div class=”ChapterContextInformation”>
11. Scarring Alopecias
Keywords
Cicatricial alopeciaFrontal fibrosing alopeciaLichen planopilarisFolliculitis decalvansDiscoid lupusFibrosing alopecia in a pattern distributionDissecting cellulitisAcne keloidalis nuchaeCentral centrifugal cicatricial alopeciaScarring alopeciaIntroduction
Hair loss has been demonstrated to cause a negative impact on self-confidence and self-esteem and can lead to higher levels of anxiety and depression and social implications. Patients with scarring alopecias in particular suffer a substantial impairment of quality of life and high levels of distress [1].
Scarring or cicatricial alopecias are a heterogeneous group of disorders characterized by the irreversible destruction of hair follicles. Follicular damage in scarring alopecias may be either primary or secondary. In primary cicatricial alopecia (PCA), the hair follicle itself is the principal target for destruction. Secondary cicatricial alopecias result from events not directed to the follicular unit that end up having an effect on and eventually destroying the follicle. The permanent follicular scarring in these cases is the result of the close proximity of the follicles to the primary pathological process [2].
Clinically, the hallmark of cicatricial alopecias is the loss of follicular openings, while under pathology, they are characterized by the replacement of follicular structures with fibrous tissue [3].
NAHRS classification for primary alopecias
Lymphocytic |
Chronic cutaneous lupus erythematosus |
Lichen planopilaris (LPP) |
Classic LPP |
Frontal fibrosing alopecia |
Graham Little syndrome |
Fibrosing alopecia in a pattern distribution (FAPD)a |
Classic pseudopelade (Brocq) |
Central centrifugal cicatricial alopecia |
Alopecia mucinosa |
Keratosis follicularis spinulosa decalvans |
Neutrophilic |
Folliculitis decalvans |
Dissecting cellulitis/folliculitis |
Mixed |
Folliculitis (acne) keloidalis nuchae |
Folliculitis (acne) necrotica |
Erosive pustular dermatosis |
Nonspecific |
Recent data from a multicenter study involving 22 institutions specialized in hair disorders revealed that frontal fibrosing alopecia (FFA) is now the most frequent type of PCA in this setting, followed by lichen planopilaris (LPP), folliculitis decalvans (FD), discoid lupus (DLE), and fibrosing alopecia in a pattern distribution (FAPD) [5].
Treatment of PCA is many times challenging, and there are no fully satisfactory evidence-based regimens available for the treatment of such conditions. Here, we will focus on the treatment of the main causes of PCA according to published data and our experience on the field. In scarring conditions, the central aim of treatment will not be hair regrowth but rather to reduce symptoms and, most importantly, to stop disease progression. Early treatment is key to minimizing the extent of permanent alopecia.
Lichen Planopilaris
Lichen planopilaris (LPP) is a primary scarring alopecia in which a lymphocytic inflammatory infiltrate occurs at the isthmus level and destroys the follicular stem cells of the bulge. It mainly affects women, although it may appear also in men [6].
Its etiopathogenesis has not been clarified. PPAR-gamma deletion in hair follicle stem cells causes a similar inflammatory reaction that leads to epithelial-mesenchymal stem cell transition and fibrosis [7, 8].
LPP may appear at any part of the scalp, but it usually affects the vertex. The typical clinical presentation consists of small patchy hair loss in a diffuse distribution with perifollicular inflammation. The patches of alopecia may coalesce leaving large areas of scarring. It frequently associates pruritus and scalp dysesthesia that may be severe [6, 9].
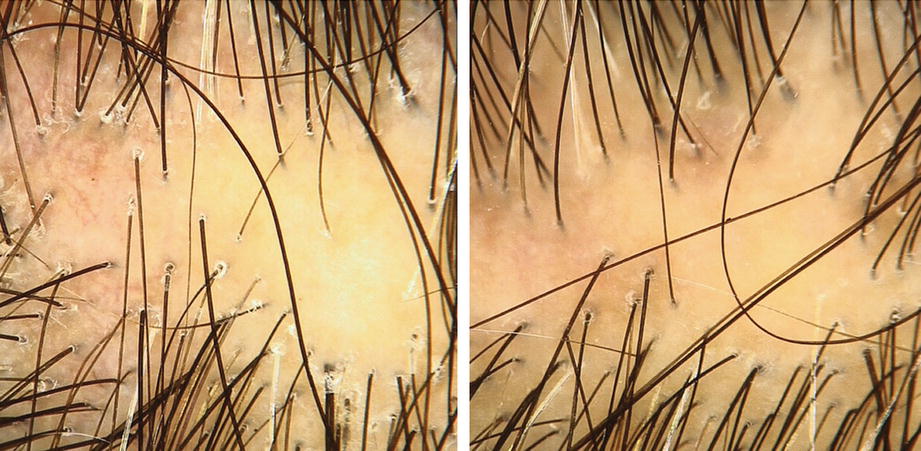
Trichoscopy of lichen planopilaris before and after systemic treatment
Histology shows a lichenoid infiltrate targeting the infundibulum and isthmus, with lamellar concentric fibrosis. Sebaceous glands are destroyed at early stages.
