div class=”ChapterContextInformation”>
18. Loss of Skin Pigmentation on Feet in a Female
Keywords
Chemical leukodermaMonobenzylether of hydroquinoneTyrosinaseConfetti- 1.
Vitiligo
- 2.
Chemical leukoderma
- 3.
Nevus depigmentosus
- 4.
Discoid lupus erythematosus

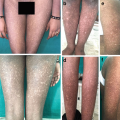
Sharply defined, depigmented macules on dorsum of feet confined to the site in contact with the strap of slipper (‘v’ shaped configuration) (Courtesy: Dr. Sunil K. Kothiwala)
Diagnosis
Chemical leukoderma
Discussion
Chemical leukoderma is an acquired cause of loss of skin pigmentation induced by repeated, cutaneous exposure to specific melanocytotoxic chemical agents [1]. Ingestion and inhalation may also lead to this condition. Such agents can be occupational (industrial chemicals) or non-occupational (household products) [1]. The most common culprits are aromatic and aliphatic derivatives of phenols and catechol, and sulfhydryl compounds. Monobenzylether of hydroquinone (MBEH) is the first identified chemical to cause leukoderma. Other such agents are mercurial, arsenic, benzoyl peroxide, tretinoin, cinnamic aldehyde, paraphenylene diamine (PPD, in hair dye and rubber gloves) and many more [1]. In genetically susceptible persons, such chemicals, on repeated applications, can lead to the loss of pigmentation at the site of contact and sometimes, at remote site [2].
The pathogenesis of chemical leukoderma is different from vitiligo. It includes TRAIL (tumor necrosis factor related apoptosis-inducing ligands) induced apoptosis of melanocytes, inhibition of melanogenesis by blocking tyrosinase by phenolic compounds (structurally similar to tyrosine) and oxidative damage to melanocytes mediated by tyrosinase-related protein-1(Tyrp1) [3]. In genetically susceptible individuals, melanocytes are unable to withstand the Tyrp1 mediated oxidative stress resulting in death.
The onset delay varies from months to years depending upon the dose and frequency of the exposure. All age groups may be affected, although adults have a much higher incidence. Any body site may be affected. In occupational settings, the hands and forearms are commonly involved. In non-occupational cases, the scalp and face are often affected. The forehead, hands, and feet are affected in Indian patients owing to the use of “bindi” and “alta” [1]. Non-contact distant sites may also get involved in some cases due to autotransfer by hands or by lymphatic or hematogenous spread in case of systemic ingestion. Clinically, depigmented macules of chemical leukoderma appear similar to that seen in vitiligo. However, lesions are usually off-white in color and may not be sharply defined as seen in vitiligo [1]. Wood’s lamp examination may be helpful to enhance the indistinct macules in many cases. Contact dermatitis is not a prerequisite for the development of chemical leukoderma and depigmentation is unlikely to occur in most of the cases of contact dermatitis. However in some cases, the same offending chemical may lead to contact dermatitis as well as chemical leukoderma, therefore itching may be an associated complaint. In most of the cases, numerous acquired round/oval confetti-like or pea-sized macules may also be seen [1]. The spreading pattern may also be helpful. A history of gradual coalescence of small discrete macules rather than the development of large macules with perifollicular sparing suggests chemical leukoderma. The presence of small confetti-like macules depends on the time of the clinical observation because they have a tendency to confluence. Histopathology in chemical leukoderma is not specific. It reveals lichenoid mononuclear infiltration in dermis and reduced/absent melanocytes.
Vitiligo is an acquired and autoimmune pigmentary disorder, characterized by well-demarcated, chalky-white macules with or without scalloped hyperpigmented border. Although it is not easy to reliably differentiate vitiligo from chemical leukoderma, trichrome morphology, koebnerization, leukotrichia, negative history of repeated exposure to a suspected chemical and lesional progression point in favour of vitiligo [1]. On histopathology in active lesions, increased numbers of Langerhans cells in epidermis and lymphocytes in the superficial dermis also support the diagnosis of vitiligo. A carefully done patch testing with suitable vehicles and fully informed consent may be useful to rule out vitiligo.
Nevus depigmentosus is a form of cutaneous mosaicism characterized by congenital, non-progressive cutaneous hypomelanosis due to dysfunctional melanocytes and abnormal melanosomes. It usually presents at birth as a solitary, circumscribed, hypopigmented macule with serrated border (splashed paint appearance) mostly on trunk, neck and proximal limbs. It remains unchanged throughout life after body’s maximum physical growth [4].
Discoid lupus erythematosus (DLE) is a chronic form of cutaneous lupus that typically presents with depigmented scaly plaques with central atrophy and hyperpigmented rim. Central scarring is usually not seen in early lesions. The photoexposed sites are commonly involved and females are more prone due to its autoimmune origin. The characteristic histopathologic findings (follicular plugging, dermal perivascular and periadnexal lymphohistiocytic infiltrates, basal layer degeneration, apoptotic keratinocytes, thickened basement membrane) can reliably differentiate DLE from other disorders of depigmentation in case of any suspicion.
Avoidance of the causative agent may lead to spontaneous gradual repigmentation in months, but treatments commonly used in vitiligo such as narrow-band ultraviolet B (UVB) phototherapy, psoralen plus ultraviolet A (PUVA) photochemotherapy, or topical immunosuppressants, often are necessary [3].
Key Points
Chemical leukoderma is typically localized to the site of application and may also spread to remote, unexposed locations.
History of repeated cutaneous or systemic exposure to a chemical is present.
Phenols and catechol derivatives are most common melanocytotoxic agents.
Contact dermatitis is not a prerequisite for the development of chemical leukoderma.
Confetti-like macules are characteristically present in most of the cases of leukoderma.
Spontaneous repigmentation is evident in many cases after avoidance of the offending chemical/s.
Related posts:
 Years Old Male with Multiple Hyperpigmented Macules on Trunk
Years Old Male with Multiple Hyperpigmented Macules on Trunk
 Gray Pigmented Macule on Right Cheek
Gray Pigmented Macule on Right Cheek
 6 Years Old Male with Multiple Black Spots on Face
6 Years Old Male with Multiple Black Spots on Face
 Young Female with Generalized Mottled Pigmentation
Young Female with Generalized Mottled Pigmentation
 Young Boy with Generalized Hyperpigmentation
Young Boy with Generalized Hyperpigmentation
 Female with Freckles Like Pigmentation on Face and Extremities
Female with Freckles Like Pigmentation on Face and Extremities
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


