Fig. 15.1
Typical cleft hand (left) and atypical cleft hand (right)
Incidence and Genetics
Birch-Jensen [5] estimated the ratio of occurrence of typical cleft hand as 1 in 90,000 births. The incidence of cleft hand among all anomalies of the upper extremity is 2.3 % of 1,476 patients in Flatt’s Iowa series [6] and 2.6 % of 943 patients in Ogino’s Sapporo series [7].
Regular autosomal dominant inheritance was evident in about 34 % of reported pedigrees. In other pedigrees, there are some different types of inheritance, such as lack of penetrance of autosomal dominant inheritance and markedly irregular dominant inheritance [8]. Vogel classified cleft hand into two types from the genetic aspect [9]. In type 1 pedigree affected members showed constant involvement of feet and had a consistent autosomal dominant inheritance. In type 2 pedigrees affected members showed variable involvement of feet and irregular inheritance.
Split hand/foot malformation (SHFM) is a congenital absence of the central rays of the hands and feet. Some authors use ectrodactyly to denote any absence deformity of the distal limbs and reserve SHFM for the typical malformation; others use ectrodactyly synonymously with SHFM [10]. The Human Genome Organization Nomenclature Committee determined in 1994 that split hand/foot malformation should be denoted SHFM. SHFM may present with syndactyly, median clefts of the hands and feet, as well as aplasia or hypoplasia of the phalanges, metacarpals, and metatarsals. In severe cases, the hands and feet have a lobster claw-like appearance [11]. However, the severity of SHFM is highly variable. In mildly affected patients, SHFM may be limited to syndactyly and several instances of non-penetrance have been documented. Clinical variability not only exists between patients, but also between limbs of a single individual [12]. The most common mode of inheritance is autosomal dominant with variable penetrance. Autosomal-recessive and X-linked forms occur more rarely and other cases of SHFM and may be caused by chromosomal deletions and duplications. Abnormality of six SHFM loci has been found [13, 14].
Difference Between Cleft Hand and Other Types of Longitudinal Deficiency
The Swanson classification, which has been adopted as the IFSSH classification, has two major categories of congenital absence of digits [15, 16]: transverse deficiency (symbrachydactyly) and longitudinal deficiency. Atypical cleft hand is best classified as transverse deficiency or symbrachydactyly. In longitudinal deficiency, the congenital absence of digits is confined to the long axis of the upper limb and is classed as ulnar deficiency, radial deficiency, or central deficiency (cleft hand). In ulnar deficiency, there are various degrees of defects of ulnar fingers, such as the hypoplastic little finger, absence of the little finger, absence of the little and ring fingers, absence of the ulnar three digital rays, and absence of the ulnar four digital rays [17]. In radial deficiency, the mildest form of the hand deformity is hypoplasia of the thenar muscles and the most severe form is total absence of the thumb [18]. Non-opposable triphalangeal thumb, which is called five-fingered hand, is also one of the types of hypoplastic thumb. In some cases, the thumb and index finger are absent. In both radial and ulna deficiencies, there may be hypoplasia or aplasia of the forearm bones, and syndactyly and central polydactyly are not often seen.
Cleft hand is central deficiency, and the severe form is the absence of central three fingers, but in some cases thumb or little finger is also absent. The forearm bones are never involved, although defect or fusion of the carpal bones in distal carpal row may be seen in severe cleft hand. There are many cases in which central polydactyly, syndactyly, and cleft hand are associated in various combinations in an affected hand or in both hands of a patient [19, 20]. These anomalies also may occur in the members of the same family in various combinations. Manske [21] reported three cleft hands and one central polydactyly in four hands of identical twins. Satake et al. [22] reported a family of a mother with bilateral cleft hands, an elder daughter with the right cleft hand and the left central polydactyly, and young daughter with the left osseous syndactyly of the middle and ring fingers associated with cross bone between the middle and index fingers. There are some cases in which the middle finger is apparently missing but on X-ray, the middle and ring fingers are fused [23]. On the other hand, Müller (1936) [24] reported cases, which seemed to be cleft hands apparently, but skeletal changes were more consistent with a polydactyly of the middle finger. This issue has not been discussed in the literature for many years. Some authors reported that there were some cases in which the middle finger appears to be missing, but the metacarpus of the middle finger is duplicated [19, 25]. It is difficult or impossible to classify these cases into central polydactyly, syndactyly, or cleft hand. By these observations, cleft hand is seen to be an anomaly closely related to central polydactyly and syndactyly [19, 20, 26–29] (Fig. 15.2). When one looks at the radiographs of patients with osseous syndactyly between the middle and ring fingers, or polydactyly of the middle finger, if the defect occurs sufficiently proximal, then an appearance of cleft hand is seen (Figs. 15.3 and 15.4a, b) [28]. These observations support the concept that a common etiological mechanism is involved in the development of central polydactyly, cleft hand, and syndactyly. They also support that a common teratogenic mechanism might be the abnormal induction of finger rays in the process of formation of the fingers in the hand plate [20, 29]. From this point of view, cleft hand is one phenotype of abnormal induction of digital rays of the hand plate in which the central fingers are missing [29].
