1 Preliminary Remarks about the Region
The primary function of the female breast or mammary gland is nourishment of the newborn infant. The breasts are a symbol of femininity and are especially important in a woman’s self-image. This should be reflected in the diagnosis and treatment of breast disease and in reconstructive and corrective surgery. Breast cancer is the most common malignant disease in women.
1.1 Topography of Chest Wall, Axilla, and Back
1.1.1 Chest Wall
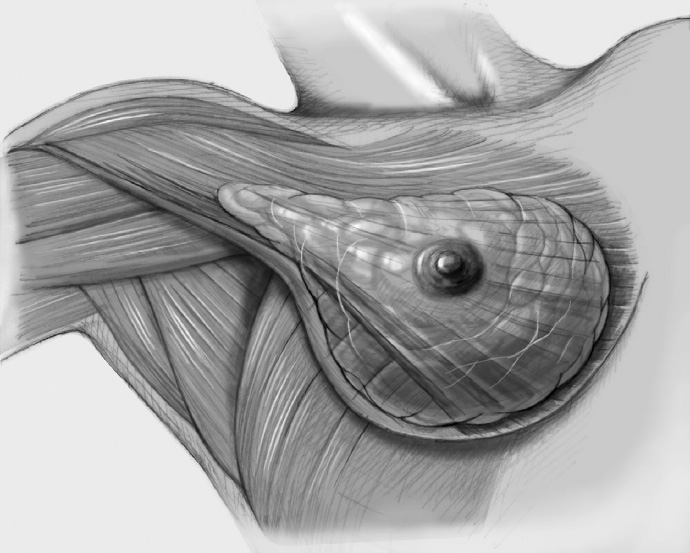
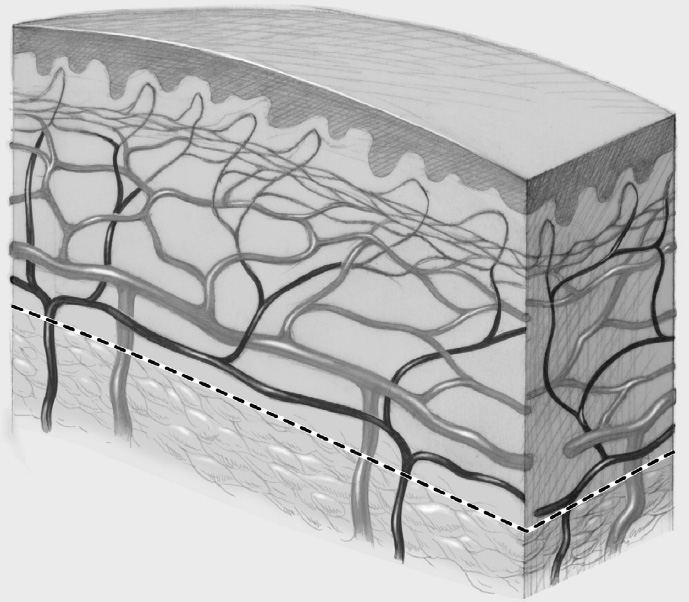
The breast lies on the chest wall with which it is intimately related with regard to blood supply, lymphatic drainage, and innervation. The breast develops embryologically from the skin. Anatomists and surgeons dispute whether the superficial body fascia can be divided into a superficial (Camper fascia) and a deep layer (Scarpa fascia), which explains the often inconsistent terminology. Doubt has been cast on the hypothesis that the mammary gland is located between the superficial and deep layers of the superficial fascia. What is certain is that the suspensory ligaments of the breast (ligaments of Cooper) pass through the parenchyma of the breast, radiating from the superficial fascia on the pectoralis muscle to the skin and helping to give the breasts their shape.
