10 Facial Danger Zone 1 – Glabellar Region
Abstract
The glabellar region is the most common filler injection site leading to blindness due to the rich anastomotic network between the supratrochlear, supraorbital, and dorsal nasal arteries. Inadvertent injection into any of these arteries can create retrograde embolus into the ophthalmic artery. The supratrochlear artery courses very superficially, often within the glabellar frown crease. Injections in the glabellar rhytides should be performed very superficially within the dermis using serial puncture technique and low pressure. Digital pressure should be applied at the supraorbital rim to occlude the supratrochlear and supraorbital vessels while injecting in the glabella.
Key Points for Maximizing Filler Safety in the Glabellar Region
Use fillers primarily for superficial line-filling in the glabellar area.
Use serial puncture technique to deposit small aliquots intradermally along rhytids.
Use digital pressure to occlude the supraorbital and supratrochlear vessels at the supraorbital rim.
Do not attempt to overcorrect deep rhytids in the glabellar region.
10.1 Safety Considerations in the Glabellar Region
The glabella has been reported as the most common filler injection site leading to blindness, and the second most common for skin necrosis. 1 , 2 , 3 , 4 , 5
Rich anastomoses exist between the supratrochlear, supraorbital, and dorsal nasal arteries, all of which are branches of the ophthalmic artery (▶ Fig. 10.1a).
Inadvertent intravascular injection into the nasoglabellar arcade can create retrograde propagation of foreign material into the ophthalmic artery (▶ Fig. 10.1b).
Subsequent distal embolism from the ophthalmic artery can cause vision loss and/or tissue necrosis. 6 , 7

10.2 Pertinent Anatomy of the Brow and Glabellar Region
A cadaveric dissection showing pertinent arteries and muscles in the glabellar and brow region is shown in ▶ Fig. 10.2 .
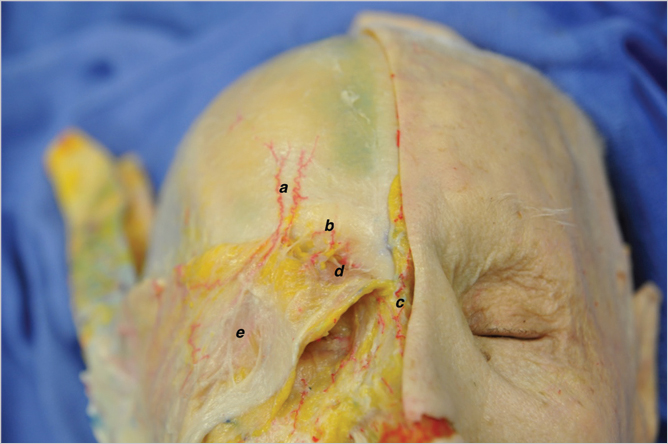
10.2.1 Arteries
(▶Fig. 10.3)

Supratrochlear Artery
A branch of the ophthalmic artery.
Exits the superomedial orbit in-line with the median canthus +/- 3 mm, or 17 to 22 mm lateral to midline. 8 , 9 , 10 , 11
Traverses vertically through the corrugator, then through the frontalis and orbicularis to enter the subcutaneous plane 15 to 25 mm above the orbital rim. 9
Continues superiorly in paramedian forehead in the subcutaneous plane, 15 to 20 mm from midline. 10
Related posts:





Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