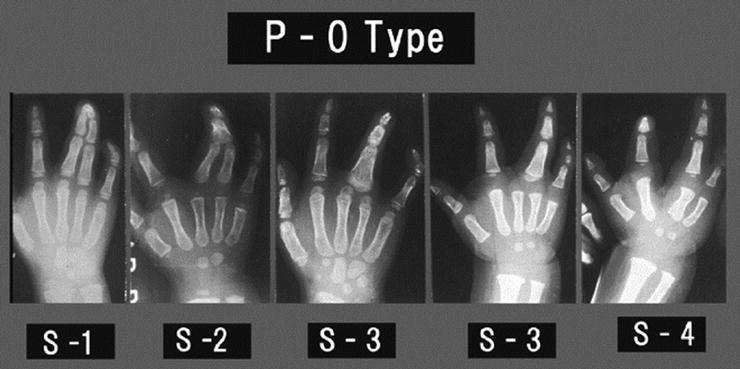
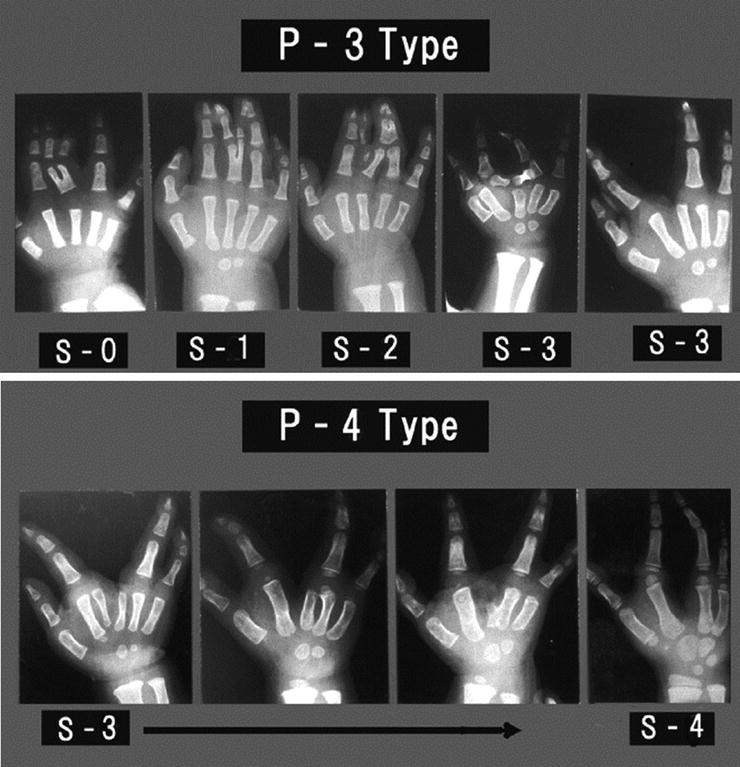
Fig. 15.2
Cleft hand formation processes from central polydactyly and/or osseous syndactyly. Reprinted with permission from Ogino T. A clinical and experimental study on teratogenic mechanism of the cleft hand, polydactyly and syndactyly. J Jpn Orthop Assoc.1979;53: 535–43
Fig. 15.3
The skeletal changes of P-0 type of anomalies in clinical cases. They seem to show that cleft hand formation proceeds from osseous syndactyly. Reprinted with permission from [28]
Fig. 15.4
(a, b) The skeletal changes of P-3 and P-4 types of polysyndactyly in clinical cases. They seem to show the cleft hand formation proceeds from central polydactylies. Reprinted with permission from [28]
Teratogenic mechanisms of formation of cleft hand and other types of longitudinal deficiency:
In order to have a better understanding of the classification, it is necessary to clarify the development of longitudinal deficiency and cleft hand. The authors developed animal models of these deformities using cleft foot as a model of cleft hand [17, 30–33]. The antineoplastic drug busulfan is given to pregnant rats, and radial deficiency and ulnar deficiency have been induced [19, 30]. The skeletal changes in busulfan-induced ulnar and radial deficiencies were similar to those of clinical cases. The critical period of ulnar deficiency in rats is about 1 day earlier than that of radial deficiency, and the critical period of radial deficiency in rats is just before limb buds appear [17, 30]. It was found that the dead mesenchymal cells were distributed evenly, and there was no localized cell deficiency inside the limb bud [33]. It was clear that the absence of digits in longitudinal deficiency was not caused by the localized deficiency of the limb bud.
