13 Facial Danger Zone 4 – Nasolabial Region
Abstract
This chapter summarizes how to inject soft-tissue fillers into the nasolabial region. Patients often report a prominent nasolabial fold as they age, and one option for treatment is the injection of soft-tissue filler. The facial artery’s anatomical location is intimately related to the location of the nasolabial fold. We present safe techniques for injection soft-tissue filler into this region to prevent inadvertent injury to any major facial vessels.
Key Points for Maximizing Filler Safety in the Nasolabial Region
Use only FDA-approved reversible hyaluronic acid fillers in most areas of the face.
Hyaluronic acid fillers are reversible if there is a vascular issue or problem because they can be reversed with hyaluronidase.
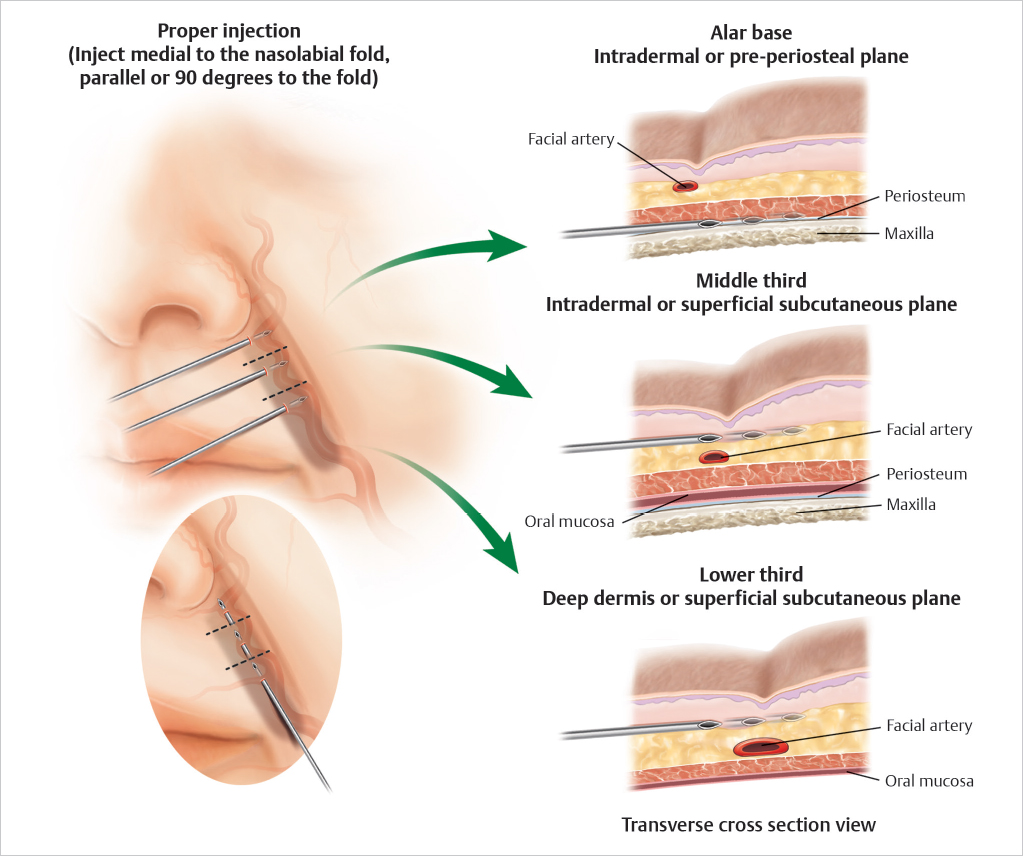
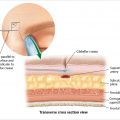
In the lower two-thirds of the nasolabial fold, inject into the deep dermis or superficial subcutaneous plane just medial to the nasolabial fold (▶ Fig. 13.1 ).
Near the alar base, inject either intradermally or in the preperiosteal plane. Use incremental deep depot injection techniques in the periapical areas (▶ Fig. 13.1 ).
Always perform using gentle, low-pressure anterograde/retrograde injections with constant motion in 1 mL syringes.
Do not inject along the alar rim, alar grooves, or nasal sidewall because the vasculature is superficial in these regions.
