The thumb constitutes 40% of hand function and attempt for salvage must be always made. However, it poses a challenge in terms of microsurgical access and positioning. The ulnar digital artery (UDA) is dominant compared to the radial digital artery (RDA) and there is often a good dorsal supply in the thumb from the princeps pollicis artery. If there is complete division of the UDA and RDA, the thumb can sometimes maintain sufficient vascularity with the dorsal supply.
In both thumb revascularization and replantation, vein grafting is usually required as tensionless anastomosis of the arteries is rarely possible. Jump vein grafting out of the zone of trauma to the radial artery in the anatomical snuff box enables a reliable anastomosis and avoids the technical difficulties of thumb positioning during microsurgery. We describe the sequence of steps in a case where a thumb was revascularized after a circular saw injury at the level of the interphalangeal joint (IPJ) (Fig. 12‑1, Fig. 12‑2, Fig. 12‑3, Fig. 12‑4, Fig. 12‑5, Fig. 12‑6, Fig. 12‑7).
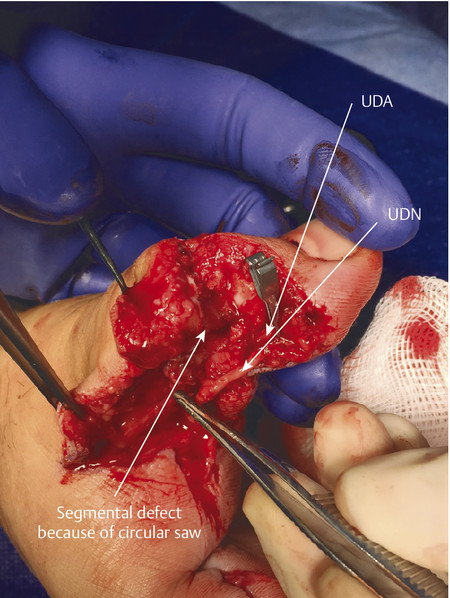
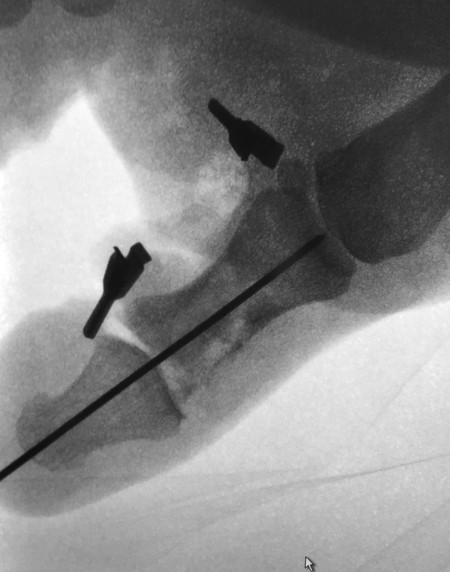
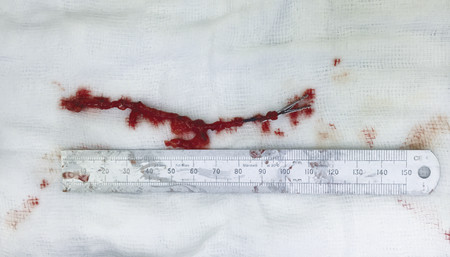
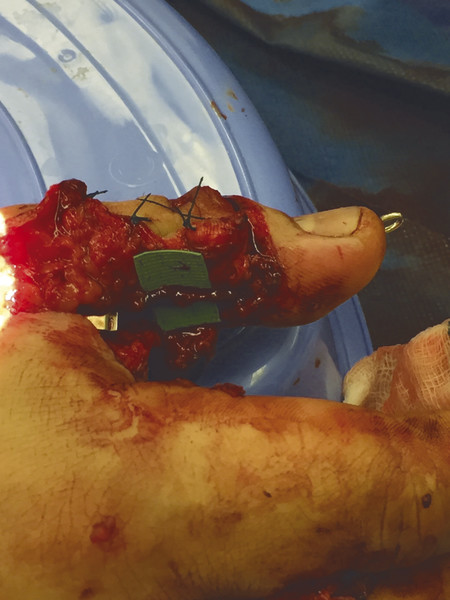
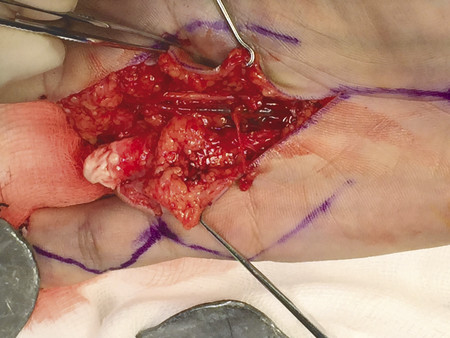
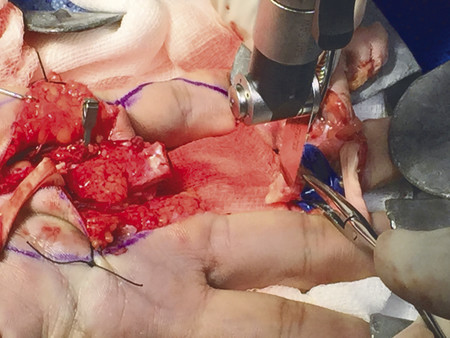
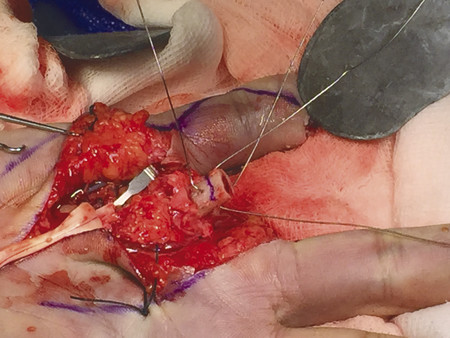
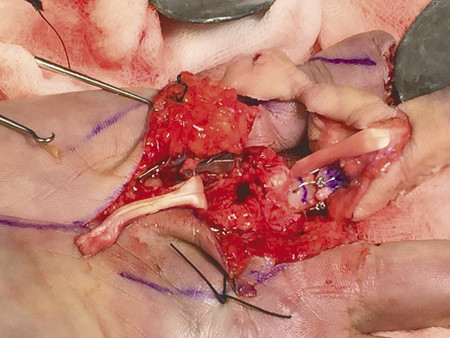