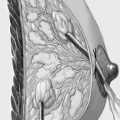
Mammary Glands
Mammary gland. The mammary gland consists of 16 to 20 distinct lobes. Each of these lobes has its own lactiferous duct opening into the nipple. These lactiferous ducts are divided into the excretory duct, directly behind the nipple, and the lactiferous sinus, a dilatation of the duct approximately 1 cm beneath its opening. The lactiferous ducts are a continuation of the lactiferous sinuses and branch extensively as they pass to the lobules, which are the site of actual milk production.
Montgomery glands. The areolar (Montgomery) glands, 10 to 15 in number, are located in a circle around the nipple and may be apparent as small elevations. Their secretion assists lactation.
Classification of pathological changes. Most (pathological) duct ectasia develops in the lactiferous sinuses. Invasive ductal breast cancer imitates the histological picture of the lactiferous ducts, while the typical histological acinar appearance of the lobules is seen in invasive lobular breast cancer.
Muscle Layers
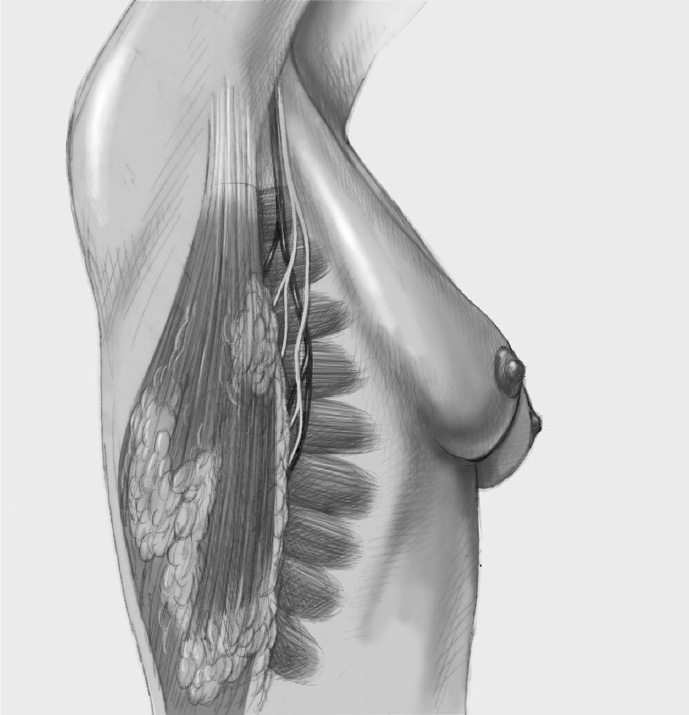
Most of the breast is situated on the pectoralis major muscle, which in turn lies directly on the actual chest wall, consisting of the ribs and intercostal muscles. The origin of the serratus anterior muscle, which runs posterolaterally, is beneath the diagonal inferior border of the pectoralis major between the axilla and the inferior part of the sternum. The pectoralis minor, with its origin on the scapula, radiates toward the anterior chest wall directly behind the pectoralis major. Other muscles that may be involved in breast surgery include the most cranial part of the rectus abdominis muscle, which is attached medially to the sternum and distal ribs, and the external oblique muscle of the abdomen, which is located together with the serratus anterior in the inferolateral part of the thorax.
