13 The Use of Autologous Grafts in Ophthalmic Plastic Surgery
Abstract
“The Use of Autologous Grafts in Ophthalmic Plastic Surgery” discusses the use of the patient’s own tissue in ophthalmic plastic surgery, where it has widespread application. By contrast, homologous material such as donor sclera, although very convenient to use, is no longer acceptable to most patients because of the small risk of transmissible disease. For this reason, the use of homologous material should be avoided if possible. If the surgeon feels it is in the best interests of the patient to use homologous material, the risks must be explained to the patient and fully informed consent obtained for its use. Autologous grafts in ophthalmic plastic surgery include full-thickness skin grafts (taken from the upper eyelid, postauricular area, preauricular area, upper inner arm, or supraclavicular fossa), split-thickness skin grafts (taken from the thigh), mucous membrane grafts (taken from the lower lip, upper lip, or buccal mucosa), hard palate mucous membrane grafts (more rigid than lip or buccal mucosa but rougher), upper eyelid tarsal grafts, auricular cartilage and nasal septal cartilage grafts, dermis fat grafts, structural fat and fat pearl grafts, fascia lata and temporalis fascia grafts, eyelid composite grafts, and bone grafts.
13.1 Introduction
Autogenous grafts have widespread application in ophthalmic plastic surgery. By contrast, homologous material such as donor sclera, although very convenient to use, is no longer acceptable to most patients because of the small risk of transmissible disease. For this reason, the use of homologous material should be avoided if possible. If the surgeon feels it is in the best interests of the patient to use homologous material, the risks must be explained to the patient and fully informed consent obtained for its use.
13.2 Skin Grafts
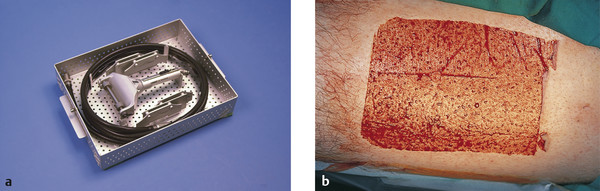
Skin grafts may be full-thickness or split-thickness grafts. A split-thickness skin graft contains only a portion of the dermis, and the graft is harvested using a dermatome (Fig. 13‑1), the thickness of the graft being varied by adjustments made on the device. By contrast, a full-thickness skin graft is harvested free hand using a surgical blade. Split-thickness skin grafts contract and have a poor color match with adjacent skin. Full-thickness skin grafts show less of a tendency to contract and are much more commonly used in ophthalmic plastic surgery.
13.2.1 Indications
Full-Thickness Skin Graft
Repair of cicatricial ectropion.
Eyelid or facial reconstruction.
Scar revision surgery.
Partial-Thickness Skin Graft
Reconstruction of the exenterated socket.
Skin coverage of large facial skin defects (Fig. 13‑2).
13.2.2 Full-Thickness Skin Graft
There are a number of potential donor sites for full-thickness skin grafts:
Upper eyelid.
Postauricular area.
Preauricular area.
Upper inner arm.
Supraclavicular fossa.
The choice of donor site is influenced by a number of factors, including the patient’s age, the size of graft required, and the degree of solar damage of the donor skin.
The upper eyelid skin is easy to harvest, provides an ideal color and texture match for eyelid defects, and has no subcutaneous fat. This site does not yield much skin, however, except in older patients with marked dermatochalasis. Removing too much skin may cause lagophthalmos and may exacerbate a brow ptosis. It may also leave the patient with an asymmetrical appearance. The skin above the skin crease is removed in a similar fashion to a blepharoplasty, marking the skin to be removed very carefully to ensure that the patient can still close the eyelids passively and that a minimum of 12 mm of skin is left between the uppermost skin marking and the lowermost part of the eyebrow.
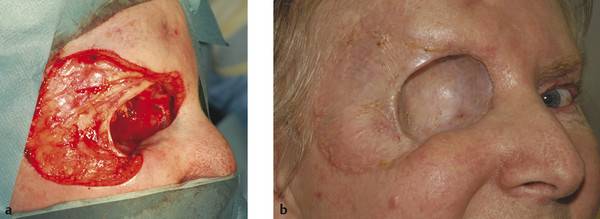
Postauricular skin provides a relatively good color and texture match for eyelid and canthal defects. Its use may be precluded by solar damage in older patients or the use of a hearing aid. The skin to be removed is shared between the ear and the scalp in the mastoid area. The removal of large grafts can draw the ear closer to the skull. Preauricular skin is more readily accessible but may not yield sufficient skin for large defects. It is also a poor site to use in patients who have very greasy skin with prominent sebaceous glands. Such skin is more prone to contracture and a “pin cushion” effect (Fig. 13‑3), particularly when used for medial canthal defects.

