue, and the application of ultrasound, laser, and radiofrequency (RF)-assisted techniques are some of the advances that have been seen in this field. 12
General Principles
Localized adiposity may be attributed to hereditary factors, medications, hormonal imbalance, poor dietary and exercise habits, and age-related changes in fat distribution. 12 , 13 Evenly distributed fat stores, unlike isolated facial deposits, 10 , 11 , 19 diminish with exercise and diet. Frequently and unfortunately, the localized deposits are the first to hypertrophy with weight gain and are generally not responsive to weight loss. This isolated adiposity is readily addressed with submental liposuction; however, patients with generalized fat deposition are best served with a weight loss program.
On a cellular level, adipose tissue is composed of adipocytes contained within a connective tissue matrix. The lipid content within a single adipocyte is variable from one cell to another and can change with fluctuations in weight. The connective tissue is composed of collagen and elastin fibers, as well as macrophages, fibroblasts, pericytes, and mast cells. 14 Illouz, one of the pioneers in liposuction, extensively studied the physiology of the human adipocyte. He was able to determine that human adipocytes multiply from birth until puberty and are largely stable in number thereafter. Based on histologic analysis, he described obese children as having a larger number of adipocytes (a hyperplastic state) versus the obese adult simply having enlargement of individual fat cells (a hypertrophic state). 5 Through the incorporation of triglycerides and fatty acid deposits, the overall volume of the fat cell increases. Weight loss is a reduction not in the number of fat cells but rather in their volume. 5 , 15
Given the underlying histologic nature of localized adiposity, surgical intervention should be directed at removing localized fat cells, ideally in a permanent fashion. These diet-resistant fat accumulations are ideal targets for lipocontouring and following removal should respond to weight gain in a fashion that is similar to adipocytes in other regions of the body. As a result, they should be resistant to significant contour changes that are out of proportion with overall weight fluctuation. 15
The use of a rigid, blunt-tipped aspiration cannula that is attached to a suction device continues to be the mainstay for suction-assisted lipectomy (SAL). Recontouring of the overlying soft tissue envelope is achieved through elimination of fat cells by suction-assisted avulsion and subsequent aspiration into the hollow-bore cannula. Traditional liposuction permits a relatively precise reduction in fat cell mass coupled with a low complication rate as compared with direct lipectomy. 3 , 9 Specifically, the tunneling technique of liposuction allows for many of the neurovascular bundles to the skin to be preserved, resulting in a lower risk of hematoma formation, and a return of skin sensation in 3 to 8 weeks. 12 Recontouring then takes place as healing progresses, with contraction of the subcutaneous tunnel network created by the liposuction technique. A carefully designed and evenly distributed tunnel system minimizes bulges and irregularities secondary to localized fat. Early healing irregularities may be seen but are usually fleeting. 7 , 10 , 16 , 17 , 18 , 20 , 21 , 22 Asymmetries, dimples, or bulges that persist beyond 6 months postoperatively are often amenable to additional liposuction, subcutaneous steroid injection, or localized fat injection. 12
As noted above, SAL demonstrates numerous advantages over techniques designed for direct fat excision. SAL eliminates the need for large incisions and reduces operative and recuperative time. The use of SAL in appropriately selected patients allows surgeons to achieve dramatic improvement in face and neck aesthetics, resulting in a high degree of patient satisfaction.
Patient Evaluation
As in all patients seeking cosmetic procedures, a thorough evaluation of the patient’s rationale and stated goals should be elicited as to motivations for seeking liposuction of the face and neck. If the patient’s expectation and goals are within reasonable limits, a thorough evaluation of the face and neck should be performed. This should be done with particular attention paid to areas that may necessitate a modification of the treatment plan from liposuction alone to one that incorporates additional techniques for optimal results (e.g., rhytidectomy, cervicoplasty, skeletal or soft tissue modification/augmentation with alloplastic implants or genioplasty). In addition to the above evaluation, standard preoperative photography should be performed and should include frontal, oblique, and profile views with the neck in both neutral and flexed positions.
