10 Breast Radiotherapy in Oncoplastic Surgery
Breast conservation represents a major advancement in the treatment of breast cancer, offering women the potential to preserve their breast without impairing their oncologic outcomes. Continued advancements in surgical and radiotherapy techniques over the past several decades has led to the evolution of breast conservation and the ability for more women to be eligible for the treatment. Recently, surgical methods known as oncoplastic techniques have been devised and are increasingly being used to offer women undergoing breast conservation the ability to enhance breast cosmesis, symmetry, and quality of life without impacting oncologic outcomes. The purpose of this chapter is to evaluate outcomes in patients undergoing oncologic surgery and radiotherapy.
Breast Conservation and Breast Irradiation Techniques
Breast-conserving therapy (BCT) represents a standard of care approach for women with invasive and noninvasive breast cancers. Multiple randomized studies with long-term follow-up have demonstrated the equivalence of BCT and mastectomy in patients with invasive disease, while studies with long-term outcomes have demonstrated the efficacy of BCT in women with ductal carcinoma in situ (DCIS). 1 – 5 Furthermore, multiple studies have shown the increase in local recurrence with the omission of radiotherapy, with meta-analyses demonstrating reduction in local recurrence for invasive and noninvasive cancers and reduction in breast cancer mortality for invasive cancers with radiotherapy. 6 – 7 Breast-conserving therapy has also been shown to improve quality of life and breast cosmetic outcomes for patients compared with mastectomy. 8 , 9 An important distinction between BCT and mastectomy is that BCT requires continued follow-up with imaging of the involved breast as well as monitoring for skin and subcutaneous tissue toxicity and evaluation of symmetry and cosmesis. 10 , 11
Traditionally, radiotherapy was delivered using whole-breast irradiation with two-dimensional techniques. Over the past several decades, radiotherapy has evolved to incorporate three-dimensional planning. 12
Radiotherapy planning techniques use anatomic landmarks and target volumes to delineate the organs at risk and to localize the borders of the irradiation fields. When a patient receives a breast cancer treatment, the tissues targeted for full-dose irradiation include the whole breast and regional nodes, when indicated. Critical normal tissues—the heart, lungs, and contralateral breast—are avoided or are subject to dose reduction or modulation when possible. Currently the most commonly used technique to treat the whole breast is called a tangential beam irradiation. This field arrangement is designed to minimize the exposure of the intrathoracic structures, especially the heart and lungs, to radiation. Treatment plans are able to evaluate the dose to the breast, lumpectomy cavity, as well as organs at risk. More recently, intensity-modulated radiotherapy has been used to further optimize treatment plans and reduce the dose to critical structures, including the heart, with initial data demonstrating reduction in acute and chronic toxicities. 13 – 15
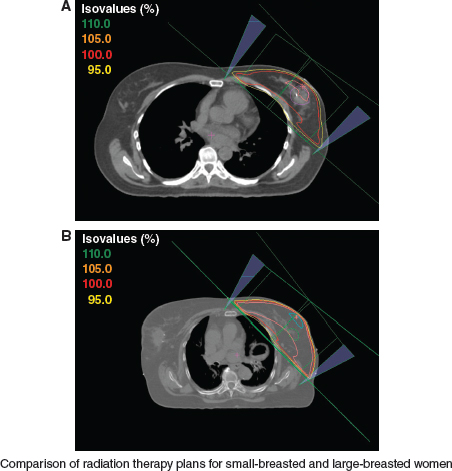
Techniques to deliver breast radiotherapy can differ, depending on the size of the breast. A and B both show radiation fields for patients who have tangents with standard, fixed-angle wedges. The isodose values on the left of each image correspond to the percentage of the prescribed dose. Lines of the same color on the CT simulation axial slice show the corresponding dose distribution in the breast tissue. B demonstrates that in a large-breasted patient, the 105% isodose covers a larger volume of breast tissue, whereas A reveals that the 110% isodose is not present at all in the smaller-breasted patient. An increased-dose inhomogeneity is inherent for larger-breasted patients, because it is affected by the size and shape of the breast and by the separation distance across the posterior field edge from the medial to the lateral field border. A larger breast size or a larger separation, especially more than 25 cm, results in greater dose inhomogeneity in the treatment volume. Homogeneity within 7% to 10% of the prescribed dose is desirable.