Surgical Procedure
Meticulous attention to detail is required to obtain a good result from a skin graft without complications (Video 13.1).
The recipient bed must be prepared carefully and all bleeding stopped. The defect should be exaggerated in the eyelids by placing traction sutures through the gray line and placing the eyelid on traction. Tightening the lower eyelid, such as with a lateral tarsal strip procedure, is often necessary before placing a skin graft, particularly if there is any significant eyelid laxity or where the graft occupies more than half of the eyelid. Failure to tighten the eyelid may result in a lower lid ectropion postoperatively as the graft contracts.
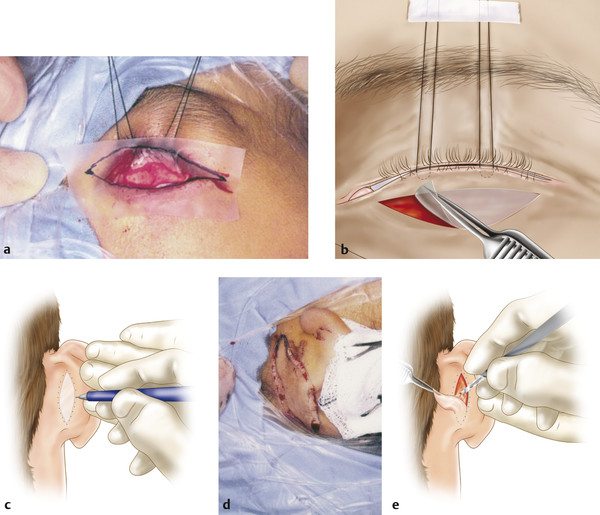
A piece of Steri-Drape is placed over the defect and outlined with a marker pen (Fig. 13‑4a,b). This is cut to the exact size and shape of the defect and used as a template.
The template is then transferred to the donor site, where it is outlined with the marker pen (Fig. 13‑4c–e).
The donor site is then injected subcutaneously with 0.5% bupivacaine with 1:200,000 units of adrenaline.
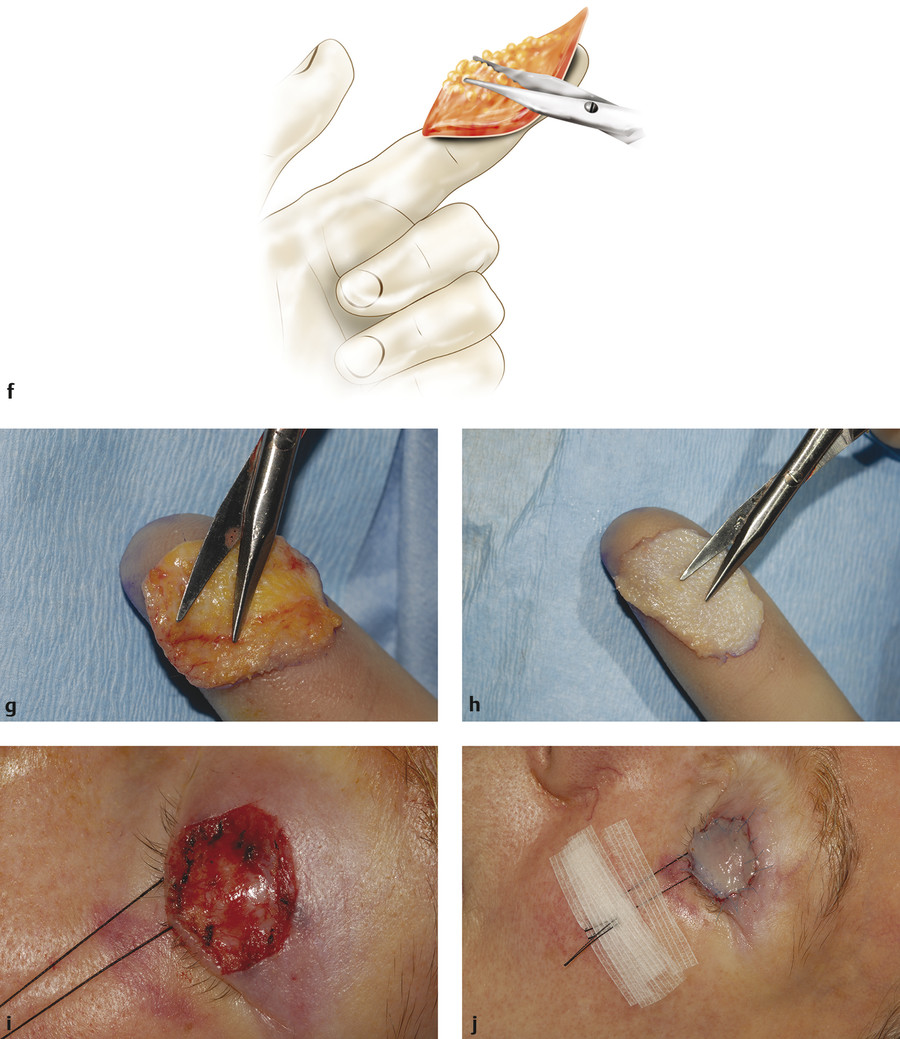
The marked line is incised with a no. 15 scalpel blade and the graft removed using forceps and the scalpel blade (Fig. 13‑4f–h). The skin should be held under tension as the blade is used to stroke across the skin, maintaining a constant depth that should be as shallow as possible; alternatively, Westcott scissors may be used. The defect may need to be converted to an ellipse to effect adequate closure of the wound or to the typical shape of a blepharoplasty incision when the upper eyelid is used.
The graft is protected in a gauze swab moistened with saline. This must be stored carefully to avoid inadvertent loss of the graft.
The donor site is closed with a 4–0 nylon suture, either as a continuous simple or blanket suture when the preauricular or postauricular area is used as a donor site. An upper lid defect should be closed with interrupted 7–0 Vicryl sutures. An upper inner arm wound should be closed with interrupted subcutaneous 4–0 Vicryl sutures followed by interrupted 4–0 nylon sutures for the skin, with the skin sutures placed in a vertical mattress fashion. A supraclavicular fossa donor site wound can be closed with a subcuticular 6–0 Novafil suture or with interrupted 4–0 nylon sutures if the wound is under tension.