Management
Proposal of a therapeutic approach in lichen planopilaris
Treatment | Dosage | Duration | |
|---|---|---|---|
Mild inflammation (mild follicular erythema and hyperkeratosis) | |||
No symptoms | Topical corticosteroid | Four to seven times per week | Treatment can be stopped and check for relapses |
Mild pruritus | Topical corticosteroid | Four to seven times per week | Until improvement |
Consider intralesional steroids (triamcinolone acetonide) | 4–8 mg/mL every 8–12 weeks | Until improvement | |
Moderate inflammation (moderate hyperkeratosis or moderate pruritus) | |||
Maintain previous recommendations with topical and intralesional corticosteroids until improvement | |||
Add one or more of the following oral therapies | Hydroxychloroquine | 200 mg/12–24 h (5 mg/kg/day) | 12 months |
Doxycycline | 50–100 mg daily | 3 months | |
Oral retinoids | Isotretinoin 0.5–1 mg/kg daily | 6–12 months | |
Acitretin 25–50 mg daily | 6–12 months | ||
Severe inflammation (severe hyperkeratosis and erythema/severe pruritus/pain) | |||
Maintain previous recommendations with topical and intralesional corticosteroids until improvement | |||
Choose one of the following therapies | Oral cyclosporine | 3.5–5 mg/kg/day | 4–6 months until tapering |
Systemic steroids | Prednisone 1 mg/kg/day | 1–2 months until tapering | |
Dexamethasone 0.1 mg/kg twice a week | 3–4 months until tapering | ||
Oral mycophenolate mofetil | 1 g twice a day | 4–6 months until tapering | |
After control of the inflammatory flare, keep one of the previous options for moderate inflammation | |||
If bad control of the disease, consider adding oral naltrexone (3 mg daily), oral pioglitazone (15 mg daily), low-level laser therapy (655 nm, 15 minutes daily), or platelet-rich plasma injections | |||
The Lichen Planopilaris Activity Index (LPPAI) is a clinical scale to monitor response to therapy in LPP. It includes symptoms (pain, pruritus, burning), clinical inflammation (erythema, scaling), pull test, and progression of the disease [10].
Frontal Fibrosing Alopecia
Frontal fibrosing alopecia (FFA) is a primary scarring alopecia with an increasing incidence in the last decade, probably being the most frequent alopecia nowadays [5]. It occurs mainly in postmenopausal women, but it also appears in young women and men [14].
The cause behind this alopecia is unclear. Hormonal imbalance in genetically predisposed individuals could trigger an autoimmune reaction against the pilosebaceous unit. The inflammatory infiltrate could induce epithelial–mesenchymal stem cell transition and fibrosis as in lichen planopilaris.

