17 Limb-Threatening Emergencies
17.1 Fasciotomy for Acute Compartment Syndrome
Compartment syndrome is an emergency that if not dealt in time can lead to limb dysfunction and loss. The surgeon should be guided clinically and should not waste time on investigations particularly when signs of compartment syndrome are present. The warm ischemia time for muscle is 6 hours and therefore emergent forearm fasciotomy should be rapidly performed.
The limb in these patients is often tense; there is severe unrelenting pain which cannot be controlled with opiates. Pain is worsened by passive extension. Late signs include diminished pulses.
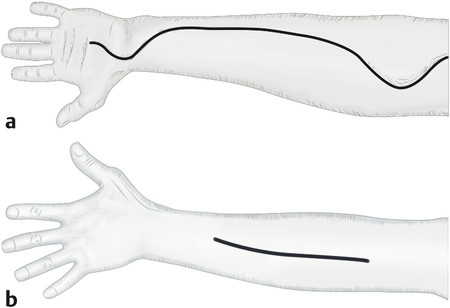
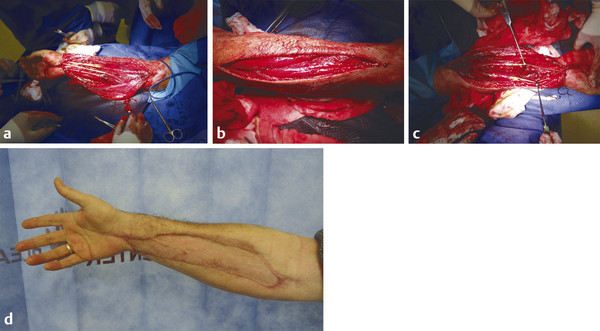
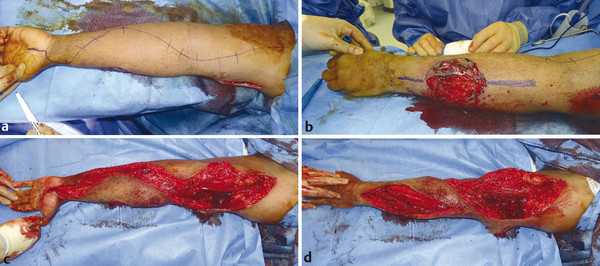
Surgery involves a long curvilinear incision over the flexor forearm and a straight line incision over dorsal extensor compartment. The carpal tunnel is first released, a U-shaped flap is placed over the wrist and this is to protect the median nerve from exposure. The incision should release the deep and superficial compartments of the arm. The flexor pollicis longus (FPL) compartment is often the most affected. The mobile wad (brachioradialis, extensor carpi radialis brevis [ECRB], and extensor carpi radialis longus [ECRL]) should also be released. Once the patient is stabilized, the wound can be skin grafted with vacuum-assisted closure (VAC). If caught in time, patients can make a full recovery with good long-term outcome (Fig. 17‑1, Fig. 17‑2, Fig. 17‑3).
17.2 Hand Compartment Release
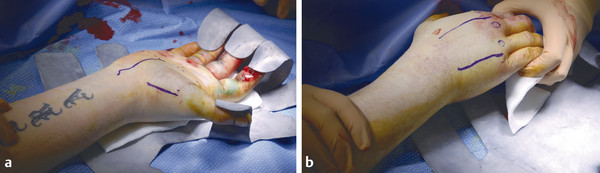
This may be necessary in severe crush injuries to the hand: high-pressure injection injuries, reperfusion injuries after replantation, and in circumferential hand burns. The hand has 10 compartments in total and all must be released to prevent muscle necrosis.
The compartments include hypothenar, thenar, adductor pollicis, the four dorsal interosseous muscles, and three volar interosseous muscles. The carpal tunnel must also be released (Fig. 17‑4, Fig. 17‑5, Fig. 17‑6, Fig. 17‑7, Fig. 17‑8, Fig. 17‑9).




Related posts:






Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