All subcutaneous tissue is completely removed with blunt-tipped Westcott scissors while holding the graft over the index finger of the nondominant hand (Fig. 13‑4f). It is important to spend time meticulously thinning the graft in this way until no more tissue can be removed. Large skin grafts are perforated at several points with the tip of the scalpel blade.
The graft is then placed on the recipient bed and four to six interrupted 6–0 silk sutures are placed if a bolster is to be applied. The sutures are passed from graft to recipient skin edge. Interrupted 7–0 Vicryl sutures are placed between the silk sutures. The graft should fit snugly into the recipient bed with a slight degree of tension(Fig. 13‑4i,j). If the patient is at risk of skin graft thickening, it is preferable to use 6–0 Novafil sutures.
A piece of sterile sponge is then cut to the size and shape of the graft using the original template. This is covered with petrolatum-coated gauze and placed onto the graft. The silk sutures are tied to each other over the sponge to act as a bolster (Fig. 13‑4k) if there is a risk of postoperative bleeding from the recipient bed. This prevents the accumulation of serous fluid or blood under the graft, which will act as a barrier to vascularization. This sponge can usually be omitted for most periocular skin grafts, which can be covered with a small folded sheet of Jelonet alone. An additional sheet is placed over this.
In the case of an eyelid skin graft, the gray line silk suture is left in place and used to keep the graft stretched and the globe protected. The skin of the cheek or forehead is treated with a small amount of tincture of benzoin applied with a swab to dry the skin. The silk suture is taped to the cheek in the case of an upper lid graft or to the forehead in the case of a lower lid graft using Steri-Strips.
A pressure dressing consisting of a sheet of Jelonet covering the orbital area and two eye pads are applied and taped into place with Micropore tape, and this is reinforced with a head bandage.
Postoperative Care
The bandage is removed by the patient after 48 hours, but the underlying dressing is maintained in place for 4 days. The dressing is then removed along with the silk bolster sutures if these have been used. The Vicryl or Novafil sutures are left in place and removed 8 to 10 days postoperatively, along with the donor site sutures.
