Stage 2.
The so-called verrucous lesions were observed in just over one-third of the 111 patients reported by Landy & Donnai [11]. These lesions were often short-lived and trivial compared with the initial vesicular eruption and therefore might have been under-reported. In the patients in whom there was a positive history, the lesions had appeared by 2 months and all had cleared by 3 years. The lesions were predominantly seen on the distal limbs, especially the digits and ankles (Fig. 130.2). They did not necessarily appear in the same areas as the vesicles. The crusting lesions that develop at the vertex following blistering at that site may be similar to the verrucous lesions but these tended to persist and to be followed by an area of alopecia.

Stage 3.
This is the stage that gives its name to the condition but its presence and extent are very variable. It can range from small streaks of pigmentation in the groin (Fig. 130.3) to more extensive lesions, especially following Blaschko’s lines around the trunk (Fig. 130.4). The nipples are frequently involved in the increased pigmentation and the axillae and groins are invariably affected in patients with pigmentation elsewhere. The pigmentation has usually appeared by 6 months but, occasionally, not until 2–3 years. By 10 years, the lesions have faded in about 25% of cases and the majority of pigmented lesions disappear by the age of 16 years.

Fig. 130.4 Female, aged 4 years, demonstrating widespread pigmentation in the distribution of Blaschko’s lines.

Stage 4.
This is the so-called atrophic phase classically seen in affected adult females. However, in the series of Landy & Donnai [11], these pale linear lesions were observed in many girls under the age of 10 years, concurrent with hyperpigmented or even vesicular and verrucous lesions. The atrophic lesions are less frequently observed on the trunk and are more often seen on the posterior aspect of the upper and lower legs (Fig. 130.5) and over the shoulders and upper arms.
Fig. 130.5 Adult female demonstrating so-called atrophic phase of IP in a linear lesion over right calf.

Nails
Nail dystrophy is frequent, occurring in approximately 40% of affected individuals. The range of manifestations is wide, from mild ridging or pitting to severe nail dystrophy resembling onychomycosis. Nail dystrophy may be a transient phenomenon. The child whose nails are illustrated in Figure 130.6 was affected for approximately 6 months before complete resolution. Subungual keratotic lesions have been described [32–34]. The histology of these lesions corresponds to that seen in the verrucous cutaneous lesions of stage 2, showing hyperkeratosis, acanthosis, papillomatosis and focal dermal dyskeratosis.

Hair
Although hair abnormalities are common, it is rare for affected females to have major cosmetic problems. Alopecia, especially at the vertex and usually after blistering or verrucous lesions at this site, is common. Hair is often described as sparse early in childhood and later in life as lustreless, wiry and coarse. Wiklund [35] described the hair in later life as ‘woolly hair naevus’.
Teeth
Dental abnormalities are common, occurring in over 80% of cases. Either, or both, deciduous and permanent dentition may be affected and abnormalities include hypodontia, delayed eruption, impaction and malformation of the crowns, especially conical forms and accessory cusps [33]. Deciduous teeth may be retained into adult life (Fig. 130.7). Dental features can be of diagnostic value in adult females and, if present in adult first-degree female relatives of an affected case, they should stimulate a search for other signs such as atrophic skin lesions or hair anomalies.

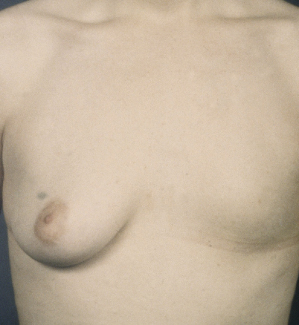
Breasts
Breast anomalies have rarely been reported in patients with IP but in the series of Landy & Donnai [11], breast anomalies occurred in 10% of cases. One woman had unilateral breast and nipple aplasia (Fig. 130.8) whereas 10 others had supernumerary nipples.
Fig. 130.8 Same adult female as in Fig. 130.7 demonstrating unilateral aplasia of breast and nipple.
Eyes
Related posts:






Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


