div class=”ChapterContextInformation”>
13. A Young Man with Generalized Pigmentation
Keywords
Vitamin B12Diffuse hyperpigmentationGlossitisMegaloblastic anemiaPeripheral neuropathySubacute combined degeneration of the spinal cord
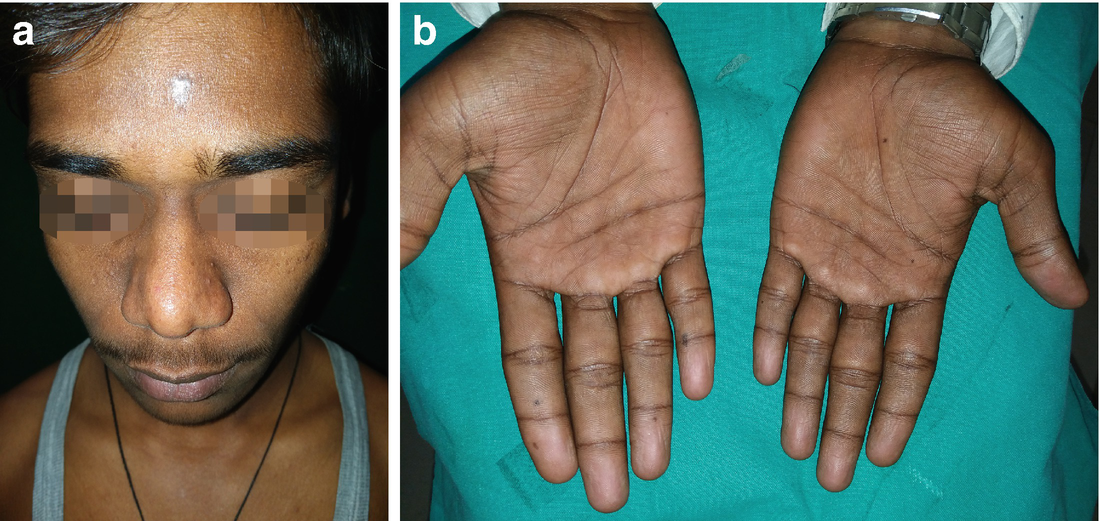
Pigmentation of the face in vitamin B12 deficiency

Pigmentation of the palms in vitamin B12 deficiency. Note pigmentation of palmar creases

Mucosal pigmentation in vitamin B12 deficiency
- 1.
Addison’s disease
- 2.
Vitamin B12 deficiency
- 3.
Cushing’s Disease
- 4.
Laugier-Hunziker Syndrome
Diagnosis
Vitamin B12 deficiency
Discussion
Diffuse hyperpigmentation may have a systemic cause of which vitamin B12 deficiency is one of the rare causes. The body reserve of vitamin B12 ranges from 2000 to 3000 μg which doesn’t need replenishment for the next 3–4 years and hence, vitamin B12 deficiency does not manifest until and unless deficiency persists for a long time [1]. Common cause of vitamin B 12 deficiency is malabsorption, usually due to pernicious anemia or gastric resection and rarely, due to inadequate intake [2]. Inadequate intake almost exclusively occurs in strict vegetarians as vitamin B12 is naturally found in animal products like meat, eggs, fish, poultry, milk and milk products [3].
Vitamin B12 is needed as a cofactor for enzymes like methionine synthase (cytoplasmic) and methylmalonyl coenzyme A mutase (mitochondrial). Also, Cobalamin is essential for DNA synthesis, haematopoiesis and myelination. As a result, vitamin B12 deficiency presents with different combinations of neurological manifestations (peripheral neuropathy, subacute combined degeneration of the spinal cord, ataxia), hematological changes (megaloblastic anemia and pancytopenia), psychiatric (psychosis, depression, mania and dementia), gastrointestinal (diarrhea), dermatologic (discoloration of skin, hair and nails), cardiovascular manifestations (thrombosis, myocardial infarction, stroke and syncope), and optic atrophy [4]. Neurological manifestations are common presenting features and the commonest neurological signs are diminished vibration sense and proprioception in the legs and can include impaired distal cutaneous sensation. Limb reflexes may be exaggerated, diminished, or absent depending on the relative involvement of the cord. Lateral column signs of a spastic paraparesis may occur, accompanied by autonomic bladder, bowel, or sexual symptoms [5].