A single cause affecting the limb bud in a certain receptive period of the development of the limb bud can induce central polydactyly, cleft hand, and syndactyly. When busulfan was given to rat fetuses at a critical period of these anomalies, later than that of longitudinal deficiency, cleft hand, central polydactyly, and osseous syndactyly were induced. The deformities were seen in varying stages of severity of osseous fusion. It was postulated that cleft hand was induced by the same etiology as osseous syndactyly and central polydactyly [29].
In order to examine the underlying mechanism of busulfan-induced cleft hand, central polydactyly, and syndactyly, the authors evaluated localized apoptosis by Nile Blue staining and TdT-mediated dUTP nick end labeling (TUNEL) assays in treated rat embryos [34]. The authors further evaluated the potential disruption of major developmental pathways linked to digit number and syndactyly using Fgf8, Bmp4, and Shh as markers of these pathways. In busulfan-treated embryos, there was no difference of expression of Fgf8, BMp4, and Shh in the limb bud and footplate. The early morphological changes leading to central polydactyly, syndactyly, and cleft hand or foot were growth reduction and abnormal clefts in the central parts of the footplates. The abnormal cleft was induced without precedent cell death and the cleft became deeper also without cell death [34]. If the abnormal cleft were induced on the edge of digital radiation, it might induce polydactyly or cleft hand or foot. If the abnormal cleft were induced on the interdigital tissue, it might induce syndactyly or cleft hand or foot. The authors conclude that the abnormal cleft formation without precedent cell death was an early change leading to central polydactyly, syndactyly, and cleft hand or foot by a teratogen (Fig. 15.5 [35]). Abnormal cleft formation without precedent cell death might be caused by localized inactivation of the apical ectodermal ridge (AER) in the central part of the footplate [36].
Fig. 15.5
Abnormal induction of digital rays. The early morphological changes leading to central polydactyly, syndactyly, and cleft hand were growth reduction and abnormal clefts in the central parts of the hand plates. The abnormal cleft was induced without precedent cell death and the cleft became deeper without cell death. If the abnormal cleft is induced on the edge of digital radiation, it might induce polydactyly or cleft hand. If the abnormal cleft is induced on the interdigital tissue, it might induce syndactyly or cleft hand. Reprinted with permission from Ogino T. Teratogenic mechanisms of congenital absence of digits. Locomotor System: Advances in Research, Diagnosis and Therapy 2011;18:173-93
Results of recent studies on split-hand/split-foot malformation (SHFM) using murine Dactylaplasia mutant (Dac) have shown that the central segment of the AER degenerates, leaving the anterior and posterior segments intact [37]. From this observation, it was suggested that localized failure of ridge maintenance activity was the fundamental developmental defect in Dac and it might also be suggested in SHFM [10]. Therefore, the teratogenic mechanism of formation of cleft hand/foot is the same both in drug-induced cleft hand in rats and in mutant mice with cleft hand.
Position of Cleft Hand in Japanese Modification of Swanson’s Classification
Based on the clinical and experimental studies, the author modified the IFSSH classification in 1986 and added a fourth new category—abnormal induction of digital rays [38, 39]. In IFSSH classification, brachysyndactyly is classified into undergrowth and transverse deficiency into failure of formation of parts, and there is no item of cleft of the palm. However, analysis of clinical cases showed that brachysyndactyly, atypical cleft hand, or transverse deficiency seemed to be morphological variants of symbrachydactyly [2, 3]. Therefore, these deformities are included in a similar concept to transverse deficiency in failure of formation of parts in modified classification.