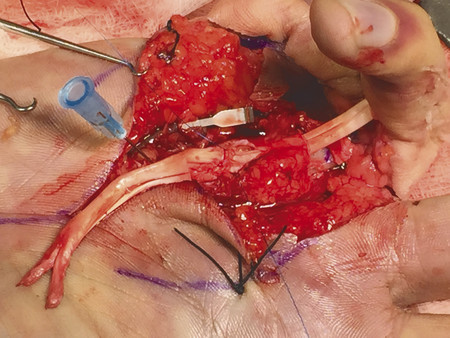
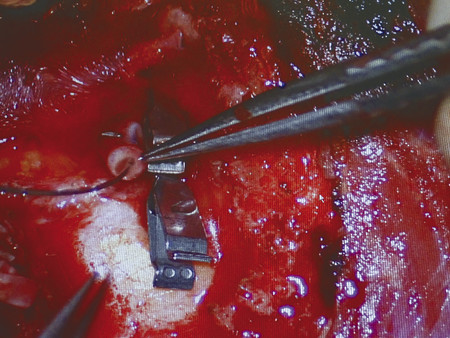
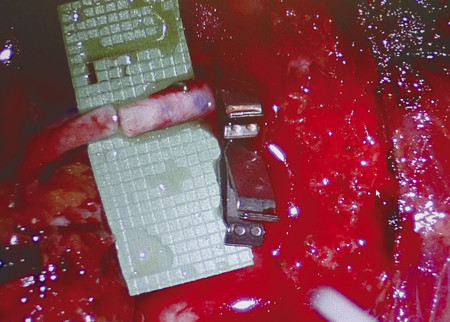
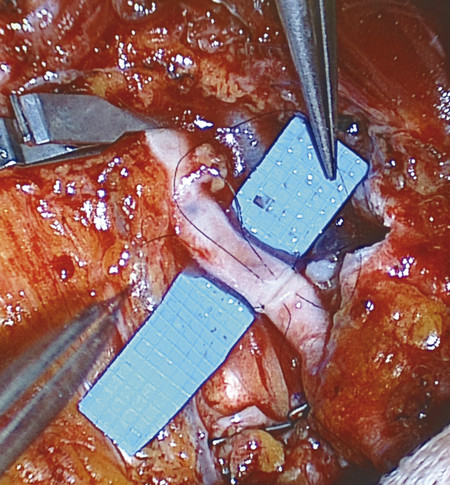
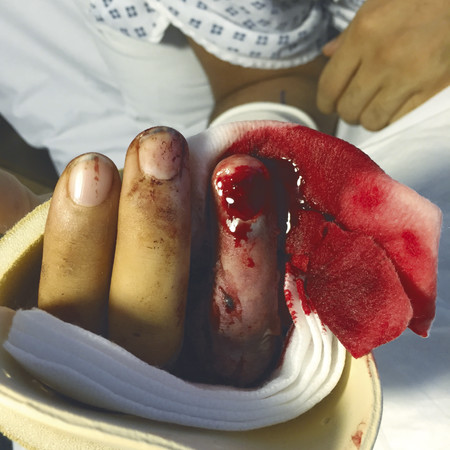
Fig. 12.1 Circular saw injury through thumb IPJ. Thumb held on by small dorsal skin bridge and the FPL tendon. Capillary refill is not present and oxygen saturations reading is unrecordable.Fig. 12.2 Both the volar neurovascular structures are divided in this case with a segmental defect. The UDA is identified distally and resected to healthy artery just proximal to the trifurcation. The UDA cannot be identified proximally in this figure. A single Acland’s clamp is placed over the distal UDA. UDA, ulnar digital artery; UDN, ulnar digital nerve.Fig. 12.3 Radial artery identified in the anatomical snuff box.Fig. 12.4 Rapid osteosynthesis performed with single axial K-wire passed retrograde first before driving wire across IPJ.Fig. 12.5 Because of the large zone of injury and poor flow from the proximal cut end of UDA and princeps pollicis artery. A jump vein graft was harvested from the forearm.Fig. 12.6 An 11-cm vein graft was taken from the forearm. An alternative site can be the vena comitans of the radial artery in the wrist. Plenty of fat was taken to cushion the vein graft and allow for swifter harvest. Ink and an Acland clamp mark the proximal extent of