div class=”ChapterContextInformation”>
6. What You Need to Know About Hair Transplantation
Keywords
Hair transplant surgeryMale pattern baldness (MPB)Female pattern hair loss (FPHL)Follicular unit excision (FUE)Safe donor area (SDA)Strip (elliptical) harvestFollicular unit transplantation (FUT)Female hair restorationBody hair transplantation (BHT)Platelet-rich plasma (PRP)Platelet-erythrocyte-rich plasma plus ACell (PeRP + ACell)Hair restorationPhysicians in different specialties are sometimes asked questions about hair transplantation (HT). Patients are looking for answers to help decide if they are good candidates, where to go, what area to treat surgically, and what method is best to achieve natural long-lasting results. This chapter is intended to educate and inform physicians so that they can provide patients with informed answers to these questions. For further reading, it is helpful to refer to the textbook used by most hair transplant surgeons [1]. Within the field of hair restoration surgery, there are differing opinions regarding many issues. When possible, the author will also attempt to outline differing points of view, provided they are still sound and reasonable.
Overview of Terminology
Recipient area – the area of alopecia or future alopecia that is to be treated during surgery.
Follicular unit (FU) – one to five hairs with associated sebaceous glands that are contained in a grouping bound by adventitial tissue, evident from the skin surface to the insertion of the AP muscle [2].
Follicular family – two FU that are so closely associated that they can be transplanted as one graft and placed into one recipient site incision.
Follicular unit excision (FUE) – harvest method using a small punch to excise one follicular unit at a time from the donor area. Each area of extraction leaves behind a small punctuate scar.
Elliptical excision/strip – harvest method in which an elliptical excision is used to remove the donor hair. The tissue is then divided under microscopic dissection to produce the follicular units. The excision is surgically closed and leaves a small linear scar.
Donor area – the region with relatively permanent hair, from which the hair is removed for transplantation.
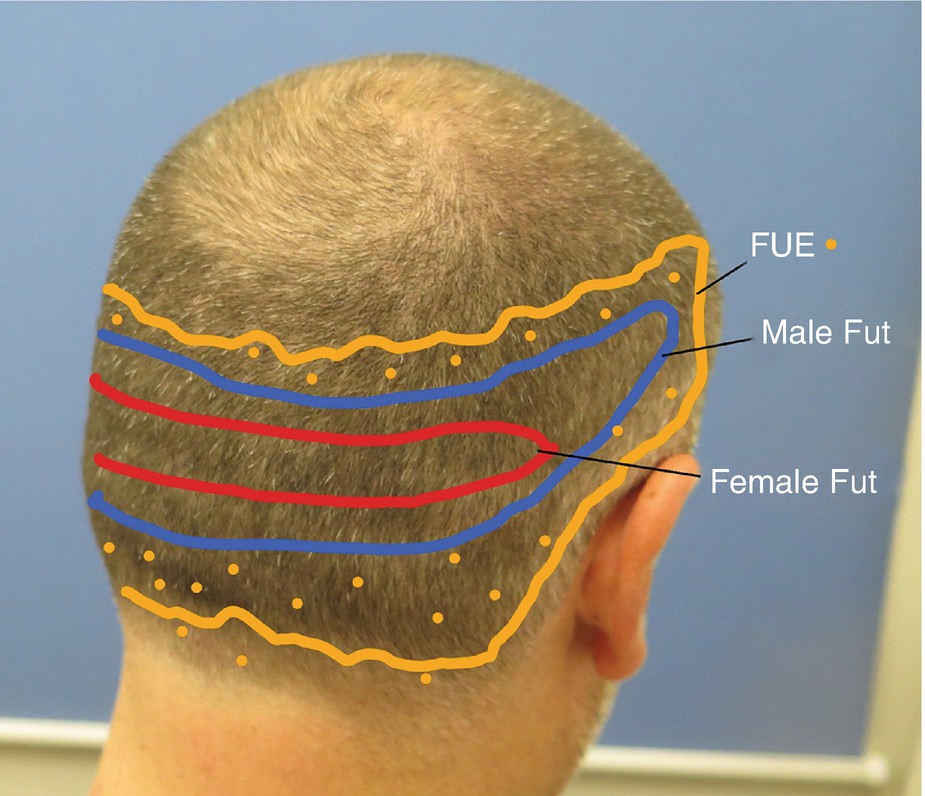
Safe donor area – also called by FUE surgeons the “major region.” This is the safest region in the donor area for harvesting grafts. Hairs in this area are the most permanent on the scalp. FUE surgeons also define a minor region which includes hairs closer to the nape of the neck and other areas superior and inferior to the major region. Hairs in these areas will last for less of the patient’s lifetime [3].