Aftercare of the skin graft is very important. The patient should avoid sun exposure for a period of a few weeks to minimize color changes in the graft. Antibiotic ointment should be applied to the graft 2 to 3 times per day for 2 weeks and massage of the graft commenced after 2 weeks. Massage should be performed in several directions over the graft for a minimum period of 3 to 4 minutes three times per day. Massage prevents contracture and thickening of the graft and should be continued for 2 to 3 months. A preservative-free ophthalmic lubricant ointment is applied to the graft before massage. The application of a silicone gel such as Kelocote or Dermatix may also help to prevent contracture and thickening of the graft, but this adds expense. If the graft does thicken, it can be injected with tiny quantities of Triamcinolone (Kenalog) at several different sites in the graft. There is increasing anecdotal evidence that tiny doses of botulinum toxin injected in multiple locations in the graft can also reduce wound thickening by inhibiting fibroblast activity.
13.2.3 Split-Thickness Skin Graft
The usual donor site for a split-thickness skin graft is the thigh.
Surgical Procedure
The thigh is prepared with undiluted iodine solution and the area draped. The area is injected subcutaneously at several sites using 15 to 20 mL of 0.25% bupivacaine with 1:200,000 units of adrenaline.
A light coating of glycerine is applied to the thigh for lubrication.
The dermatome is prepared with a blade of an appropriate size and the desired thickness of the graft set on the dermatome (usually 1/16 inch). The dermatome is checked to ensure that it is working correctly.
The assistant places a small wooden board across the thigh in front of the dermatome to flatten the contour of the thigh (Fig. 13‑5a,b).
The dermatome is applied to the thigh at a shallow angle and slowly advanced while countertraction is applied to the skin of the thigh in the opposite direction.
An assistant holds the skin as it emerges from the dermatome. Once the desired amount of skin has been harvested, the dermatome is stopped and the skin attachment to the thigh is cut with Stevens tenotomy scissors.
The skin graft is then cut and shaped according to the defect and sutured into place as described for a full-thickness skin graft.
The patient should be prescribed appropriate postoperative analgesia to be administered as soon as the effects of the local anesthetic agent begin to wear off.
Most split-thickness skin grafts in oculoplastic surgery are used to line an exenterated socket (Fig. 13‑5c–e).
Such grafts are first placed in a skin graft mesher and enlarged 1:2 (Fig. 13‑5f).
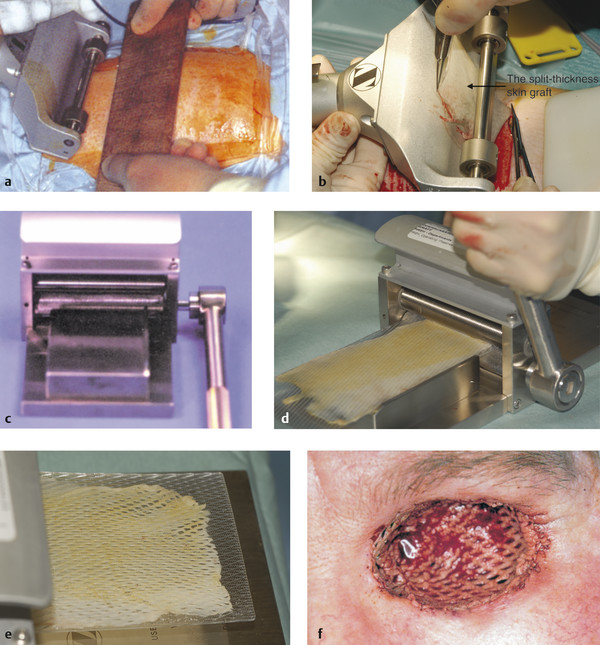
The mesher effectively enlarges the area of the graft, reducing the size of the donor site. It also ensures egress of serosanguinous fluid. Any remaining skin is returned to the donor site, which aids the rapid healing of the donor site.
Postoperative Care
The patient should be given adequate analgesia, because this procedure can be associated with considerable postoperative pain. The thigh wound is covered with an Allevyn Non-Adhesive (Smith and Nephew) foam dressing and attached using adhesive Opsite Flexifix (Smith and Nephew) transparent film covering. A piece of Gamgee (3M), a highly absorbent cotton roll padding with a nonwoven cover, and a bandage are also applied to aid hemostasis and to reduce the amount of exudate. This dressing should be changed if any exudate leaks from it. As the wound continues to heal, a less absorbent dressing may be considered, and an Allevyn Thin or Compression (Smith and Nephew) dressing can be used to protect the area from clothing and allow the wound to completely heal. Once healed the area should be then be massaged with petrolatum.