the vein as it needs to be turned around due to valves.Fig. 12.7 The harvested vein graft was bridged from the radial artery to the UDA. A double Acland clamp isolated a segment of the radial artery in the snuff box and an end-to-side anastomosis was performed with 9.0 ST. The distal anastomosis was performed end to end with the UDA.
12.2 Digital Replantation
Digital replantation follows a sequence of steps and can be performed if the principles in the previous chapters in this book are learned (Fig. 12‑8, Fig. 12‑9, Fig. 12‑10, Fig. 12‑11, Fig. 12‑12, Fig. 12‑13, Fig. 12‑14, Fig. 12‑15, Fig. 12‑16, Fig. 12‑17, Fig. 12‑18, Fig. 12‑19, Fig. 12‑20, Fig. 12‑21, Fig. 12‑22, Fig. 12‑23, Fig. 12‑24, Fig. 12‑25, Fig. 12‑26, Fig. 12‑27, Fig. 12‑28, Fig. 12‑29). Osteosynthesis should be performed first to provide a stable platform followed by repair of macroscopic structures (tendons). Microscopic structures should then be repaired (nerve, artery, veins). Amputations of the thumb, pediatric amputation, and multidigit loss are all absolute indications for replantation. However, some cases where there are crush or avulsion injuries, success rates are poor and in the figure of 50 to 60%. Success does not just rely on survival but on long-term function and replantation proximal to the flexor digitorum superficialis (FDS) insertion may never regain a normal range of motion.