FUE punch terminology – there is an entire chapter sometimes dedicated to this topic. In brief, there are sharp, dull, and hybrid punches. Excision is achieved with rotation, oscillation, and/or vibration. The punch diameter may be defined according to internal diameter that reflects the size of the tissue removed or the external diameter that reflects the size of the defect left behind in the skin (the scar) [4].
Candidacy
- 1.
Patients with active dermatopathology causing alopecia – including scarring and nonscarring alopecia. Most importantly, LPP and FFA may recur at any time and would affect the transplanted as well as pre-existing hair [5].
- 2.
Patients with nonscarring alopecias like alopecia areata, active telogen effluvium, or anagen effluvium should ideally wait for resolution. The main reason for excluding surgery for patients with nonscarring alopecia is that it may be unnecessary. The second reason is that it is impossible to be accurate in surgical planning when the doctor does not know what the patient will look like after recovery from their temporary hair loss. Third, it may affect the donor area, and if the donor is harvested using a strip method, some tissue with dormant hair follicles may be discarded as alopecic.
- 3.
Patients with very limited donor hair and a large alopecic recipient area and unrealistic expectations. The author adds this third requirement because even patients with a poor donor:recipient ratio may find that hair transplantation at least produces enough hair that certain styling options can be used to cover untreated areas [6].
- 4.
Patients with diffuse unpatterned hair loss including the region normally used for donor harvest.
- 5.
Patients on clopidogrel who are unable to stop use for the surgery.
Surgical Planning of the Recipient Area
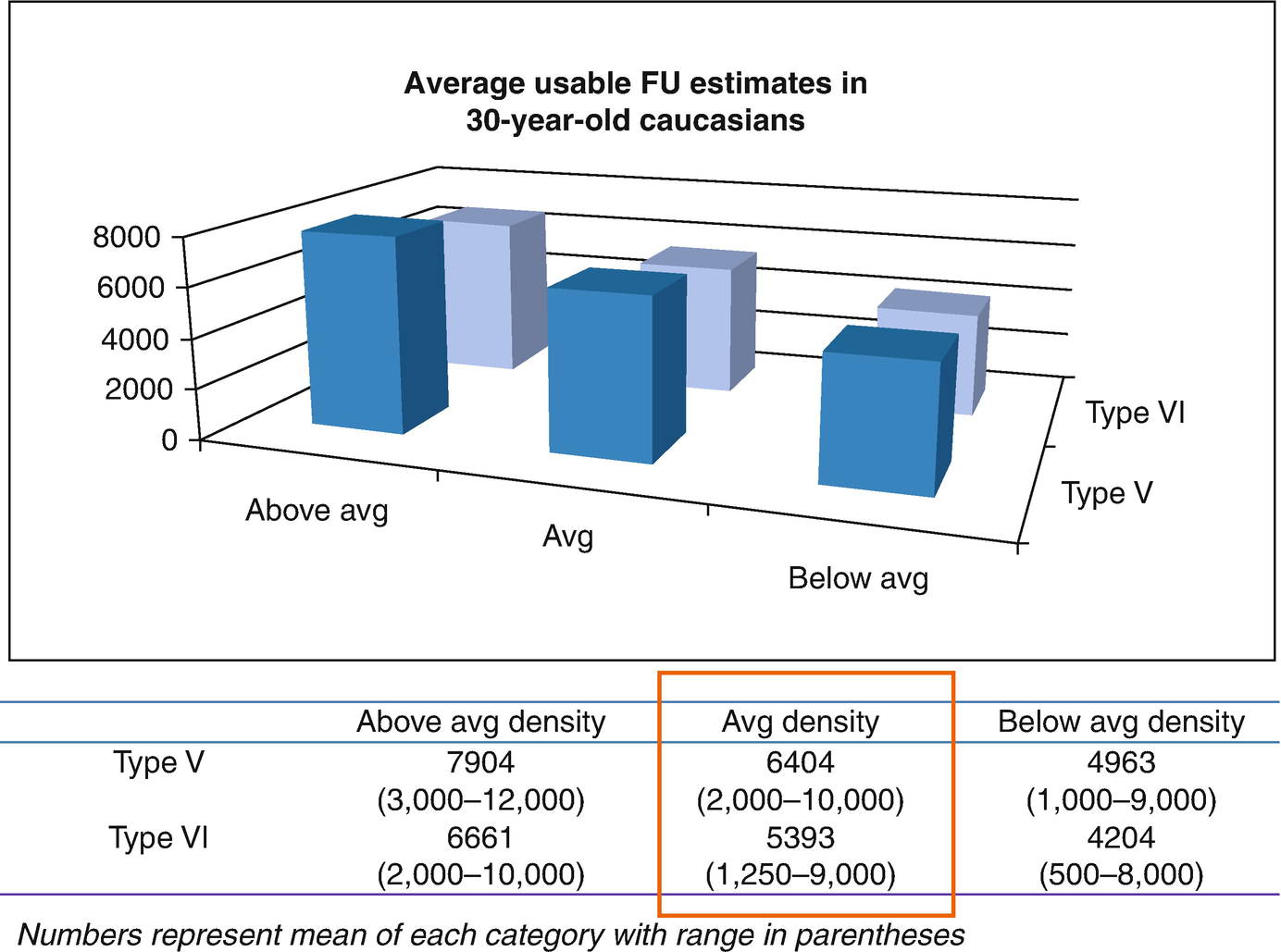
A group of 39 expert hair restoration surgeons (with a combined 900 years of expertise) were asked to give their estimate of the number of likely permanent donor hairs that were available over the lifetime of patients in various scenarios. This figure shows the results of their answers and highlights the importance of using available donor hair very judiciously. (Reprinted with permission from Unger et al. [6])