Postoperative care of the exenterated orbit is described in Chapter 24.
13.3 Mucous Membrane Graft
A mucous membrane graft can be removed free hand or with the aid of a mucotome. It is generally easier and safer to remove such a graft free hand.
There are a number of potential donor sites for mucous membrane grafts:
The lower lip.
The upper lip.
The buccal mucosa.
The lower lip is preferred. The access is easier and no sutures are required to close the wound, which epithelializes spontaneously over the course of 2 to 3 weeks. The buccal mucosa yields more graft material but normally has to be sutured and is not as accessible. Great care must be taken to avoid damage to the parotid duct, whose opening is opposite the upper second molar tooth, when harvesting a buccal graft.
13.3.1 Indications
Conjunctival replacement after an enucleation.
Fornix reconstruction in an anophthalmic socket.
Severe upper eyelid entropion.
Symblepharon division and reconstruction.
Any patient who is to undergo an enucleation and who has conjunctival scarring from previous surgery or trauma may require a mucous membrane graft. The patient should be counseled about this possibility before surgery and the anesthetist should be informed. The anesthetist should place a throat pack after induction of anesthesia and should place the endotracheal tube to one side of the mouth. The donor site is injected with 0.5% bupivacaine with 1:200,000 units of adrenaline before the patient is prepared and draped for surgery.
Surgical Procedure
The recipient bed must be prepared carefully and all bleeding stopped.
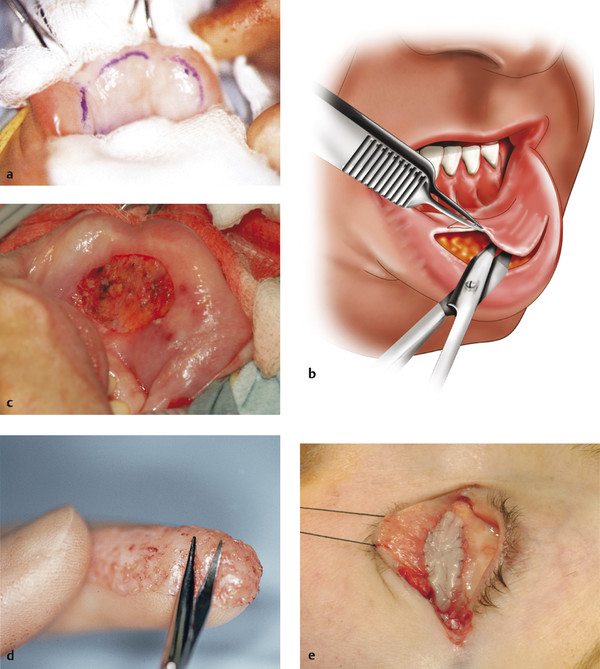
A piece of Steri-Drape is placed over the defect and outlined with a marker pen. This is cut to the exact size and shape of the defect and used as a template much in the same way as for a full-thickness skin graft.
Two Babcock’s bowel clamps are placed over the edge of the lower lip, which is protected with gauze swabs moistened with saline.
The vermilion border of the lip is included in the clamps, ensuring that this area cannot be included in the area used to harvest the graft.
The template is then transferred to the donor site, where it is outlined with the marker pen after the mucosa has been dried with a dry swab.
The donor site is then injected with saline (Fig. 13‑6a). This is repeated at intervals, because it aids the dissection of the graft.
The marked incision line is gently incised with a no. 15 scalpel blade and the graft removed very carefully using blunt-tipped Westcott scissors and small-toothed forceps (Fig. 13‑6b,c). The Westcott scissors should be kept just under the surface of the graft with the edge of the graft drawn horizontally to ensure that the graft is not inadvertently perforated and that the dissection is not taken too deep. Dissection in a deeper plane risks leaving areas of the lip with sensory loss. Alternatively, a mucotome may be used.
The graft is protected with a gauze swab moistened with saline. This must be stored carefully to avoid inadvertent loss of the graft.
A swab gently moistened with 1:1000 units of adrenaline is held over the donor site for 5 minutes, and any bleeding vessels are cauterized using bipolar cautery.