Generally, clean-cut amputations distal to the FDS insertion with minimal ischemic time (< 12 hours warm ischemia) do well. Those with avulsion-type mechanism and long ischemic time have poorer outcomes as in the case demonstrated; and in many cases a no-reflow phenomenon occurs. Patient selection is therefore crucial and if an anastomosis is to be performed in a crush avulsion case, it should be done outside of a zone of trauma and in some cases vein grafts may be necessary to increase the chances of success.
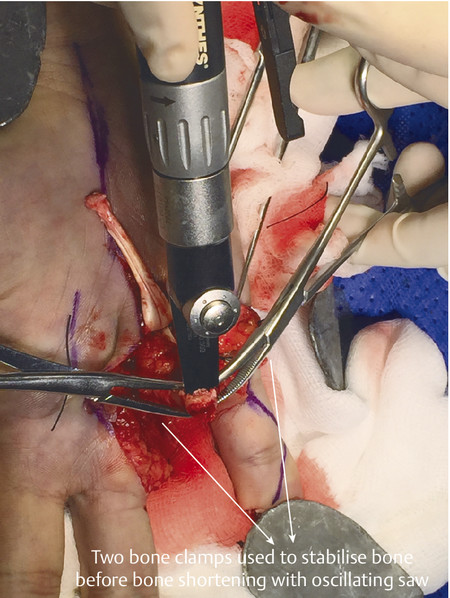
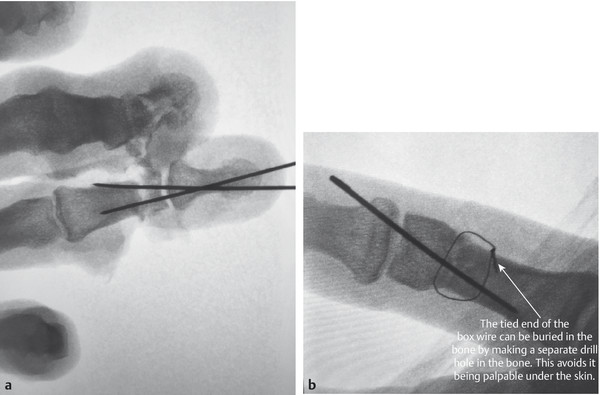
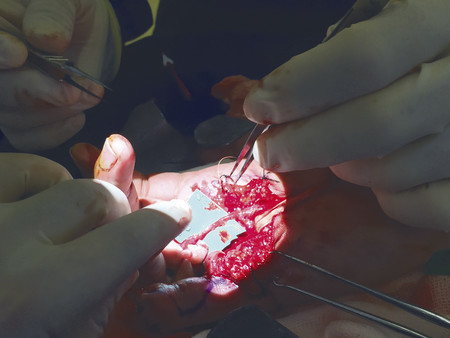
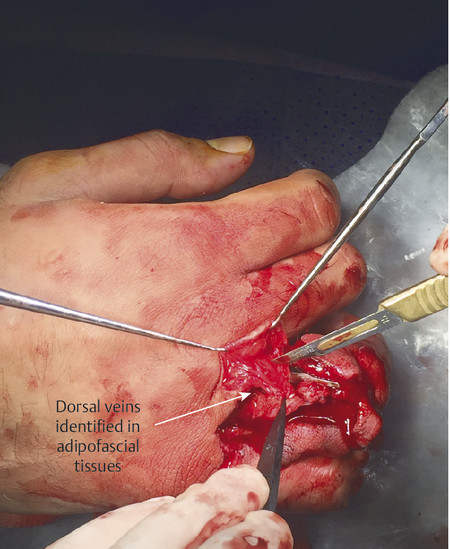
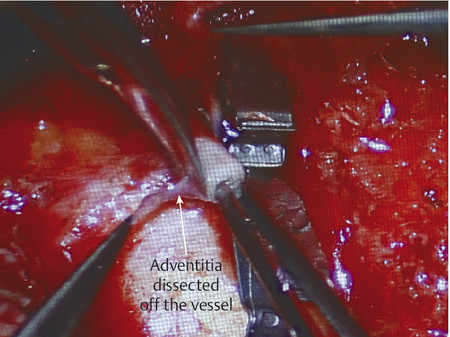
Fig. 12.8 (a,b) Avulsion crush amputation of little and ring fingers. Digits were wrapped in wet gauze in a plastic bag placed on ice. The amputated part should never be placed directly on ice.Fig. 12.9 Amputated parts should be explored in theater to see if there are any suitable vessels. This will buy time while the patient is being anesthetized. The amputated digit can be stabilized during this process with pins and vascular loops. In a multidigit amputation, if one amputated part is unreplantable it should be used for “spare parts” for the remaining digits.Fig. 12.10 Vein grafts marked in proximal forearm before arm exsanguination.Fig. 12.11 Common digital nerve and artery found outside zone of trauma proximally.Fig. 12.12 Bone ends are shortened in preparation for osteosynthesis. Glove used to protect neurovascular bundles.Fig. 12.13 Cross-clamping method to stabilize bone before shortening.Fig. 12.14 90–90 wiring used to bring bone ends together rapidly. This avoids the use of a C-arm during the procedure and is rapid, cheap, and provides excellent bone-to-bone contact.Fig. 12.15 Radiograph of box wires.Fig. 12.16 Alternative method of fixation is K-wires. Amputated part is prepared first with retrograde pass of two 0.9 K-wires.Fig. 12.17 (a,b) Alternative methods of osteosynthesis include retrograde cross