Cutaneous manifestations associated with vitamin B12 deficiency are characteristic and include skin hyperpigmentation, angular stomatitis, and hair changes like premature canitis. Most common type of cutaneous manifestation is reversible brown to black pigmentation over the dorsum of hands and feet (predominantly over knuckles and interphalangeal joints; and palmar creases) and over pressure points like elbows, knees and malleoli. Other sites of pigmentation include sun exposed areas, genital, perineum, and umbilicus, resembling addisonian type of pigmentation. Rarely, hyperpigmentation of skin may be the only presenting manifestation of vitamin B12 deficiency and awareness of this condition may lead to early diagnosis [6]. Hyperpigmentation in vitamin B12 deficiency is related to depletion of glutathione which increases the activity of tyrosinase and increases eumelanogenesis, resulting clinically in hyperpigmentation. Ultraviolet rays cause further depletion of intracellular glutathione, thereby accentuating the pigmentation in sun-exposed areas. Mucosal manifestation may vary from mucosal pigmentation, mucositis, glossodynia to recurrent ulcerations. The classic manifestation of mucous involvement is Hunter glossitis/Moeller glossitis (25% cases) that has an early inflammatory stage presenting as red beefy tongue and a late atrophic stage causing atrophy of papillae [5].
It is important to note that folate deficiency may present with similar melanosis of skin and neurological manifestations. Sometimes, folate and vitamin B12 deficiencies may co-exist in same patient and it is prudent to supplement both when deficiency of either nutrient is suspected. Both Folate and vitamin B12 have essential roles in methionine synthase mediated conversion of homocysteine to methionine, which is essential for nucleotide synthesis and genomic and non-genomic methylation Folate deficiency manifests as fatigue, weakness, headaches, difficulty concentrating, palpitations and diarrhoea similar to vitamin B12 deficiency. In the early stages, the tongue may be red and painful leading to a smooth shiny surface in the chronic stages of deficiency. The reported neuropsychiatric effects of folate deficiency are remarkably similar to those described for vitamin B12 deficiency [7].
The common differential diagnoses include Addison’s disease, Cushing’s disease and Laugier-Hunziker syndrome. Addison’s disease results from adrenal insufficiency caused by a defect anywhere in the hypothalamic-pituitary-adrenal axis. Patients present with generalized hyperpigmentation and the diagnosis is confirmed by estimating serum electrolytes and serum 8 a.m. cortisol level. Cushing’s disease is caused by prolonged exposure to elevated levels of glucocorticoids (endogenous or exogenous). Patients develop proximal muscle weakness, easy bruising, weight gain, hirsutism, and, in children, growth retardation, hypertension, osteopenia, diabetes mellitus, and impaired immune function. Addisonian pattern of pigmentation is noted in 10% patients. Besides cutaneous and systemic changes nails shows longitudinal pigmented bands and hair is often dark. The diagnosis of requires demonstration of inappropriately high level of cortisol in the serum or urine and screening tests include midnight serum or salivary cortisol, 24-h urine free cortisol and low dose dexamethasone suppression test. Laugier-Hunziker syndrome is an acquired pigmentary disorder presenting with hyperpigmented macules of the lips and buccal mucosa with associated longitudinal melanonychia, without any systemic features [5].
A diagnosis of vitamin B12 deficiency is often overlooked in its early stages because these signs are not specific to vitamin B12 deficiency alone. Vitamin B12 deficiency results in megaloblastic anemia and pancytopenia- so patients have low hemoglobin, low total leucocyte count and reticulocyte count, but high mean corpuscular volume. Vitamin B12 level estimation is diagnostic. Anti parietal cell antibody titre may be done to identify patients of autoimmune gastritis and pernicious anaemia who are deficient in intrinsic factor, essential for absorption of vitamin B12 [5].
Related posts:
 Years Old Male with Multiple Hyperpigmented Macules on Trunk
Years Old Male with Multiple Hyperpigmented Macules on Trunk
 Gray Pigmented Macule on Right Cheek
Gray Pigmented Macule on Right Cheek
 6 Years Old Male with Multiple Black Spots on Face
6 Years Old Male with Multiple Black Spots on Face
 of Skin Pigmentation on Feet in a Female
of Skin Pigmentation on Feet in a Female
 Young Man with Hypopigmented Macules on Trunk and Multiple Shiny Nodules Over Face
Young Man with Hypopigmented Macules on Trunk and Multiple Shiny Nodules Over Face
 Young Boy with Generalized Hyperpigmentation
Young Boy with Generalized Hyperpigmentation
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


