Abstract
Infections in the hand are a common and diverse group of conditions. The physician’s evaluation begins with an overall assessment of the patient, including past medical history, allergies, occupation, and activities. Assessment continues with the history, physical examination, imaging, and laboratory testing to make a diagnosis. Once a diagnosis has been made, treatment should be initiated. Timing of treatment often impacts prognosis and patient outcomes. It is imperative that the treating physician understand the common hand infection conditions so that patients can receive timely and proper treatment.
13 Infection
I. Patient Evaluation
Stabilize patient
First priority is treating sepsis if present with broad spectrum antibiotics and intravenous (IV) fluid administration.
History
Time of onset.
Mechanism.
Occupation, handedness, social situation, and activity level.
Medical evaluation of comorbidities, allergies (especially to antibiotics), anticipate risks with anesthesia or surgery.
Physical examination
Location of symptoms on flexor versus extensor surfaces.
Erythema, swelling, gross purulence, crepitus, and fluid collections.
Pain with palpation or passive movement of fingers/wrist.
Preoperative tests
Blood cultures if worried about systemic infection, ideally before antibiotics.
Complete blood count (CBC), basic metabolic panel (BMP), prothrombin time and international normalized ratio (PT/INR), partial thromboplastin time (PTT), type and screen.
Electrocardiogram (EKG) and chest X-ray based upon medical history.
II. Important Infections
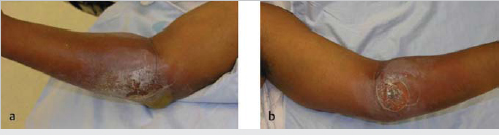
A. Necrotizing Fasciitis
Background
Life and limb threatening surgical emergency.
Bacterial spread along fascial planes.
Presentation
Pain.
Bullae, cutaneous hemorrhage, skin sloughing, and crepitus (► Fig. 13.1).
Most commonly caused by polymicrobial infection; most common isolated organism is Group A strep.
Testing
Imaging not required for diagnosis but may show gas in tissue planes.
Labs consistent with inflammatory/infectious process: LRINEC scoring (score ≥6 predictive of necrotizing fasciitis).
C-reactive protein (CRP) ≥15 = 4 points.
WBC<15 = 0 points; 15-25 = 1 point; >25 =2 points.
Hemoglobin >13.5 = 0 points; 11-13.5 = 1 point; <11 =2 points.
Sodium ≥135 =2 points.
Creatinine >1.6 = 2 points.
Glucose ≥180 = 2 points.
Treatment
Surgical emergency—incision and drainage (remove all necrotic tissue) versus amputation with obtaining intraoperative cultures.
Timing to operating room (OR) most important factor in survival.
Risk factors for poor outcome are delay in time to OR, age >50 years, and diabetes.
Classically see “dishwater” fluid from liquefied fat intraoperatively.
Broad spectrum IVantibiotics
Empiric antibiotics: Penicillin G, clindamycin, metronidazole, and aminoglycoside.
Strep or clostridium: Penicillin G.
Polymicrobial: Imipenem, doripenem, or meropenem.
Methicillin-resistant Staphylococcus aureus (MRSA): Vancomycin or daptomycin.
B. Septic Arthritis
Background
Infection within a joint.
Cartilage can be destroyed secondary to release of bacterial toxins and proteolytic enzymes.
Most common organism is Staphylococcus aureus, but consider Neisseria gonorrhoeae in those with risk factors.
Presentation
Swollen, painful joint with decreased range of motion; pain with active and passive range of motion; pain with axial loading of joint.
Testing
Joint aspiration.
WBC >50,000, polymorphonuclear leukocytes >75%, glucose level 40 mg < fasting glucose.
Treatment
Incision and drainage in OR with cultures.
Intravenous antibiotics.
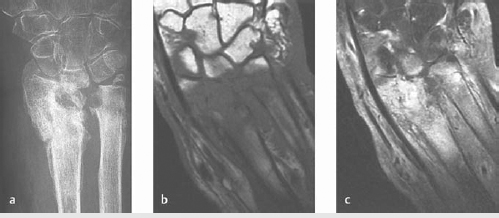
C. Osteomyelitis
Background
Infection of bone.
Risk factors include recent surgery, trauma, IV drug use immunocompromised state, poor blood supply, and neuropathy.
Most common organisms are S. aureus and Streptococcus.
Sequestrum is an area of dead bone near an infected nidus.
Involucrum is new bone forming around area of necrosis.
Presentation
History of fever, although fever is usually only seen in acute cases.
Erythema, tenderness, and sinus tracts can all be seen on examination.
Testing
Radiographs obtained first can show lucencies/sclerosis and periosteal reaction.
MRI with contrast best test to assess for extent of infection and assist in surgical planning (► Fig. 13.2).
CBC, erythrocyte sedimentation rate (ESR), CRP, and blood cultures should be obtained.
Treatment
Nonoperative
Only when operative intervention is not possible.
Operative
Irrigation and debridement of all devitalized tissue; advanced cases may require amputation.
Obtain intraoperative or preoperative cultures to narrow antibiotics.
Antibiotics
Tailor based on bone cultures.
Related posts:
 6 Fractures, Dislocations, and Ligament Injuries of the Hand
6 Fractures, Dislocations, and Ligament Injuries of the Hand
 8 Fractures and Dislocations of the Distal Radius and Ulna
8 Fractures and Dislocations of the Distal Radius and Ulna
 14 Flexor Tendon Injury, Repair, and Reconstruction
14 Flexor Tendon Injury, Repair, and Reconstruction
 12 Tendinitis, Tendinosis, and Dupuytren’s Contracture
12 Tendinitis, Tendinosis, and Dupuytren’s Contracture
 Private: 20 Vascular Pathology of the Hand and Upper Extremities, including Kienbock’s Disease
Private: 20 Vascular Pathology of the Hand and Upper Extremities, including Kienbock’s Disease
 Private: 25 Fractures of the Pediatric Hand
Private: 25 Fractures of the Pediatric Hand
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