Cervicofacial liposuction as an isolated procedure should be limited to those patients with good elasticity of the face and neck skin, without excessive wrinkles or laxity, and lack of visible platysmal banding, and to those with a palpable submental fat mass. This submental fat mass can be further delineated on preoperative assessment by means of palpation with and without contraction of the platysma muscle. If the amount of fat that is palpated in the submentum decreases with platysmal contraction, this may be indicative of deeper lying fat as opposed to fat primarily in the subcutaneous plane. 23
There is a degree of unpredictability associated with submental liposuction, and patients must be counseled appropriately during the preoperative period. Once lipocontouring has been performed, the outcome is dependent on the ability of an individual’s skin to contract and adhere to the underlying tissue. In some cases, it may take up to 6 months to see the final result, and no promises can be made as to what degree of change will occur.
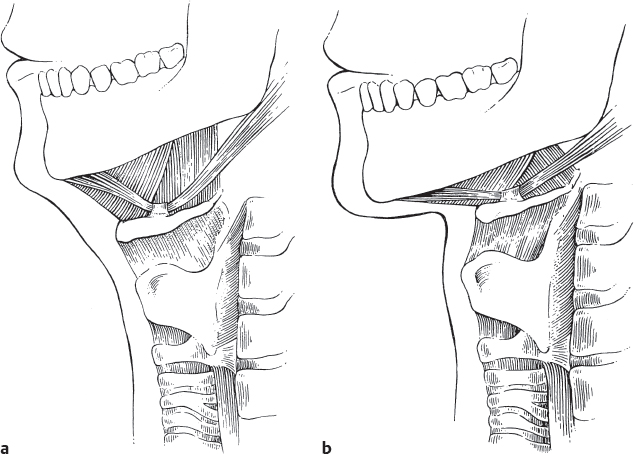
In considering cervicofacial liposuction, the surgeon must thoroughly evaluate the muscular support of the neck, the skeletal configuration of the face and neck, and the patient’s overall body habitus. Conley showed that the position of the hyoid bone in relation to the mentum is the most significant determinant of a desirable cervicomental angle. 24 A low, anterior hyoid position will produce a less favorable result in liposuction than will a high, posteriorly placed hyoid. Additionally, those with a retrusive chin will show less of an effect with liposuction, and in such patients, consideration should be given to concomitant chin augmentation or genioplasty ( Fig. 18.1 ).
The cervicomental angle is measured by an oblique line tangent to the anterior projection of the neck intersecting with a horizontal line through the menton (inferior most point of the chin on profile). The angle should measure between 105 and 120 degrees. 25 Ellenbogen described a total of five visual criteria that he associated with a youthful neck. 25 These are a distinct inferior mandibular border from mentum to angle with no jowl overhang, a subtle subhyoid depression, a visible thyroid cartilage bulge, visible anterior border of the sternocleidomastoid (SCM) muscle in its course from mastoid to sternum (which he found to be the least useful of the criteria), and a cervicomental angle between 105 and 120 degrees 25 ( Fig 18.2 ). He found that an angle greater than 120 degrees gives the patient the visual appearance of a double chin and/or a heavy neck. 25

Similarly, Powell and Humphries describe the mentocervical angle as a means of determining the appropriate contour of the face and neck. 26 This is formed by the angle created by intersecting lines from the glabella (most anterior projecting point of the forehead on profile view) to the pogonion (most anterior projecting point of the chin on profile) and a line from the menton to the cervical point (junction of the submental and cervical regions on profile). They found attractive features were associated with an angle between 80 and 95 degrees. 26 In this classification, an angle greater than 95 degrees is associated with blurring of the distinction between face and neck. 27
In addition to the above metrics, other anatomical landmarks such as relative underprojection of the chin and submandibular position also warrant mention as they can contribute to the appearance of an obtuse cervicomental angle. Ideal chin projection, when viewed from profile, is approximated by dropping a line from the mucocutaneous junction of the lower lip. 28 In males, the chin should project to this point or just beyond it, whereas in females, it may be just shy of the vertical line. Similarly, in an attempt to define the ideal chin position, Gonzalez-Ulloa described a meridian that approximates the ideal position of the chin. 29 , 30 This line is perpendicular to the Frankfort horizontal plane and extends through the nasion. Again, in this measure of chin projection, its ideal configuration is one that projects to this vertical line on profile view. Similarly, ptotic submandibular glands may be the cause of a less acute cervicomental angle.