The graft is carefully thinned with Westcott scissors, removing any fibrofatty tissue while holding the graft over the index finger of the nondominant hand (Fig. 13‑6d).
The graft is then placed, ensuring that the original graft surface faces upward, on the recipient bed, and interrupted 7–0 Vicryl sutures are placed from the graft edge to the recipient conjunctival edge (Fig. 13‑6e).
The graft must be maintained in position with the use of a symblepharon ring when the graft is placed onto the globe or with a conformer of an appropriate size and shape when the graft is placed centrally in an anophthalmic socket. If the graft is used to reconstruct a conjunctival fornix it should be held in place with a 240 silicone retinal band and 4–0 nylon fornix-deepening sutures (see Chapter 22).
Postoperative Care
The patient should be prescribed an antiseptic mouthwash for 7 to 10 days and should have a soft bland diet until the donor site has healed. The donor site usually re-epithelializes within 2 to 3 weeks.
13.4 Hard Palate Graft
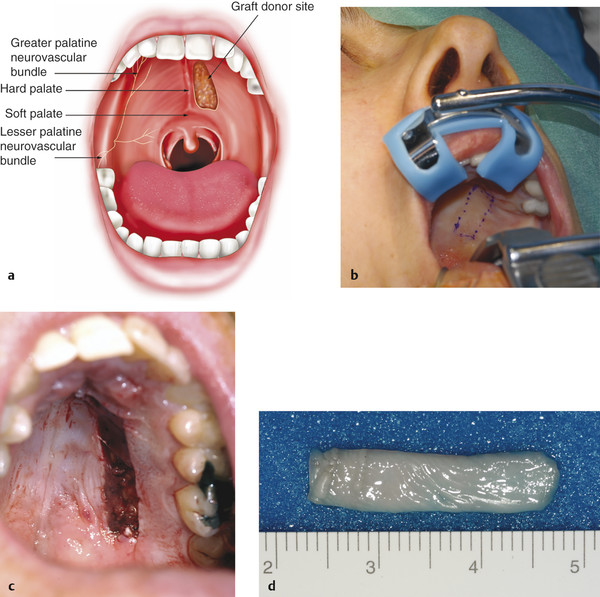
Hard palate mucosa is more rigid than lip or buccal mucosa but has a rougher surface. It does not tend to shrink more than 10% postoperatively. As a general rule it should not be used in the upper eyelid where it may abrade the cornea, except in an anophthalmic patient.
The anesthetist should place a throat pack after induction of anesthesia. The donor site is injected with 3 to 5 mL of 0.5% bupivacaine with 1:200,000 units of adrenaline before the patient is prepared and draped for surgery.
13.4.1 Indications
A spacer graft in lower lid retractor recession surgery.
A posterior lamellar graft in lower eyelid reconstructive surgery.
A graft in severe lower eyelid cicatricial entropion surgery.
A graft for the reconstruction of a contracted socket.
Surgical Procedure
A Boyle–Davis (or similar) retractor is carefully placed, ensuring that the endotracheal tube is not displaced. The patient should be placed in a reverse Trendelenburg position. The surgeon should stand at the side of the patient and should wear a headlight. The anesthetist should tilt the head posteriorly to improve access to the hard palate.
The hard palate is dried with a dry swab.
The graft size to be harvested is measured and the margins marked on the hard palate, avoiding the gingival border, the midline, and the soft palate (Fig. 13‑7a,b).
An incision is made with a no. 15 Bard–Parker blade through the surface epithelium and into the adipose layer beneath. The periosteum should not be disturbed.
The graft is then removed using a no. 66 Beaver blade, keeping the dissection plane within the firm adipose layer (Fig. 13‑7c,d). Westcott scissors may aid the dissection once the plane has been established with the no. 66 blade.
The graft is protected in a gauze swab moistened with saline. This must be stored carefully to avoid inadvertent loss of the graft.
A patty gently moistened with 1:1000 units of adrenaline is held over the donor site for 5 minutes and any bleeding vessels are cauterized using bipolar cautery. The wound is left to heal by secondary intention.
Excess adipose tissue is removed with blunt-tipped Westcott scissors while holding the graft over the index finger of the nondominant hand.
The graft is then placed on the recipient bed and interrupted 7–0 Vicryl sutures are placed from the graft edge to the recipient conjunctival edge, ensuring that the sutures are buried.
Related posts:




Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