On the other hand, central polydactyly is classified as duplication, syndactyly as failure of differentiation of parts and typical cleft hand as failure of formation of parts in the IFSSH classification. However, these congenital deformities appear when the same teratogenic factor acts on embryo at the same developmental period. Because they have a similar causation, central deficiency, osseous syndactyly, central polydactyly, and cleft of the palm may be grouped together, and are included in the same category of abnormal induction of digital rays in modified classification [38, 39] (Table 15.1). Recent literature has reported that chromosome abnormality and also abnormalities of the positional gene may cause these anomalies [40–42].
Table 15.1
The Japanese Society for Surgery of the Hand Modification of the IFSSH classification revised by Ogino T. (2013)
I. Failure of formation of parts (arrest of development) |
A. Transverse deficiency |
1. Peripheral hypoplasia type |
2. Short webbed finger type |
3. Tetradactyly type |
4. Tridactyly type |
5. Didactyly type |
6. Monodactyly type |
7. Adactyly type |
8. Metacarpal type |
9. Carpal type |
10. Wrist type |
11. Forearm type |
12. Above elbow type |
B. Longitudinal deficiencies |
1. Radial deficiencies: |
(a) Dysplasia of the radius |
(b) Deformities of the hand |
(c) Dysplasia of the elbow |
2. Ulnar deficiencies: |
(a) Dysplasia of the ulna |
(b) Deformities of the hand |
(c) Dysplasia of the elbow |
C. Phocomelia |
D. Tendon or muscle dysplasia |
E. Nail dysplasia |
1. Aplapsia/hypoplasia of the nail |
2. Nail defect with brachytelephalangia |
II. Failure of differentiation of parts |
A. Synostosis |
B. Radial head dislocation |
C. Symphalangism |
D. Contracture |
1. Soft tissue |
(a) Arthrogryposis multiplex |
(b) Webbed elbow (pterygium cubitale) |
(c) Clasped thumb |
(d) Windblown hand |
(e) Camptodactyly |
(f) Aberrant muscles |
(g) Nail deformities: |
(i) Nail deformity with clinodactyly |
(ii) Nail deformity with hypoplasia of the distal phalanx |
(iii) Nail deformity or palmar nail with hypoplastic digit and symphalangism |
2. Bone |
(a) Kirner deformity |
(b) Delta bone (longitudinal epiphyseal brancket) |
(c) Madelung deformity |
3. Others |
E. Tumorous conditions |
III. Duplication |
A. Thumb polydactyly |
B. Central polydactyly (it should be category IV) |
C. Polydactyly of little finger |
D. Opposable triphalangeal thumb |
E. Other hyperphalangism |
F. Mirror hand |
G. Dorsal and palmar duplication |
1. Double dorsal limited in the digit |
2. Double dorsal including the hand |
3. Double palmar limited in the digit |
4. Double palmar including the hand |
IV. Abnormal induction of digital rays |
A. Soft tissue: |
(1) Cutaneous syndactyly, (2) Cleft of the palm |
B. Bone: |
(1) Osseous syndactyly, (2) Central polydactyly, (3) Absence of central finger ray(s), (4) Triphalangeal thumb with cleft hand |
C. Ulnar cleft hand: |
(1) Cleft of the fourth web space: (a) with absent ring finger, (b) without absent ring finger |
(2) Stiff finger: (a) symphalangism; PIP and/or DIP joint, (b) partial ankylosis; PIP and/or DIP joint |
(3) Nail deformity: (a) clam nail, (b) claw nail, (c) circumferential nail |
D. Abnormal induction of digital rays with hypoplastic hand: |
(1) polydactyly, (2) syndactyly, (3) central finger absence |
V. Overgrowth |
A. Macrodactyly |
B. Hemihypertrophy |
VI. Undergrowth |
A. Microcheiria (hypoplastic hand) |
B. Brachydactyly |
C. Clinodactyly |
VII. Constriction band syndrome |
(1) Constriction ring, (2) Lymphedema, (3) Acrosyndactyly, (4) Amputation type |
VIII. Generalized skeletal abnormalities and a part of syndrome |
IX. Others (including unclassifiable cases) |
The Japanese Society for Surgery of the Hand adopted our modification of the IFSSH classification in 1996 and it is now called the Japanese modification [43]. As a skin manifestation, there are syndactyly and cleft of the palm. As a skeletal manifestation, there are osseous syndactyly, central polydactyly, and absence of central finger rays (cleft hand), and triphalangeal thumb associated with cleft hand.