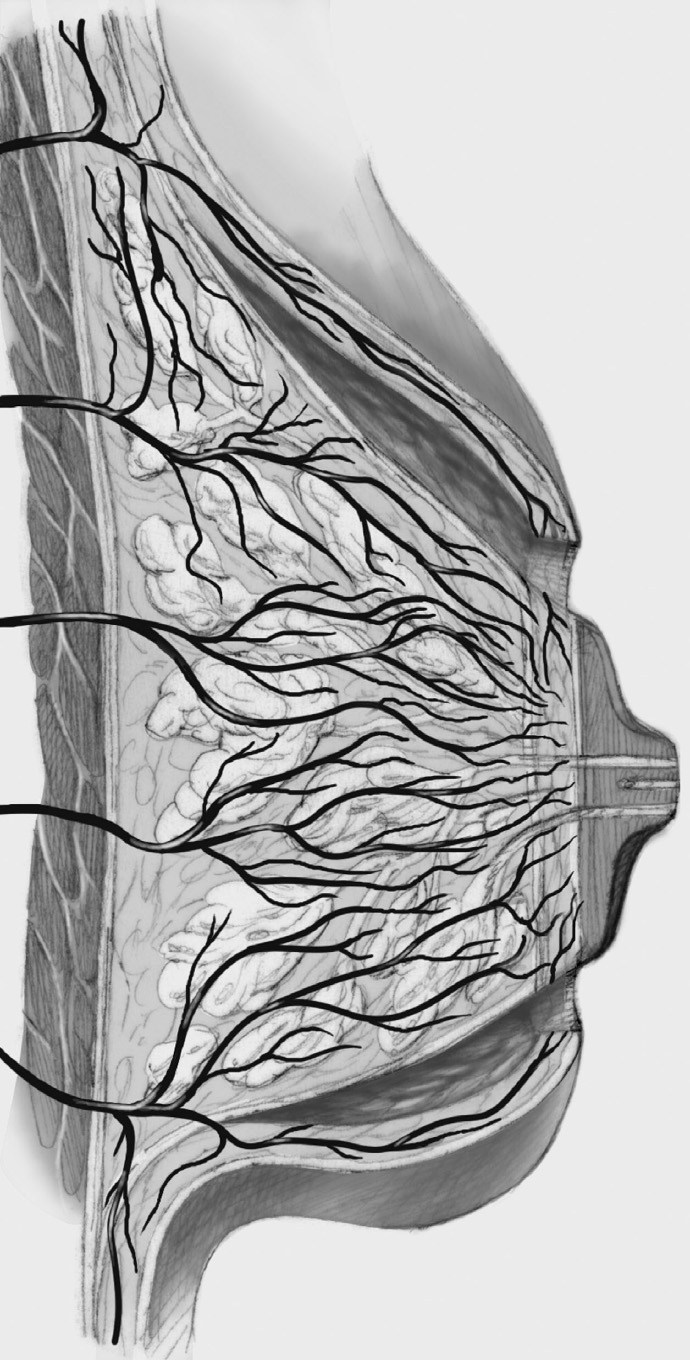
Blood Supply
From the medial side, the mammary gland is supplied by perforating branches of the internal mammary artery. From the axillary and cranial direction, the blood supply is mainly through the lateral thoracic artery, which runs on the serratus anterior beneath the pectoralis minor. The lateral blood supply comes from branches of the intercostal arteries. Sooner or later, the different arteries drain into a subcutaneous vascular plexus, which is very important in supplying the skin, areola, and nipple, and must be protected during many oncoplastic surgical procedures. Perforators from the pectoralis major enter the breast directly. Understanding the external and internal blood supply and course of the blood vessels of the breast is important especially for oncoplastic pedicle techniques (Chapter 3.3.2) and during dissection of the skin layer.