There are various compensation methods used to modulate the dose distribution to achieve improved homogeneity. One such technique is the open-field, uncompensated treatment plan (see Fig. 10-1). One technique that is widely used to ameliorate dose inhomogeneity is the placement of compensator devices in the beam, often using wedge compensators of fixed angles or, more recently, virtual wedges of variable compensation degrees. The wide part of the wedge (or compensator) is placed in the beam in the same orientation as the tip of the triangle of the breast, to compensate for the thinner tissue separation at the apex of the breast at the nipple area.
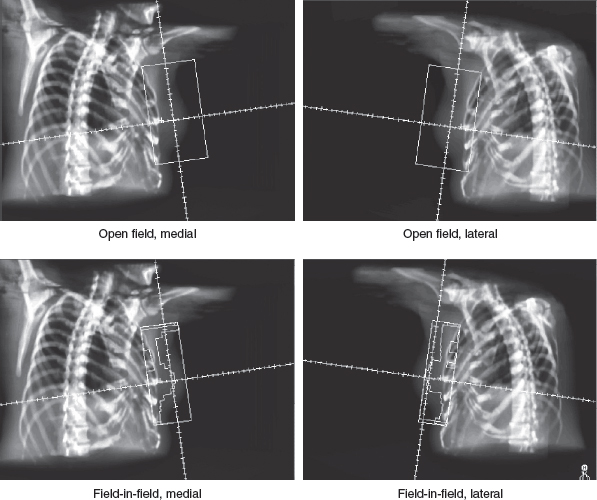
After multileaf collimation (MLC) became available, custom compensation using field-in-field MLC shaping became increasingly popular. With this technique, the MLC is used to shape smaller fields that correspond to the areas of high-dose inhomogeneity, covering the high-dose regions with custom-shaped fields for small portions of the total dose to improve homogeneity. Another technique, intensity-modulated radiotherapy, typically involves three-dimensional planning using dose-volume constraints for target tissues and normal organs, with either forward or inverse planned dose calculations. Each compensation method can reduce and redistribute the “hot spots” (isodose regions in excess of 100% of the prescribed dose) compared with open fields with no compensation.
Despite advances in radiotherapy techniques (3D-CRT) and treatment delivery (IMRT), concerns exist regarding toxicity and cosmetic outcomes in women undergoing BCT. Although some of this is associated with radiotherapy, much of the difference in symmetry and cosmesis can be attributed to the reduction in breast volume after breast-conserving surgery.
Oncoplastic surgery first and foremost is an oncologic procedure that allows excision of the tumor with incorporation of multiple techniques (reduction mammoplasty, mastopexy, tissue transfer/rearrangement) to enhance cosmetic outcomes and patient satisfaction after BCT. 16 , 17
At this time, limited data are available on clinical, cosmetic, and toxicity-related outcomes with radiotherapy in patients undergoing oncoplastic procedures. However, in light of the growing use of such techniques, it is imperative that clinicians be aware of the data currently available.
Oncoplastic Techniques
Oncoplastic techniques do not represent a single procedure but rather a combination of techniques used in conjunction with each other based on the patient’s breast size, anatomy, tumor location, and lumpectomy cavity size to enhance cosmetic outcomes without impairing oncologic outcomes.
The most commonly used oncoplastic technique is tissue rearrangement and includes local glandular transfers or flaps as well as transfer or rearrangement from local or regional sites. These techniques work to minimize the defects after BCS and/or shift the defect to a less visible area. 16 A second technique commonly employed is mastopexy, which can be particularly helpful in patients with significant breast ptosis or in large-breasted patients; with this technique, the contralateral breast may also be treated to enhance symmetry. Finally, reduction mammaplasty can be used bilaterally to enhance symmetry in large-breasted women, with the contralateral breast reduced to match the breast after resection. The contralateral breast can be operated on initially or in a delayed setting to allow changes after adjuvant treatment. 17
Cosmesis and Toxicity of Traditional Radiotherapy
The predominant toxicities associated with breast cancer radiotherapy include skin or subcutaneous tissue toxicity and the potential for impaired cosmesis as a result. Acute reactions typically include skin erythema, hyperpigmentation, rash, and possibly dry or moist desquamation. Acute toxicity occurs in skin and other acute-reacting tissues, with the likelihood of toxicity related to breast size. Other acute toxicities include breast swelling, edema of the skin, chest wall inflammation, fatigue, and subacute pneumonitis. There is no technical reason to postulate that oncoplastic reconstructions would be associated with worsened acute toxicities than those seen after a standard lumpectomy. Chronic toxicities are largely caused by the development of fibrosis and microvascular compromise in the treated tissues during the months after radiotherapy. Fibrosis can lead to distortion or asymmetry of the breast, although this is usually a relatively subtle effect. The risk of late fibrosis is related in part to the dose inhomogeneity, which is more pronounced in larger-breasted patients. It is also probably attributable to the extent of postoperative scarring, and thus more extensive surgery may also increase the risk of late fibrosis. If immediate oncoplastic reconstruction results in increased surgical scar tissue, cosmesis after radiotherapy could be compromised. However, because many women who undergo oncoplastic reconstruction may have otherwise required mastectomy or would have had greater asymmetry without the oncoplastic procedures, it is likely that the overall cosmetic outcome will be more satisfactory for these patients.