Adding to the above methods of facial analysis, Dedo proposed a more practical classification scheme for patients seeking cervicofacial rejuvenation. 31 He placed patients into six categories based on the degree of underlying deformity seen in the skin, fat, and underlying bony and muscular structures. 31 In his classification schema, the class 1 neck requires minimal correction, a class 2 neck shows sagging of the skin without excessive fat or platsymal banding, class 3 patients have submental liposis, and class 4 patients have significant platysmal banding. In addition to submental fullness, patients with class 5 have microgenia and those with class 6 have a low anterior hyoid position. 31 Dedo created this classification as a preoperative means of assessing patients and tailoring treatment to best address the underlying deformity. In this classification, type 1 patients with accumulation of moderate amounts of submental fat and younger patients in class 3 are ideally suited to treatment with submental liposuction ( Fig. 18.3 ).

Moreover, with increasing laxity of the skin and platysmal banding, additional procedures such as formal cervicofacial rhytidectomy and platysmaplasty are necessary to correct the underlying anatomical deformities. Finally, Dedo stressed the need for correction of a retrusive chin and an awareness of the role that hyoid location plays in creating an unfavorable milieu for neck rejuvenation. More recently, McCollough, Rohrich, Matarasso, and others 32 , 33 , 34 , 35 have proposed classification systems that similarly categorize patients based on anatomy and degree of aging to assist in the selection of the appropriate technique for correction of the aging face and neck.
While the above classification systems are useful for preoperative assessment and can be useful in patient education, it has been our experience that patients who demonstrate localized adiposity out of proportion to the remainder of the body will benefit most from a localized fat removal procedure. Skin elasticity and muscle tone usually are good indicators of postoperative skin contraction and redraping of the soft tissue envelope; therefore, younger patients are generally more appropriate candidates. Overweight patients should be at the lower end of their usual range, with any planned weight loss taking place several months prior to the procedure. If these patients have had dramatic fluctuations in their weight, they may have lost the needed skin elasticity for later contraction.
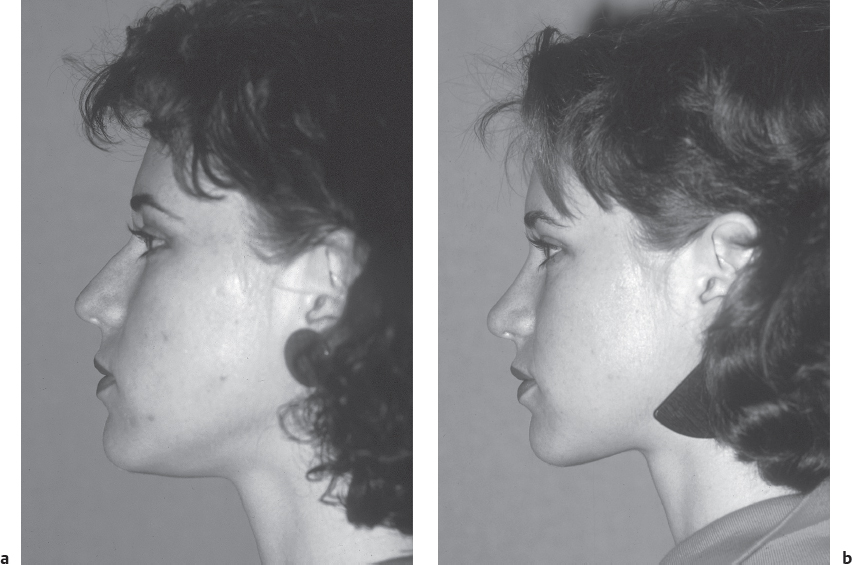
In general, women have greater skin elasticity than men and are better candidates for closed cervicofacial liposuction as a primary procedure ( Fig. 18.4 ). In addition to greater elasticity, women tend to have thinner skin that contracts over the reduced subcutaneous bed. This is not to say that men are not to be considered for this procedure. Expectations simply need to be tempered for this subset of patients. Despite these general guidelines, we have had older male patients exhibit significant skin retraction, and younger patients who did not, again demonstrating the unpredictability that can accompany this procedure when it is performed in isolation.