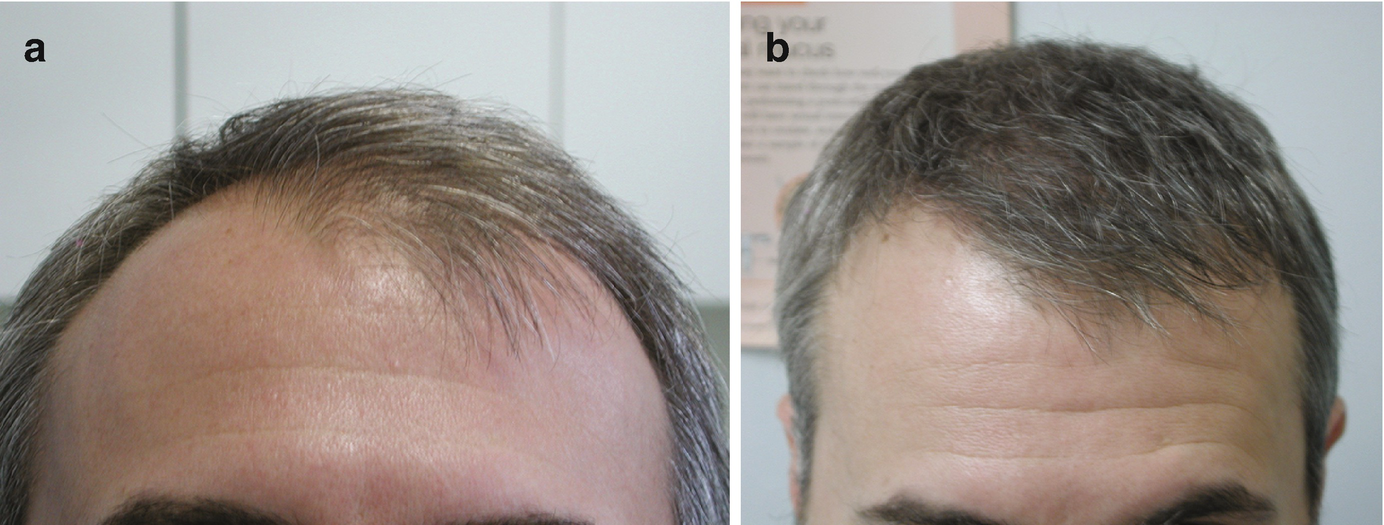
(a) A male patient with fairly advanced hair loss prior to surgery. (b) The same patient 6 months after surgery. This illustrates our ability to cover a larger recipient area with a lower number of follicular units per square cm (FU/cm2) and still achieve good cosmetic density
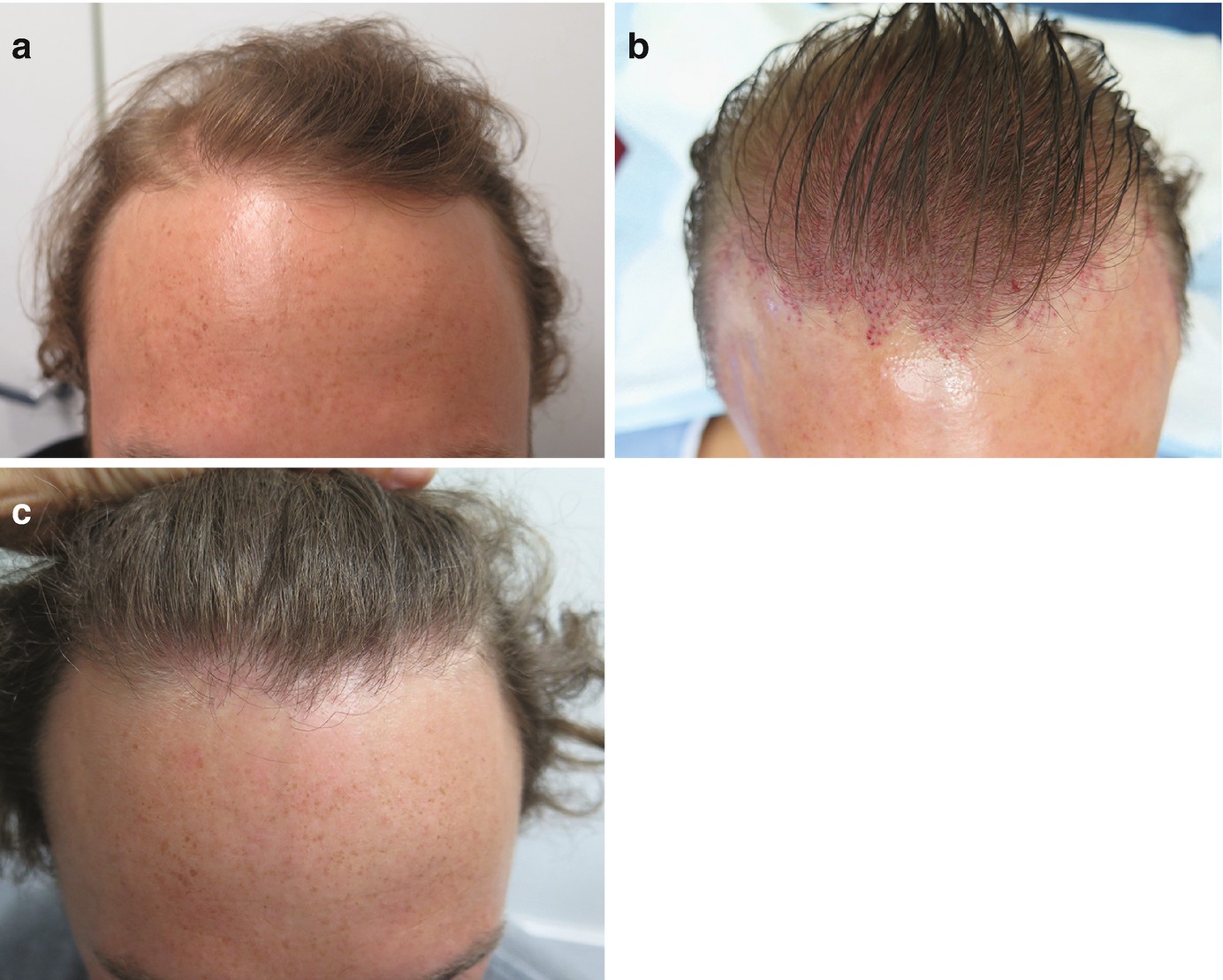
(a) A young patient before surgery with a significant amount of pre-existing hair that will be lost in the future. (b) The same patient showing the pattern of the sites in the recipient area. (c) One year after the surgery. There is a lower density “feathered” hairline and density increases posteriorly. Over 50% of grafts were used in areas with existing hair. The density was further increased in those areas by using double follicular units (DFU) in the center midscalp
Surgical Planning of the Donor Area
Related posts:





Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