The cosmetic appearance of the treated breast after whole-breast irradiation is typically recorded by the physician at each follow-up visit. Radiation oncologists use a four-point cosmetic scoring system to compare the treated and untreated breast. The appearance of the treated breast can be scored as “excellent” (nearly identical to the untreated breast), “good” (slight difference of less than 25% asymmetry between breasts), “fair” (obvious differences between breasts), or “poor” (marked distortion of the treated breast). 18 , 19 Traditionally, excellent or good cosmetic outcomes have been noted in more than 70% of women with long-term follow-up. A series from Fowble et al 18 evaluated 697 women with stage I/II disease treated with BCT and with 58-month follow-up, a 93% rate of excellent or good cosmesis was noted. An analysis from Wazer et al 19 found that factors associated with adverse cosmetic outcomes included the volume of breast tissue resected. Oncoplastic techniques would be able to help with this by reducing the tissue deficit in the area around the lumpectomy cavity. Additionally, previous studies have documented inferior outcomes with the use of reexcision, the placement of the excision scar, the volume of skin excised, older patient age, a larger tumor size, the use of radiotherapy and medial or inferior tumors, which is often a result of less tissue and more-visible defects. 19 – 21
However, oncoplastic techniques exist specifically for this region to optimize cosmesis. 17 A more homogeneous dose of radiotherapy is associated with better long-term cosmesis; therefore the use of compensators or dose modulation to achieve a homogeneous dose is critical. Likewise, the total dose to the whole breast, the total dose of the tumor bed boost, and the dose per fraction may affect overall cosmesis. Whole-breast doses of less than or equal to 50 Gy in daily dose fractions of less than or equal to 2.6 Gy are typically used, and the total tumor bed dose is generally less than or equal to 66 Gy.
Large breast size has been consistently associated with inferior cosmetic outcomes following traditional radiotherapy; the rationale for increased toxicity and inferior cosmesis is based on larger skin folds, which can create an autobolus effect, exacerbating skin toxicity and also the potential for increased inhomogeneity with larger breast volumes.
Gray et al 22 evaluated 257 women undergoing BCT and found significantly higher rates of asymmetry and breast retraction in a large-breasted cohort compared with a small-breasted cohort. Similar findings were noted by Moody et al 23 ; they reported that 39% of women with large breasts had late radiation changes, compared with 6% of women with small breasts. A recent study from William Beaumont Hospital found that these outcomes persisted with standard and hypofractionated radiotherapy and that acute and chronic toxicities were increased in large-breasted patients. 24
In theory, oncoplastic techniques resulting in a smaller breast volume may improve homogeneity and cosmesis after irradiation; however, this has not been studied and must be balanced against the potential increase in surgical complications or by the impact of more extensive surgery compared with lumpectomy alone.
Related posts:
 6 Breast-Conserving Therapy: Decision-Making and Anticipating the Unfavorable Aesthetic and Functional Result
6 Breast-Conserving Therapy: Decision-Making and Anticipating the Unfavorable Aesthetic and Functional Result
 11 Indications and Benefits of Oncoplastic Breast Surgery
11 Indications and Benefits of Oncoplastic Breast Surgery
 9 Improving the Quadrantectomy Defect
9 Improving the Quadrantectomy Defect
 8 Improving the Partial Mastectomy Deformity
8 Improving the Partial Mastectomy Deformity
 14 Psychosocial Aspects of Oncoplastic Breast Conservation
14 Psychosocial Aspects of Oncoplastic Breast Conservation
 13 Timing of the Oncoplastic Reconstruction: Immediate, Delayed, and Delayed-Immediate
13 Timing of the Oncoplastic Reconstruction: Immediate, Delayed, and Delayed-Immediate
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