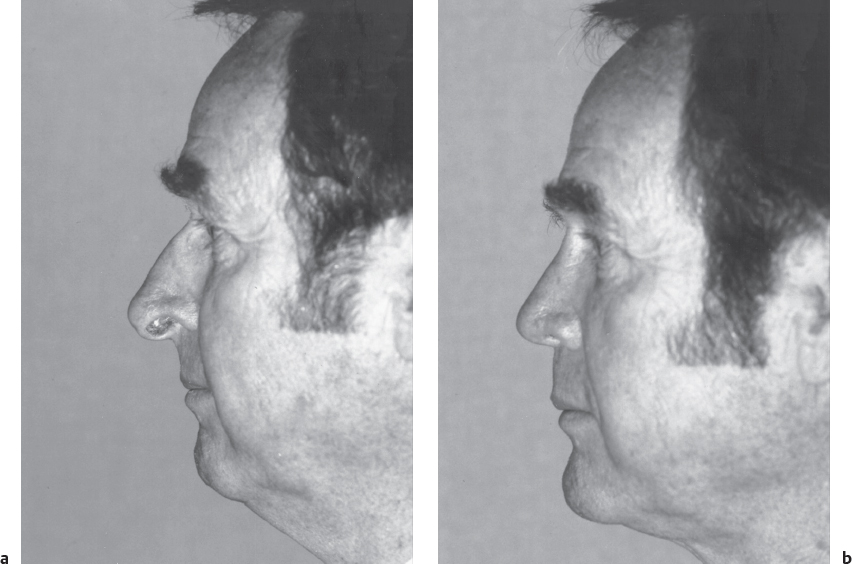
Inappropriate candidates for cervicofacial liposuction as an isolated procedure are those who present with prominent wrinkling of the skin, significant ptosis of the muscular sling, and prominent platysmal bands. In addition, the shape of the neck is determined by the position and tone of the platysma muscle, and when a wide diastasis, prominent banding, or asymmetry is present, a formal platysmaplasty, and not isolated submental liposuction, is indicated. In some cases, correction of the platysmal bands by plication may result in submental skin redundancy. Similarly, redundant and inelastic skin, often fails to redrape appropriately after the removal of moderate to large amounts of subcutaneous fatty deposits. 7 , 20 , 21 , 22 , 36 , 37 Exceptions certainly do occur, and some patients can have marked improvement with cervicofacial liposuction alone ( Fig. 18.5 ).
As noted above, platysmal banding will not be eliminated with cervical liposuction alone and, in fact, may be exacerbated by fat resection. Liposuction can unmask platysmal banding in patients with significant submental fat, especially when the platysma has a pattern of nondecussation in the midline. 38 This can produce a cobra deformity of the submentum with hollowing centrally in the area of fat removal and relative fullness created by the platysmal bands laterally.
In a retrospective review of 301 patients who underwent rejuvenation of the face and neck, Kamer et al attempted to define preoperative factors associated with suboptimal results in rejuvenation of the face and neck. Of the 301 patients treated with various means of rejuvenation (liposuction alone, liposuction with rhytidectomy ± superficial musculoaponeurotic system [SMAS] retrodisplacement and formal platysmal plication), 20 patients (6.6%) were found to have postoperative banding. Only 7/20 patients opted for surgical correction, and all were found to have an undecussated platysma at the time of reoperation. Furthermore, the authors noted that treating the posterior aspect of the SMAS alone did not yield longterm improvement in platysmal banding, thereby underscoring the importance of formal plication to correct the underlying deformity inherent to the platysma. While nondecussation of the platysma can be difficult to discern in a patient with significant submental liposis, they advocate direct treatment of the platysma in the midline if this finding is noted at the time of surgery. 38 As a result, the patient with significant banding or cording should be informed preoperatively of the need for either a platysmal plication or a full rhytidectomy for optimal results.