Patient with frontal fibrosing alopecia in a linear pattern
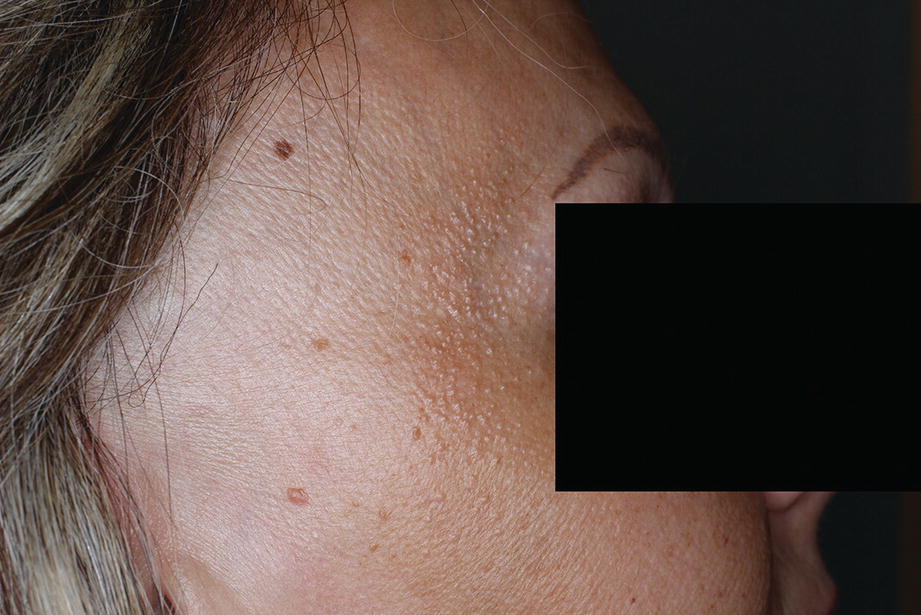
Facial papules in a frontal fibrosing alopecia patient
Management
Therapeutic management in frontal fibrosing alopecia
Treatment | Dosage | Duration | |
|---|---|---|---|
Local treatment | |||
Mild inflammation | Pimecrolimus 1% cream or tacrolimus 0.1% ointment Compound tacrolimus in cetaphil lotion to obtain 0.03% concentration | One to two times per week. Daily if needed Daily | Until improvement Can be utilized for long-term maintenance |
Moderate inflammation | Topical calcineurin inhibitor and clobetasol propionate 0.05% solution Consider triamcinolone acetonide injections | Four to seven times per week Four to seven times per week 4–8 mg/mL every 8–12 weeks | Until improvement (short-term follow-up) |
Severe inflammation | Clobetasol propionate 0.05% solution and triamcinolone acetonide injections | Four to seven times per week 4–8 mg/mL every 8–12 weeks | Until improvement (short-term follow-up) |
Partial eyebrows loss: topical calcineurin inhibitor + prostaglandin agonist eyedrops +/− triamcinolone acetonide injections 1–2 mg/mL | |||
Systemic treatment | |||
First-line therapies | Oral 5-alpha reductase inhibitors | Dutasteride 0.5 mg three to seven times a week Finasteride 2.5–5 mg daily | 2 years |
Second-line therapies | Hydroxychloroquine | 200 mg once or twice a day (5 mg/kg/day) | 1–2 years |
Oral retinoids | Isotretinoin 20 mg daily Acitretin 20 mg daily | 1–2 years 6–12 months | |
Third-line therapies | Pioglitazone | 15 mg daily | 6–12 months |
Cosmetic approach | |||
Facial papules: oral isotretinoin (5–30 mg daily for 2–12 months) | |||
Complete loss of eyebrows: microblading or cosmetic tattooing | |||
Hairline recession: partial hair prostheses or hair transplant (if 2 years without progression is confirmed) | |||
Eyebrow loss leads to an important cosmetic impairment, so its treatment is mandatory. Intralesional injections of triamcinolone 1–2 mg/mL can be used for partial hair loss, and regrowth is possible in early stages. Long-term topical treatment with latanoprost /bimatoprost or travatoprost eyedrops and calcineurin inhibitors is also recommended. Microblading and cosmetic tattooing are encouraged when complete loss of the eyebrows.
Facial papules can be treated with low-dose oral isotretinoin, but relapses are common after discontinuing usage [26]. To improve cosmetic impairment on hairline recession, partial hair prostheses or hair transplantation can be done, if stop of the alopecia is confirmed after 2 years.
Fibrosing Alopecia in a Pattern Distribution
Fibrosing alopecia in a pattern distribution (FAPD) is a primary scarring alopecia that involves androgenetic hair loss areas. The cases reported reflect a slight higher prevalence in women, but it also occurs in men [27–29]. The etiopathogenesis of this scarring alopecia is unknown, but the combination of hair follicle miniaturization and lichenoid inflammatory infiltrate leads to a permanent alopecia [27, 30].