K-wire fixation or a single K-wire and a loop of interosseous wire described by Lister.Fig. 12.18 Completed intraoperative 90–90 box wiring.Fig. 12.19 Next the flexor digitorum profundus (FDP) tendon is repaired with preservation of the A2 pulley. The FDS was not repaired as it had been avulsed from the bone and FDS repair would compromise tendon glide. The extensor tendon is next repaired.Fig. 12.20 Nerve repair is performed next under tourniquet. If nerves cannot be repaired, then the digit will have no use as an insensate digit. The tourniquet is then let down and arterial anastomosis is performed. One must check that there is good flow proximally by releasing the Acland clamp.Fig. 12.21 Veins can be difficult to find and can be easily found in the adipofascial tissue under the dorsal skin flaps. After arterial anastomosis, they become engorged and more readily visible. Ideally, two venous anastomoses should be performed.Fig. 12.22 When preparing for the arterial anastomosis, the adventitia is stripped off. The artery is then dilated with vessel dilators.Fig. 12.23 Heparin saline is used to irrigate the vessel lumen and remove any visible clots.Fig. 12.24 The artery is prepared for anastomosis. A single Acland clamp can be used and a background helps with visualization.Fig. 12.25 A double Acland provides more optimal control and enables the repair of the anterior wall first and then turning over for posterior wall repair. This is, however, not always possible in a confined space and a back wall first anastomosis must be performed.Fig. 12.26 The best way to avoid catching the posterior wall with anterior wall stitches is to suture the back wall first.Fig. 12.27 The final stitches on the anterior wall are done using an untied Harashina stitch. This reduces the chances of catching the back wall of the anastomosis.Fig. 12.28 Completed replantation of ring finger.Fig. 12.29 Congested digit managed with heparin-soaked gauze to allow bleeding from the nailbed.
Only gold members can continue reading. Log In or Register to continue