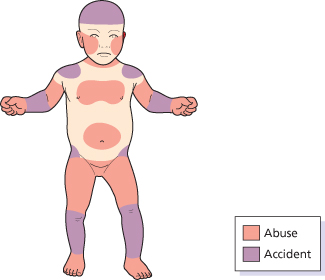
Fig. 154.3 Anatomical sites of abusive and accidental bruising.
Reproduced from Kos & Shwayder 2006 [15] with permission from Wiley-Blackwell.
Patterned bruising is a strong indicator of abuse and may occur together with lacerations and abrasions. A variety of instruments may be used to inflict injury on a child and cause different types of bruising.
Loop marks are curvilinear marks produced by small ropes, cords or electrical belts which appear randomly over the body as a result of the striking of a struggling child.
Buckles from belts leave a characteristic imprint that can often be matched to the buckle used. Buckles inflict deep ecchymotic injury and can result in injury of the underlying organs and bones.
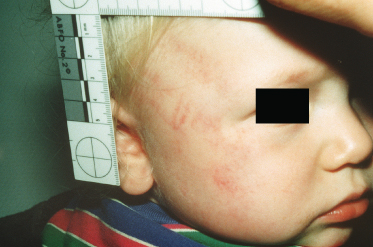
When a child is slapped, blood is forced laterally by the fingers, extravasating and leaving an outline of the fingers while the actual point of impact is white.
Pinch marks, particularly on the ears or in the genital region of male children, should alert the examining physician as male toddlers rarely sustain bruises on the genitalia secondary to a fall.
Blunt trauma can be a very severe form of abuse that may result in cutaneous lesions. If abdominal bruising is noted, the physician must also look for associated internal injury. In the form of slapping injury, it often leaves the imprint of the perpetrator’s hand across the child’s skin. Capillaries break between the fingers, producing linear bruises outlining the blunt object.
Binding injuries (Fig. 154.4) are more likely when the perpetrator is emotionally disturbed or psychotic. Acute binding injuries cause oedema of the soft tissue around the wrists and ankles that may resemble rope burns with redness and warmth or abrasions. This type of injury can also result in distal petechiae and oedema. Chronic binding injuries can cause bands of hyperpigmentation.

The colour of a bruise is influenced by various factors such as time and depth of injury, the body surface involved, the skin colour, vascularity of the underlying tissue, child’s age and gender and medications that affect the rate of ecchymosis dispersion. Dark skin may mask bruises. A fresh bruise generally appears blue or red-purple, but red can be present in bruises whatever their age. A bruise is older if it is yellow, green or brown. Bruises of different colours on the same body surface are mostly not compatible with a single event.
A study by Bariciak et al. [11] showed that physicians are unable to accurately determine the age of bruises. The examiner must be very cautious in making estimates as the appearance of a bruise depends not only on its age, but also its site and depth as well as the complexion of the skin. Woods’ lamp illumination has been reported to have an application in identifying bruises that are faint or not visible to the naked eye.
Box 154.6 Conditions Commonly Mistaken for Inflicted Bruising [12]
- Mongolian spots
- Capillary haemangioma
- Lymphangioma
- Ink, dye or paint stains
- Eczema
- Phytophotodermatitis
- Coagulation disorders
- Hypersensitivity reactions
- Purpura fulminans or meningococcaemia
- Incontinentia pigmenti
- Impetigo
- Café-au-lait spots
- Chilblain
- Osteogenesis imperfecta
- Ehlers–Danlos syndrome
Bite Marks
All bite marks should raise suspicion of abuse and lead to full examination of the skin. A classic bite mark is circular or oval (Fig. 154.5). Human bite marks may serve to identify the abuser. They typically have a central area of ecchymosis with either of the following patterns:
- positive pressure from the closing of teeth with disruption of small vessels
- negative pressure caused by suction, creating surrounding erythema and oedema with occasional petechiae.
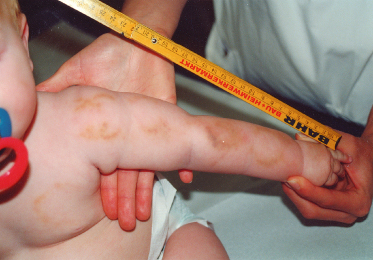
The canines leave the deepest and most prominent marks. The normal distance between the maxillary canine teeth in adults is 2.5–4.0 cm, so bites with an intercanine distance greater than 3 cm are likely to be adult bites. A forensic odontologist can differentiate an adult bite from that of a child by the pattern of teeth and can also make impression models of the suspected perpetrator’s teeth and thus help to identify the individual [13].
Human bite marks differ from animal bite marks in that they produce a crushing type of injury, whereas typical animal bite marks result in puncture of the skin.
Bite marks may be visualized more clearly 2–3 days after the injury because of the decreased oedema and surrounding erythema. As a result, sequential examinations and photographs should be obtained for evaluation. Bite marks should be photographed with and without a ruler and without distortion.
For DNA testing, prior to any cleansing, all fresh bite marks should be swabbed with a sterile cotton swab moistened with sterile saline, which is then dried, placed in an envelope and sent to a forensic laboratory for analysis. A second swab should be obtained as a control from an unharmed area of the child’s skin.
Burns
Burns comprise approximately 5–22% of physical abuse. Burn abuse seems to be more common in children <3 years of age and accounts for 8–25% of all paediatric burns [14,15]. When compared with accidentally burned children, abused children were significantly younger, had longer hospital stays and a higher rate of mortality [16].
Burns can be electrical, chemical, thermal or radiant. The degree of local heat damage depends on the contact temperature, the duration of exposure and the affected skin region. In contact burns, further parameters of burn severity are whether they are caused by a metallic or non-metallic hot object and moist or dry heat, which is apparent from the coefficient of thermal conductivity. Dry heat requires an essentially longer exposure time than moist heat to cause a burn of comparable intensity at the same temperature [17]. Chemical burns are either acidic or alkaline, and cause a prolonged period of burning because of the residual product on the skin. Alkaline burns result in liquefaction and deeper injury.
Thermal injury may follow accidents or carelessness, or be due to negligent or inadequate parenting. Burns may be deliberately inflicted by exposure to hot liquids or other hot object and constitute an especially traumatic form of injury to children.
A delay between injury and seeking medical care of more than 2 hours often occurs with inflicted burns and should always raise suspicion for abuse.
Box 154.7 Features Suggestive of Abuse in Burn Injuries [12]
- Burns that look older than the history would suggest
- The existence of other injuries
- Symmetrically distributed burns
- Burns localized to the perineum/buttocks
- Burns suggestive of immersion: no splash marks, clear tide levels, stocking- or glove-pattern burn
- Wounds necessitating skin grafting or intensive care
- Sparing of flexor creases
- Burns of posterior head or back
- Multiple burn sites
- Burns consistent with the following mechanisms of injury: brands/contact burns, cigarette burns, scalding immersion, microwave oven, stun guns, fork tines, light bulb, iron or grill markings
The shape of a burn may be diagnostic when it reflects the pattern of an object or the method of injury. Burn abuse includes scalds, pattern burns due to contact with various household appliances, flame burns, cigarette burns and electrical/chemical burns.
Scalds are the most frequent form of burn abuse, with more than 80% resulting from tap water. They are typically divided into immersion and splash/spill burns. Forced immersion burns tend to be symmetrical and have clear lines of demarcation, often called ‘tide marks’ [18]. They usually have a uniform burn depth and commonly involve the buttocks, perineum and lower extremities (Figs 154.6, 154.7).