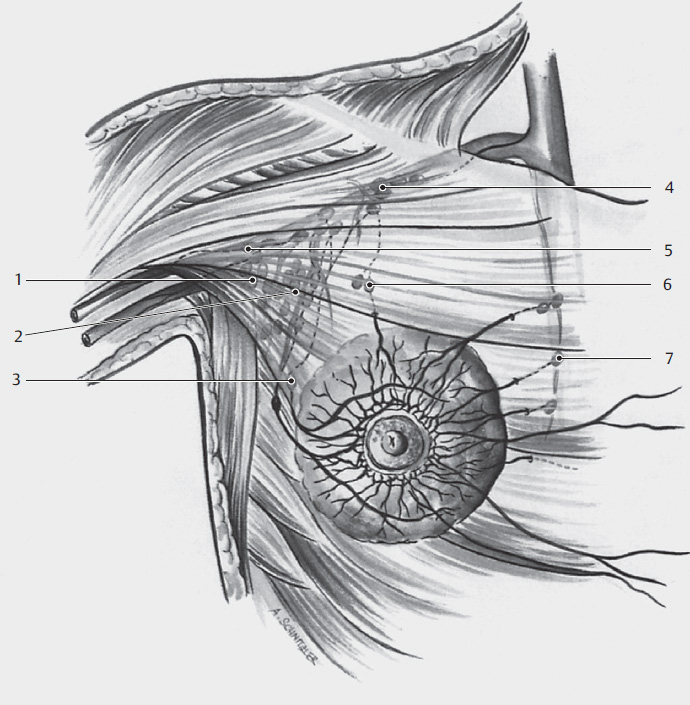
Lymphatic Drainage
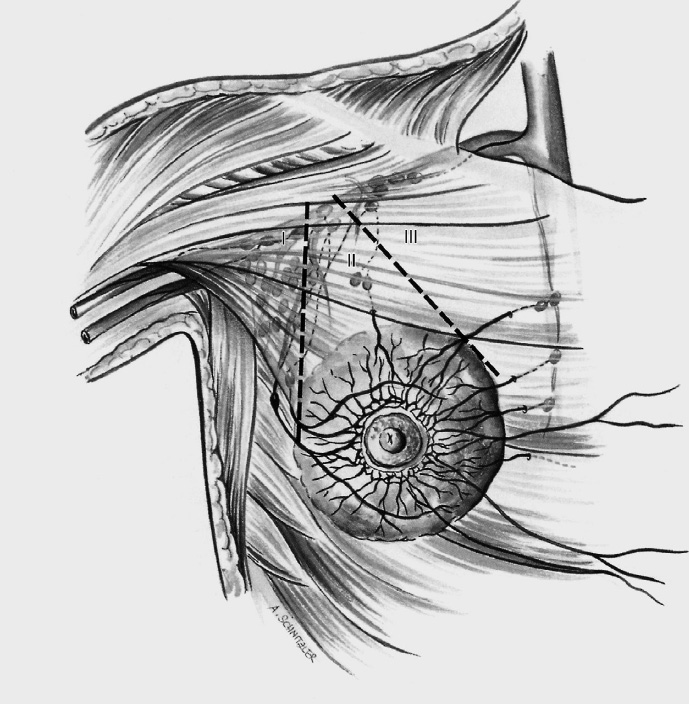
The lymphatic drainage of the breast essentially follows the arteriovenous vessels. The medial third of the breast drains especially to retrosternal lymph nodes. Smaller lymphatic pathways in the superior part of the breast can drain directly into the subclavian lymph nodes, partly through the Rotter (interpectoral) lymph nodes (level II). Most of the breast drains through the classic sentinel node group at the border of the pectoralis muscle into the level I axillary lymph nodes. Lymphatic vessels crossing the sternum to the contralateral side have also been described.
Innervation
The breast receives sensory innervation via a number of nerve pathways. The skin of the superior part of the breast is innervated by terminal branches of the supraclavicular nerves, while the remainder of the skin is innervated by lateral and medial branches of the intercostal nerves. Denervation problems in the chest wall are very rare; they are more frequent in the skin of the medial upper arm after the division (sometimes unavoidable) of the intercostobrachial nerves, which pass through the axilla to the upper arm.