13.1 Safety Considerations in the Nasolabial Region
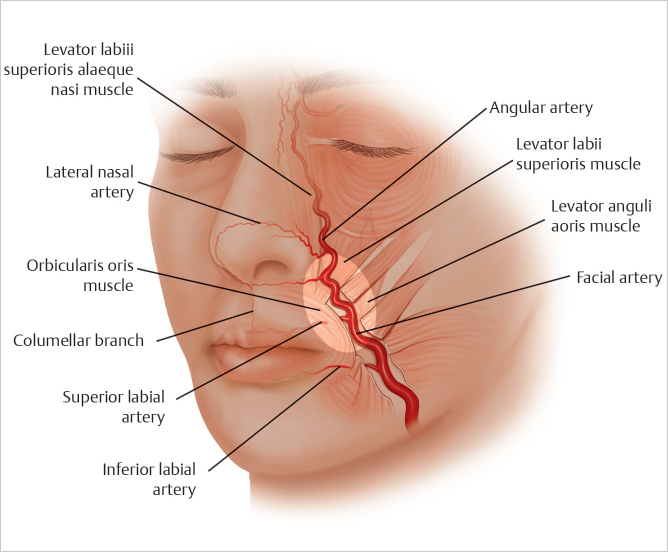
When injecting the nasolabial region, knowledge of the depth and course of the facial artery is paramount to prevent complications associated with intravascular injury (▶ Fig. 13.2).
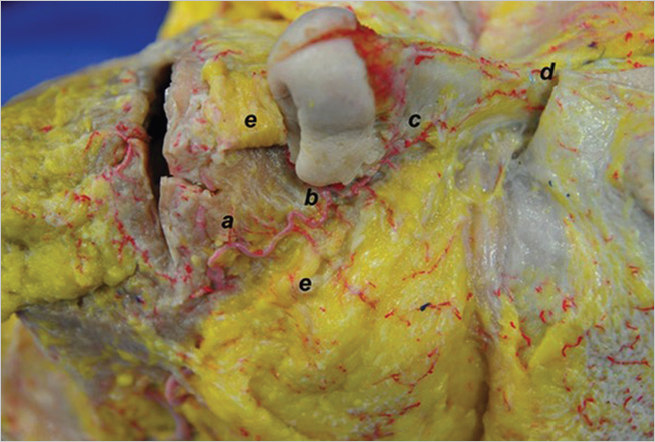
In the lower two-thirds of the nasolabial fold, the facial artery course lies beneath the muscle or in the deeper planes above the muscle (▶ Fig. 13.3 ).
The artery becomes superficial at the upper third of the nasolabial fold and is most at risk for injury at this level (▶ Fig. 13.3) (Video 13.1).
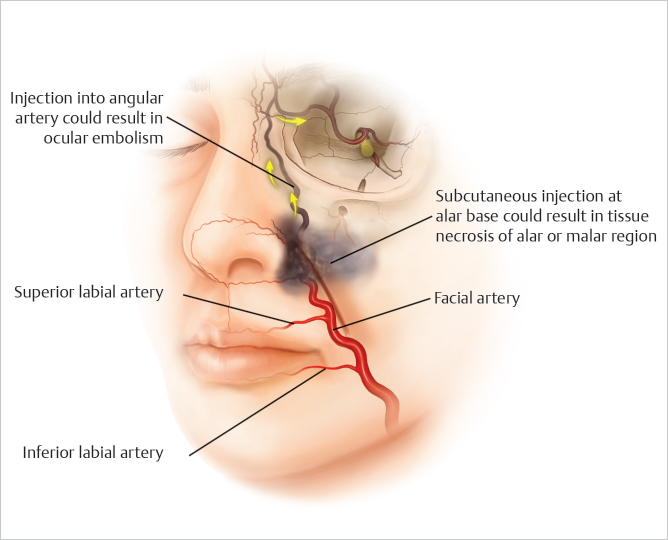
Subcutaneous injections in the upper third of the nasolabial fold can lead to soft-tissue necrosis of the alar or malar regions if there is intravascular injury (▶ Fig. 13.4 ).
In the upper third of the nasolabial fold and superior to it, intravascular injections into the angular artery could result in ocular embolism (▶ Fig. 13.4 ).
The nasolabial fold is the second most common injection site for tissue necrosis and the third most common site leading to visual loss. 1 , 2
Related posts:




Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