In a subsequent analysis of submental liposuction, Bank et al 39 evaluated 58 patients between the ages of 40 and 75, 20 of whom underwent submental liposuction. Of these 20 patients, the average age was 57 years (range: 40–74), the average volume of fat extracted was 75 mL (range: 25–125), and the average amount of lidocaine used was 4 mg/kg (range: 1.5–6). All patients were noted to have good to excellent results, no significant complications, and no problems with excessive skin sagging or unfavorable skin redraping.
Finally, skin irregularities and asymmetries should be noted and discussed with the patient preoperatively. With rare exceptions, dimpling, depressions, and scarring will not improve with liposuction alone, and may become more pronounced with a change in neck contour.
Indications
While the focus of this chapter is the aesthetic use of liposuction in the head and neck for removal of localized adiposity, liposuction can be used to manage a variety of other surgical conditions. It can be used to elevate rhytidectomy skin flaps atraumatically, 11 to defat pedicled or free flaps, 40 and it can also be effective for the removal of benign fatty tumors. 41 , 42 Additionally, its use has been described to correct submental lymphedema in head and neck cancer patients, 43 , 44 and in benign symmetrical lipomatosis (Madelung’s disease/Launois-Bensaude syndrome), especially when used for smaller lesions and in combination with ultrasound-assisted liposuction. 45 , 46
When used in isolation as a closed technique (through a small incision) without muscle or SMAS elevation, suspension, excision, plication, or imbrication, liposuction’s greatest effect is seen in creating improvement in the cervicomental angle and, when used judiciously, in the jowl region. The open technique implies liposuction over fat deposits under direct visualization, generally in association with rhytidectomy. The nasolabial folds and the lower jowl fat pads have both been addressed with the use of closed liposuction with less predictable results in the absence of controlled longterm followup. Nasolabial fold prominence is usually the result of gravity-associated descent of the midfacial structures and may be better treated with resuspension of the midfacial fat pads or injection of soft tissue fillers into the folds. Although liposuction results may vary, its judicious use in the midface and for correction of the nasolabial folds may be helpful. The natural tendency for progressive atrophy of facial fat 7 , 10 , 21 makes midface liposuction risky, and liposuction performed above the mandible must be done conservatively, if at all. The thin skin in this location combined with overjudicious suctioning can cause obvious depressions and skin irregularities.
Additional considerations in facial sculpting include a family history of facial liposis in the midface and buccal area. Some parents and grandparents have full faces throughout life, and a buccal lipectomy may be indicated for the similarly shaped faces of their descendants. When buccal lipectomy is used in combination with cervicofacial liposuction, the results can be dramatic ( Fig. 18.6 ).

Furthermore, ideal candidates for primary liposuction of the cervicofacial region exhibit sufficient skin elasticity, which will promote skin contraction. In those patients with moderate or poor skin elasticity, removal of localized adiposity may predispose to an increased appearance of sagging skin. Dedo suggests that, after the age of 40 years, the contractile ability of skin may become unsatisfactory in this setting. 47 Others have suggested that age itself should not be the primary determinant in the efficacy of this procedure, but rather, that one should rely on actual tissue assessment as the predictive factor. 19 , 47 Occasionally, a young patient with apparently good skin elasticity may have limited results. Again, patients should be aware that good results are not entirely predictable when based only on the characteristics of skin elasticity and underlying structure.
Methodology and Physiology
There are several different methods to accomplish the primary goal of cervicofacial lipocontouring. When considering liposuction of the face and neck, the surgeon must be cognizant of the thinness of the facial skin, the proximity of sensory and motor nerves, the depth of fat to be aspirated, and the natural effects of aging on facial fat deposits.