Fig. 154.7 Dunking scald injury of the foot of a newborn.
Courtesy of Dr J.P. Sperhake, Hamburg, Germany.

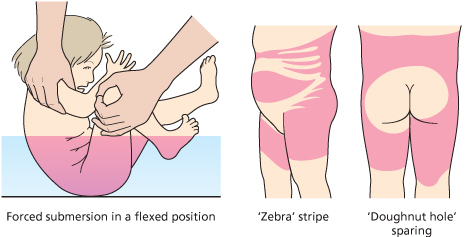
Dunking scald injuries occur most often in infants and toddlers. Scalds on the buttocks may be associated with attempts to toilet train an infant. ‘Doughnut-type sparing’ may occur on the child’s buttocks when the buttocks are held against a cooler tub or basin while the surrounding hot water scalds the remaining immersed skin. Dunking scalds of the extremities leave a characteristic ‘stocking and glove’ distribution with a very sharp demarcation of the burn. ‘Zebra stripes’ are due to sparing of the flexural creases secondary to the body’s flexed position in the hot liquid (Fig. 154.8).
Fig. 154.8 Patterns of forced submersion.
Reproduced from Kos & Shwayder 2006 [15] with permission from Wiley-Blackwell.
In contrast to all this, accidental immersion burns, where a child falls into hot liquid, typically have irregular borders and non-uniform depth as the patient is struggling to escape. Accidental burns are also rarely full thickness as they typically involve shorter contact times.
In conclusion, simultaneous scald burns to buttocks, feet and perineum are highly suspicious for physical abuse, as are well-demarcated burns around the buttocks or bilateral symmetrical glove and stocking burns [15].
Splash and spill burns are scalds resulting from a hot liquid which is thrown at or poured over a child. They often occur accidentally, they are generally more superficial than immersion burns and associated splash marks are more frequently seen than in immersion burns. Distinguishing between accident and abuse in this form of burn can be very difficult.
Branding injuries take the shape of the heated object. Accidental contact burns are often patchy and superficial as the child quickly withdraws from the hot object. Inflicted contact burns are deeper, may be multiple, have well-demarcated margins and are often located on typically protected sites of the body. They are commonly due to hot irons, radiators, hair dryers, curling irons and stoves. Hand burns can also be seen in accidents, but then the more common site is the palm and the anterior surface of the fingers, which would be in contact with the hot object while the child is grasping it. In abuse, the dorsum of the hand is commonly involved.
Cigarette burns represent a frequent form of thermal injury. They appear as 7–10 mm round, well-demarcated burns that have a deep central crater and heal with scarring.
Cigarette burns inflicted with the intention of maltreatment are mostly located in regions typical of abuse, e.g. on the back of and the palms of the hands (Fig. 154.9), the soles, the genitals, the neck, shoulders, back and buttocks, the forehead and the chest. A multitude of cigarette burns and an arrangement in geometric patterns are particularly suspect. Accidental dropping of a cigarette onto a child or a child brushing against a lighted cigarette will cause only a very slight superficial burn because of the short duration of exposure and the minor intensity of the contact [19,20].

Stun guns
Related posts:






Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