Fibrosing alopecia in a pattern distribution in a 64-year-old female patient
Management
Proposal of therapeutic approach for fibrosing alopecia in a patterned distribution
Treatment | Dosage | Duration | |
|---|---|---|---|
Topical treatment | |||
Mild inflammation | Clobetasol propionate 0.05% solution | Four to seven times per week | Until improvement (short-term follow-up) |
Moderate inflammation and/or symptoms | Clobetasol propionate 0.05% solution Consider triamcinolone acetonide injections | Four to seven times per week 4–8 mg/mL every 8–12 weeks | Until improvement (short-term follow-up) |
Associate topical minoxidil 2%–5% once or twice daily (better low-propylene glycol preparations) | |||
Oral treatment | |||
Finasteride | Men: 1 mg daily Women: 2.5–5 mg daily | The same recommendations as those for androgenetic alopecia | |
Dutasteride | 0.5 mg daily | ||
Consider other antiandrogen options for women following recommendations for female androgenetic alopecia | |||
Consider oral anti-inflammatory treatment (doxycycline, hydroxychloroquine, etc.) following recommendations for lichen planopilaris | |||
Discoid Lupus Erythematosus
Alopecia is a well-known sign in chronic discoid lupus erythematosus (DLE). Approximately 60% of patients with DLE have patches of scarring alopecia on the scalp [31]. Association with systemic lupus erythematosus is not frequent, and only 5–15% of the patients will develop it [32].

Patch of alopecia due to discoid lupus erythematosus
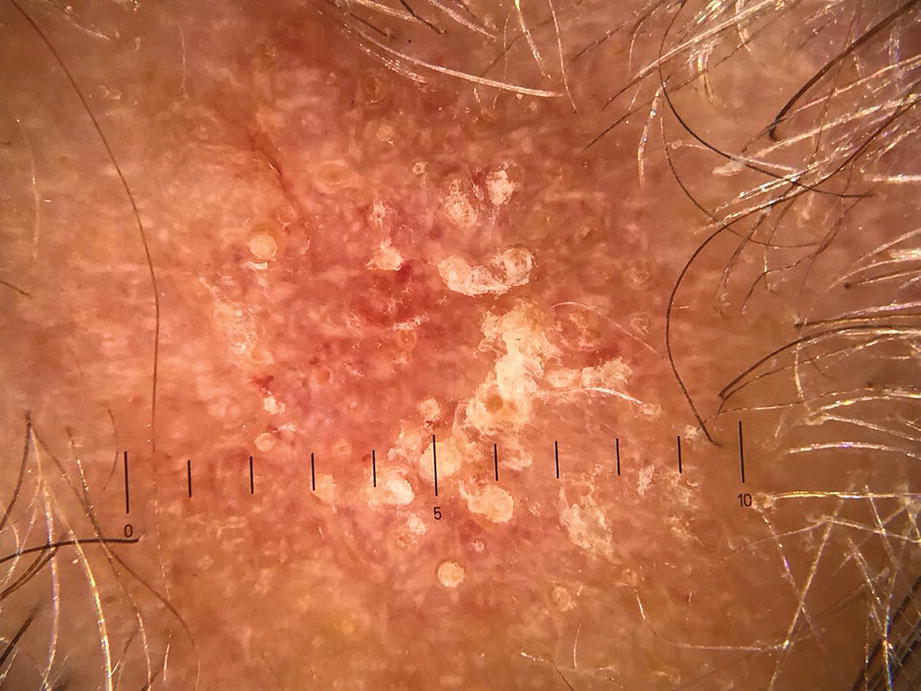
Trichoscopy of discoid lupus erythematosus lesion with follicular keratotic plugs
Management
Therapeutic approach for discoid lupus erythematosus
Treatment | Dosage | Duration | |
|---|---|---|---|
Local treatment | |||
Acute lesions | Topical Clobetasol propionate 0.05% | Four to seven times per week | Until improvement (short-term follow-up) |
And/or triamcinolone acetonide injections | 4–12 mg/mL every 8–12 weeks | ||
Chronic lesions and relapses prevention | Clobetasol propionate 0.05% solution | Once or twice a week | 3–4 months |
And/or topical calcineurin inhibitors | Every day | Adjust to relapses | |
Systemic treatment | |||
First-line therapies | Antimalarials | Hydroxychloroquine 200 mg daily or twice a day (5 mg/kg/day) Chloroquine 155 mg three times a day for 10 days and then 155 mg daily | 6–12 months Adjust to respond and consider long-term use according to relapses |
Second-line therapies | Add quinacrine | 100 mg daily | |
Third-line therapies | Methotrexate | 15–25 mg weekly | |
Other therapeutic options: retinoids, mycophenolate, dapsone | |||
Photoprotection (sunscreen, hats, sun avoidance) Smoking cessation | |||
Related posts:



Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