Liposuction as it is used today was introduced in the 1970s and makes use of a rigid cannula attached to a suction device. 2 , 3
The cannula is rapidly advanced and withdrawn through the fatty deposits via subcutaneous tunnels. Fat cells are sharply avulsed by being drawn into the perforated cannula by the negative pressure created by the suction device. If the suction pressure is high enough, the fat cells are actually lysed and destroyed.
The addition of tumescence—the technique of using a large volume of infusate or wetting solution (usually an isotonic solution with a dilute mixture of lidocaine and epinephrine) to produce tissue turgor—to the liposuction regimen is widely used for body contouring and improved the safety and efficiency of liposuction after its initial description by Klein in the late 1980s. 48 Tumescence may be used in the head and neck in smaller volumes not only for fat aspiration, but also for tissue plane dissection. Despite these purported benefits, however, in the face and neck, tumescence may produce tissue distortion and make the end point more difficult to discern. 49 , 50 , 51
An alternative means to achieve lipectomy in the face and neck is the liposhaver, and its use warrants brief mention. Gross and Becker 52 , 53 advocate the liposhaver for direct lipectomy or for use in a closed technique in the cervicofacial area. The liposhaver is a guarded, motorized blade that removes fat via sharp excision either under direct vision or under a subdermal flap. Trauma is reportedly less than with standard techniques because of the excision versus avulsion principle. The shaver differs from the traditional, the tumescent, and the assisted liposuction techniques in that it does not require high suction pressures, and that it actively excises rather than avulses the fatty deposit. 52 , 53 Multi-institutional comparison trials 53 have shown success of the device and offer it simply as an alternative to conventional liposuction with the potential for less postoperative bruising, and in experienced hands, precise lipolysis. Despite its initial promise, there have not been additional reports or assessment of longterm outcomes using the liposhaver in the literature in the last 10 to 15 years.
The continued demand for improved results in liposuction procedures with low morbidity and downtime has led to the incorporation of energy sources, such as ultrasound, laser, and RF, to augment traditional treatment regimens. While useful under certain conditions, these newer technologies can have significant additional financial costs. Ultrasound energy can be applied via internal or external treatment of the fatty deposit, for fat cell disruption and facilitated aspiration. Studies documenting the use of ultrasound-assisted body lipocontouring reveal that the treatment of areas with a high fibrous content 49 is facilitated with the use of an internal or external ultrasound device. Additional reported benefits include liposuction that is less strenuous for the surgeon and more efficient for fat aspiration. 50 , 51 , 54 , 55 Further study of the use of body liposuction with ultrasound assistance reported less swelling and bruising postoperatively. 56
As ultrasound-assisted techniques have gained more widespread acceptance, refinements in their technical utilization have been made with progressive generations of these devices for safer and more efficient lipoaspiration. First-generation techniques delivered continuous ultrasound energy through large solid probes, yet did not allow simultaneous aspiration. Second-generation devices (e.g., LySonix [Mentor]) allowed simultaneous fat fragmentation and aspiration. Due to the small lumen (2 mm) of the hollow cannula in this device, however, aspiration was found to be largely inefficient, in some cases requiring posttreatment aspiration with a standard microcannula (Tulip [Tulip Biomed]). 57 , 58 Despite the initial enthusiasm for first- and second-generation ultrasound devices, it was nonetheless felt that the available techniques required excessive amounts of energy to achieve the desired effect. Additionally, it was felt that by using these devices, there may be an increased risk of burns and seroma formation due to thermal and cavitary effects, respectively. 57 Additionally, some authors feel that a hollow cannula that aims to concurrently apply ultrasound energy while aspirating can lead to inadvertent blunt trauma injury to neural, vascular, and lymphatic structures. 59