The author reviewed his own cases of abnormal induction of digital rays affecting 186 hands in 125 patients. Eighty-three cases were male and 42 female. The right side was affected in 47 cases, the left in 17 cases, and both in 61 cases. The deformities of the affected hand were expressed by the combination of cleft on the palm, cutaneous syndactyly, osseous syndactyly, absence of central digit(s), which is absence of all phalanges of the digital ray(s), and central polydactyly. Of the 186 abnormal hands, a single deformity appeared in 86 hands: cutaneous syndactyly alone in 65 hands, osseous syndactyly alone in 17 hands, and cleft on the palm without absence of digit in 4 hands. In 100 hands, multiple deformities appeared in the same hand of a patient. Polydactyly and syndactyly were present in the same hand in 16 cases; a combination of cleft on the palm and syndactyly in six cases; a cleft, polydactyly, and syndactyly in one case; an absence of central digit and cleft on the palm in 37 cases; an absence of central digit, cleft on the palm, and syndactyly in 34 cases; an absence of central digit, cleft on the palm, and polydactyly in one case; and an absence of central digit, a cleft on the palm, central polydactyly, and syndactyly in five cases. In these cases there were eight hands with triphalangeal thumb associated with absence of the index finger, and there was one hand with a floating little finger. In bilaterally affected cases, same type of expression was evident in both the right and left hands in 47 cases. Different abnormalities occurred in the right and left hands in 14 cases. Hand deformities were expressed by combinations of cutaneous syndactyly, cleft on the palm, osseous syndactyly, central polydactyly, absence of central digit, and triphalangeal thumb with cleft hand with absence of the index finger. This review suggested that abnormal induction of digital rays may explain simultaneous occurrence of differing abnormalities within the same hand. The concept of abnormal induction of digital rays seemed useful for classification of congenital hand differences.
In this chapter, the author has revised the Japanese modification of the IFSSH (see Table 15.1). The abnormality of the nail has not been clearly classified, and the abnormalities of the dorso-ventral plane of the hand also have not been described in the previous Japanese modification. First, “E. Nail dysplasia” in I. Failure of formation of parts was subdivided into:
1.
Aplapsia/hypoplasia of the nail.
2.
Nail defect with brachytelephalangia.
3.
Others.
Secondly, II. Failure of differentiation of parts had (g) Nail deformities added as a sub-category, and it is sub-classified into:
1.
Nail deformity with clinodactyly
2.
Nail deformity with hypoplasia of the distal phalanx
3.
Nail deformity or palmar nail with hypoplastic digit and symphalangism (This is the same deformity observed in “ulnar cleft hand: VI. C”)
4.
Others
Thirdly, III. Duplication had “G. dorsal and palmar duplication” added and is sub-classified into:
1.
Double dorsal limited in the digit
2.
Double dorsal including the hand
3.
Double palmar limited in the digit
4.
Double palmar including the hand
5.
Others
Fourthly, the categories IV. Abnormal induction of digital rays added the categories:
C. Abnormal induction of digital rays, ulnar cleft hand
D. Abnormal induction of digital rays with hypoplastic hand
After these changes, it becomes easier to differentiate true typical cleft hand described by Barsky and other cleft hand-like deformities.
Clinical Characteristics
Blauth and Falliner’s reported incidence of cleft hand: they found bilateral involvement in 50 %, and in unilateral involvement, the ratio of right hand to left hand is 60 to 40 %. The ratio of male to female is 60 to 40 % [44]. In approximately one out of three cases of cleft hand there was associated cleft foot.
Defect of the central finger rays varies [45]: there are hands with deep cleft formation on the palm without absence of the finger rays. This is a type of central deficiency, and therefore a form of cleft hand (Type 0) [46]. There are cleft hands with one finger absent, two fingers absent, three fingers absent, or four digits absent. In one finger absence type (Type 1), the middle finger is most commonly absent. In that case, the ring finger often will have camptodactyly. This deformity is not actually true camptodactyly, but a claw finger deformity due to abnormal lumbrical or interosseus muscles. Most often, the affected ring finger has no joint contracture when the child is young. If the metacarpophalangeal joint of the ring finger is passively flexed to neutral, the patient can actively extend the PIP and DIP joints of the affected finger.