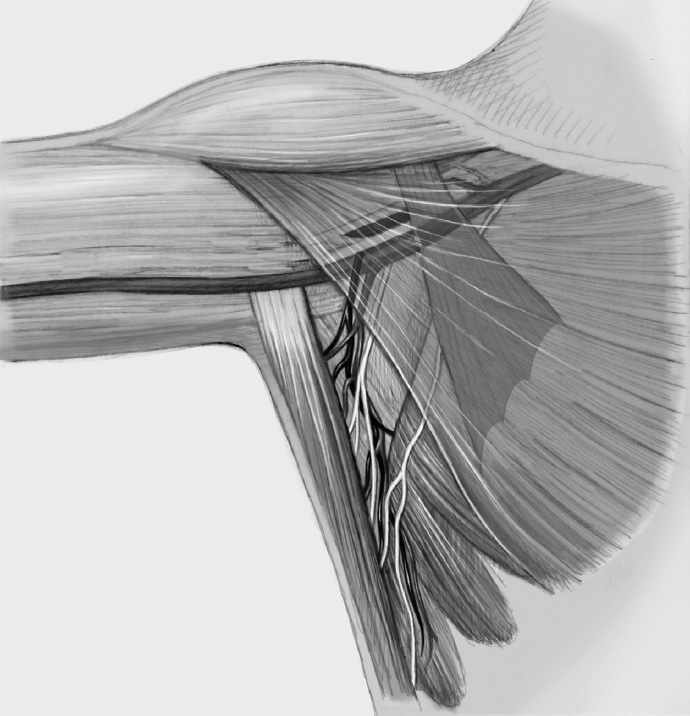
1.1.2 Axilla
The axilla is a virtual space. Its anatomical boundaries are defined as follows. Medially, the axilla is bounded by the pectoralis major and pectoralis minor muscles and the bony thorax (ribs). For anatomists, the posterior boundary is formed by the subscapularis and teres major muscles. The latissimus dorsi muscle defines the lateral boundary. The superior boundary is described (anatomically) as consisting of the outer surface of the first rib, the underside of the clavicle, and the upper border of the scapula, which basically corresponds to the shoulder joint. The inferior boundary is considered to be the collateral artery from the thoracodorsal trunk to the serratus anterior.
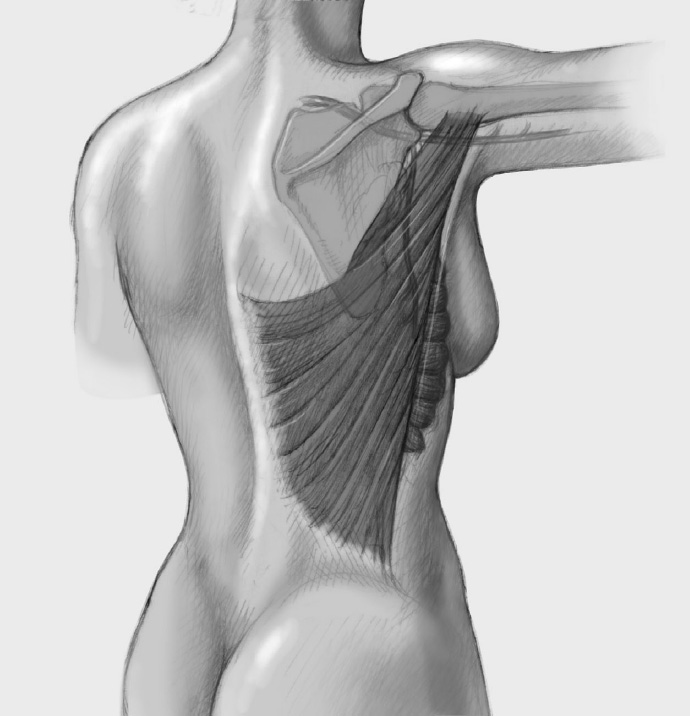
1.1.3 Back
The anatomy of the back is important for the breast surgeon when the latissimus dorsi muscle is dissected for autologous breast reconstruction. Although no major vessels run posteriorly, there are numerous perforating vascular connections between the different muscles, which can retract into muscle, rendering hemostasis difficult.
1.2 Breast Cancer
1.2.1 Fundamentals for the Surgeon
Epidemiology. Breast cancer is the most common malignant disease in women. Despite the good 5- and 10-year cure rates of up to 80% it heads the mortality statistics, ahead of colon and lung cancer. The lifetime risk of developing the disease is 7 to 9% with life expectancy of 80 years. This frequently published figure is often misunderstood. Starting from the maximum risk, this means that the risk of developing the disease becomes smaller with each year lived without breast cancer. The peak age is between 50 and 70 years. The incidence of breast cancer is increasing whereas mortality is unchanged or decreasing. Nearly one-third of all breast cancers are now smaller than 1 cm, not least as a result of extensive mammographic screening, so a large percentage of them are curable.