This prompted further advancements leading to the development of thirdgeneration appliances such as the VASER device (Sound Surgical Technologies). VASER, or vibration amplification of sound energy at resonance, uses pulsed, low-power ultrasound and high-efficiency, small-diameter solid titanium probes with grooves near the tip to increase fragmentation efficiency. This grooved design comes in a 2.9- and 3.7-mm cannula, and allows for effective fragmentation and aspiration at lower power settings. The reduction in energy required to achieve the desired effect is due to the grooved design that redistributes some of the applied energy to an area just proximal to the tip. Since ultrasound power delivered to the tissues is largely a function of probe diameter, the smaller cannula leads to an approximately 50% reduction in the energy required to achieve the desired effect. Moreover, the pulsed mode of the VASER device allows shorter treatment durations without a loss of efficiency, which also contributes to the reduced energy that is required to effectively fragment the adipose tissue. 59 Di Giussepe and Commons have reported good results with limited complications when using the VASER device for face and neck remodeling. 60
From a physiologic standpoint, when ultrasound energy is applied to tissues, this energy is transformed into mechanical vibrations that create a “micromechanical effect, a cavitational effect (expansion and compression cycles form microcavities in adipose tissue, which then implode, resulting in cellular destruction; that is, liquefaction of fat), and a thermal effect on fat cells.” 51 Grippaudo et al 61 utilized gas chromatography to confirm that ultrasound energy disrupts the adipocyte membrane, resulting in an egress of cellular contents without mechanical or enzymatic damage to triglyceride molecules.
Despite the purported benefits of ultrasound-assisted liposuction, numerous studies have shown potential problems with the use of subcutaneous ultrasound energy. These include excessive heat generation by the ultrasound device at the skin incision site 10 , 51 , 61 , 62 and potential heat-related complications at more distant subdermal sites. 37 , 63 Additionally, due to the proximity of neurovascular structures in the face and neck, caution is warranted as an animal-based study performed by Howard et al revealed the potential for neural injury with direct application of ultrasound energy at a higher amplitude. 54 Furthermore, it is thought that the cavitational effect produced by the applied ultrasound energy can lead to demyelination due to the high lipid content of myelin. 64 Despite these reports, ultrasound-assisted liposuction has been used for treatment of the face and neck without any reports of permanent neural injury. 58 , 65
Laser-assisted liposuction is another technique that has been described to facilitate and augment traditional SAL. Early adoption has taken place primarily in the arena of body contouring, although some reports have detailed its use in the face and neck. 66 , 67 , 68 Laser-assisted liposuction functions on the principle of selective photothermolysis and its incorporation into traditional liposuction techniques aims to facilitate aspiration, reduce operative blood loss due to selective coagulation of vessels, and provide tightening of the overlying skin envelope via effects on collagen. These effects are achieved by using lasers in the near infrared spectrum to selectively target water molecules within adipose and dermal tissue, and intravascular hemoglobin molecules to achieve coagulation. 69 The 980 nm diode, 1064 nm Nd:YAG (which has been used and studied most extensively for this purpose), and 1064/1320 nm Nd:YAG (which aims to take advantage of selective tissue absorption characteristics by employing the two wavelengths concurrently) are the three most commonly used lasers for laserassisted liposuction. 70 , 71 Histologic analysis following the application of a 1064 nm Nd:YAG laser revealed rupture of the adipocyte membrane, channel formation at the site of treatment, and collagen coagulation. 66 Although the above findings highlight the potential uses for this technology, some authors feel that laserassisted liposuction has only a limited role in facial liposuction with limited benefits and has a significant learning curve during its initial utilization. 60 , 72
Application of RF energy and RF-assisted liposuction are additional emerging technologies that take advantage of a tissue’s inherent characteristics to facilitate liposuction and achieve concomitant tissue tightening. A tissue’s native impedance, or resistance to electrical activity, is what allows the selective heating of tissues and subsequent tissue tightening via collagen denaturation. 73 Adipose tissue is ideally suited to treatment with RF devices as it has relatively high tissue impedance, thereby allowing the generation of large amounts of heat for treatment purposes. In addition, adipocytes have a low heat transfer coefficient, limiting the amount of unwanted energy transfer to adjacent structures. 74 These principles have been expanded to the use of RF energy as an adjunct to lipoaspiration. The application of RF energy via an internal electrode dissolves adipocytes while also triggering collagen contraction and neocollagenesis. 75 Early reports in body lipocontouring have shown favorable results using this technique 72 , 75 , 76 ; however, no formal reports of RF-assisted cervicofacial liposuction exist at the time of this writing.