Some cases with mild excessive cleft and absence of the middle finger will have normal looking third metacarpal bone radiologically. However, in some cases the third metacarpal bone deviates ulnarly and has a common MP joint with the fourth metacarpal bone and proximal phalanx of the ring finger. Alternately, third metacarpal bone will deviate radially and have a common MP joint with the second metacarpal bone and proximal phalanx of the index finger. In the former case, the ring finger is wider than normal and in the later case the index finger is wider than normal. When middle finger ray including the third metacarpal is absent, the cleft is deeper than usual. The deeper the cleft is, the more often syndactyly of the first web space and the fourth web space occur. In some rare cases of deep cleft, hypoplasia of the little finger, or the fusion of the fourth and fifth metacarpals, is seen. In Type 1 cleft hand, the index finger or ring finger also may be absent [47, 48]. When the index finger is absent, the thumb is often triphalangeal and will deviate radially, in contrast to most triphalangeal thumbs, which deviate ulnarly. A “Y” shaped second metacarpal bone between the thumb and middle finger, or two thumb metacarpal bones may be seen on X-ray. When the ring finger is absent, the little finger is small and stiff, and this may be called “ulnar cleft hand.” When the finger is not absent and the cleft is in the forth web apace, this is often associated with stiffness of the IP joints, palmar nail, and the dorsal skin on the palmar side of the little finger. This may be called “double dorsal deformity of the finger.” The etiology of this deformity is considered to be different from other types of cleft hand (see below).
In two-finger absence type (Type 2), the index and middle fingers are absent more commonly than the middle and ring fingers. When the index and middle fingers are absent, the thumb is usually triphalangeal. In three-finger absence type (Type 3), if the thumb is opposable then pinch is possible between the thumb and the little finger. If the thumb is in the plane of the hand however, pinch between the thumb and little finger is impossible [49]. In four-digit absence type (Type 4), the radial four digits are absent in most commonly, but very rarely the ulnar four digits will be absent and only the thumb remains [46]. In radial-four-digits absence type, the metacarpals of the thumb and affected fingers are usually only partially absent or not involved.
A cross bone is a transverse or oblique bone lying in the base of the cleft. It is regarded as the displaced remnant of the metacarpal or proximal phalanx of the missing digit and it bridges between the end of the metacarpal bones of the missing digit and the proximal phalanx, MP joint, or the metacarpal bone of the adjacent finger. There may be two cross bones which might be duplicated proximal phalanges of the missing digit and are located between missing digit and adjacent fingers between the end of the metacarpal bones of the missing digit and the proximal phalanx, MP joint, or the metacarpal bone of the adjacent finger. There may be two cross bones, which might be duplicated proximal phalanges of the missing digit, and are located between missing digit and adjacent fingers. There may be solid bone union or cartilaginous continuity between the cross bone and the proximal phalanx of the adjacent finger in the skeletally immature patient. In some cases, the proximal phalanx of the adjacent finger will have a deltaphalanx (longitudinal epiphyseal bracket). X-ray films may show, two metacarpals supporting one digit, side-to-side fusion of the neighboring metacarpals, broad metacarpals, or duplicated metacarpals.
Surgical Classification of the Cleft Hand
Saito et al. [45] classified typical cleft hand into four types on the basis of the number of defective finger rays:
Type 1: deep cleft formation on the palm without missing finger.Related posts:
 Anesthesia Concerns in Congenital Anomalies of the Upper Extremity
General Skeletal Disorders
Anesthesia Concerns in Congenital Anomalies of the Upper Extremity
General Skeletal Disorders
 Therapy Management of Children with Congenital Anomalies of the Upper Extremity
Therapy Management of Children with Congenital Anomalies of the Upper Extremity
 Physical Medicine and Rehabilitation Management of Children with Congenital Anomalies of the Upper Extremity
Physical Medicine and Rehabilitation Management of Children with Congenital Anomalies of the Upper Extremity
 Ulnar Polydactyly and Ulnar Dimelia
Ulnar Polydactyly and Ulnar Dimelia
 Arthrogryposis
Arthrogryposis

Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