Risk factors. The classic risk factors are increasing age, a history of cancer in the contralateral breast, and a positive family history of premenopausal disease in a first-degree relative, when the individual risk rises to up to 30%. Nevertheless, most breast cancers are sporadic. According to current knowledge, only about 5 to 10% have a direct hereditary genetic cause, that is, mutations in the BRCA1 and BRCA2 genes. Another risk factor that may be important in screening for risk stratification in the future is the postmenopausal “dense” breast (ACR 3/4). Pregnancy and having the first child at a young age are protective factors, while breast-feeding does not influence the incidence of breast cancer. The question of the influence of oral contraceptives and oral hormone replacement therapy is particularly problematic; oral contraceptives appear to increase the incidence minimally and this effect was no longer seen 10 years after stopping the medication. The situation with hormone replacement is even harder to assess: while nonhysterectomized patients on estrogen and progesterone hormone replacement had an increased risk for breast cancer, this was not observed in hysterectomized women taking estrogen-only hormone replacement. With the negligible shifts in risk, each patient must be considered individually.
Histological types and treatment. The histological classification into invasive ductal breast cancer, the incidence of which is reported as 60 to 65% of all breast malignancies, and invasive lobular carcinoma, which accounts for about 15 to 20% of the tumors, is important for the surgeon. Medullary carcinoma (about 5% of cases), mucinous carcinoma (< 5%) and tubular carcinoma (< 1%) are much rarer. Premalignant lesions, collectively known as ductal intraepithelial neoplasia and lobular intraepithelial neoplasia (DIN, LIN), are as important as the histology of invasive carcinoma. Originally, the only defined pathological condition was ductal carcinoma in situ (DCIS), which was graded G1 to G3 depending on the degree of differentiation. It soon became clear that this is a precancer, as subsequent carcinoma rates were up to 50%. Over time it was realized that other precursor lesions could be distinguished and different nomenclature systems (DIN, WHO, DCIS) were introduced to describe the entire spectrum of ductal hyperplasia. Parallel use of these nomenclatures has led to a certain degree of confusion. Tables 1.2 to 1.4 show the nomenclatures and treatment options.
Based on data obtained in studies, nearly every larger DCIS now receives radiotherapy after breast-conserving resection. Radiotherapy can be omitted by agreement with the patient if the historically important Van Nuys prognostic index is ≤ 4, that is, if the lesion is small (< 2 cm), R0 resection is adequate (> 5–10 mm), and grading is favorable (low or medium grade). If DCIS recurs locally, simple mastectomy should be considered. Around 50% of DCIS recurrences are invasive carcinomas. DCIS with focal microinvasion is treated like an invasive ductal breast cancer.
While high-grade DIN is regarded today as precancer, the majority of lobular neoplasias (LINs) are considered to be risk markers. Lobular neoplasia is often multifocal (40–80%) and bilateral (30–70%). Ipsilateral and contralateral carcinomas occur in between 10 and 20% of patients over a period of 10 to 20 years. LIN3 is often called LCIS (lobular carcinoma in situ). The recommended treatment for LCIS (synonym: pleomorphic LIN) and DCIS is similar.
If lobular neoplasia is diagnosed on needle biopsy, open biopsy of the area in question is advisable above LIN2–3 because higher-grade preinvasive or invasive lesions are often found. If LIN1–2 is diagnosed in an excision biopsy, no further treatment is indicated regardless of resection status (R0, R1). By contrast, a LIN3/LCIS lesion should be completely resected, like DCIS. Further resection is not performed if LIN1–2 is found at the resection margin in breast-conserving surgery, but is required if an LIN3 lesion is found. Postoperative radiation after LIN/LCIS resection does not appear justified according to current knowledge.
Related posts:





Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