In addition to energy-assisted liposuction techniques, a number of noninvasive techniques can be used to enhance the results of SAL. An extension of the above RF techniques is the ThermaCool device (Thermage Inc.), which applies transcutaneous RF energy via a monopolar RF probe and has shown good improvements in addressing cheek and neck laxity. 77 Similarly, ThermiRF (Thermitight [ThermiAesthetics]) can be used as an adjunctive or alternative technique to formal cervicofacial liposuction. This device delivers RF energy in a subdermal location via small entry incisions, thereby tightening the skin via the aforementioned mechanisms associated with tissue response to RF application. Cool sculpting is another means of achieving lipocontouring and tissue tightening using the concept of cryolipolysis, or selective reduction of adipocytes after controlled exposure to cooling to induce apoptosis. This technique has primarily been used to refine the results of body sculpting and contouring, and no reports have emerged regarding its use in the face and neck. 78 Finally, intense focused ultrasound (Ulthera Inc.) is a technique that uses short, millisecond pulses with a frequency in the MHz domain to achieve tissue tightening by tissue absorption of acoustic energy and has shown good results in improving laxity of the lower face and neck. 73 , 79
This technology, also known as intensity-focused ultrasound or microfocused ultrasound, utilizes dual-function transducers that use lower energy ultrasound for tissue visualization while also providing higher ultrasound energies for tissue treatment and induction of thermal injury. It has been shown to be effective in achieving tissue tightening in the face and neck with minimal downtime and no reported severe longterm complications. 80 This intensely focused ultrasound energy causes intermolecular friction with resultant release of thermal energy causing a coagulative necrosis and subsequent tissue tightening. 80 This occurs at a defined depth without injuring the more superficial epidermis. These thermal-injury zones can be reliably controlled based on the use of tissue probes leading to neocollagenesis and reorientation/remodeling of collagen and elastin fibers in the reticular dermis. 80 While multiple reports confirm that moderate improvement can be seen with Ulthera when used for this purpose in the face and neck, 81 , 82 , 83 , 84 appropriate patient selection is a critical factor in obtaining good outcomes. Patients with significant photoaging, liposis, and laxity of the face and neck may be better served by alternative, more formal surgical means. 84 Thinner patients with mild tissue laxity and lipoptosis of the face and neck, however, are more suited to this noninvasive treatment modality, although expectations should be managed at the time of the preoperative evaluation with thorough counseling by the treating surgeon. 84
Lastly, another method of addressing submental fullness in a nonsurgical manner has recently gained FDA approval. 85 Kybella (Kythera Biopharmaceuticals), or injectable deoxycholic acid (ATX101), has been shown to be efficacious in reducing submental fullness in a number of clinical trials. 86 , 87 , 88 Deoxycholic acid is a natural bile salt and detergent that reduces subcutaneous fat stores. Kybella injection causes induction of pores in the cellular membrane with resultant cytoplasmic leakage and subsequent adipocyte lysis. 89 An influx of inflammatory cells and fibrosis follows adipocytolysis and this is thought to cause the clinical effect seen in the form of a reduction in submental fullness and tissue tightening. 87 This treatment is carried out using a number of injections (up to 0.2 ml per injection) spaced approximately 1 cm apart in the submental region. 86 While its clinical use is approved by the FDA, frequent adverse effects, including erythema, edema, and bruising at the injection site were reported. Moreover, dysphagia, temporary weakness of the marginal mandibular nerve, and skin ulceration/necrosis were reported following Kybella injection. As a result, the depth and location of injection were cited as critical safety factors associated with this treatment. 86
Related posts:






Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


