div class=”ChapterContextInformation”>
14. Infections and Infestations
Keywords
Hair infectionsPediculosisTinea capitisPiedraTrichomycosisTrichoscopyTreatmentPediculicidesIvermectinAntifungalsAntibacterial agentsHair shavingIntroduction
Infections and infestations of the hair are caused by bacteria, fungi, and ectoparasites. These disorders have a worldwide distribution and affect both sexes and any age and race. Pediculosis is a pruritic infestation of the scalp (Pediculosis capitis) and pubis (Phthirus pubis). Pediculosis capitis affects mainly children and women with long hair, and pediculosis pubis affects pubic hairs and in some cases eyebrows and eyelashes. Tinea capitis is caused by dermatophytes and can be noninflammatory (trichophytic and microsporic) or inflammatory (Kerion celsi).

Trichophytic tinea caused by T. tonsurans

Inflammatory tinea capitis (Kerion celsi)
Diagnostic Procedures and Labs Required Before Starting Treatment

Pediculus capitis (dermoscopy 70×)
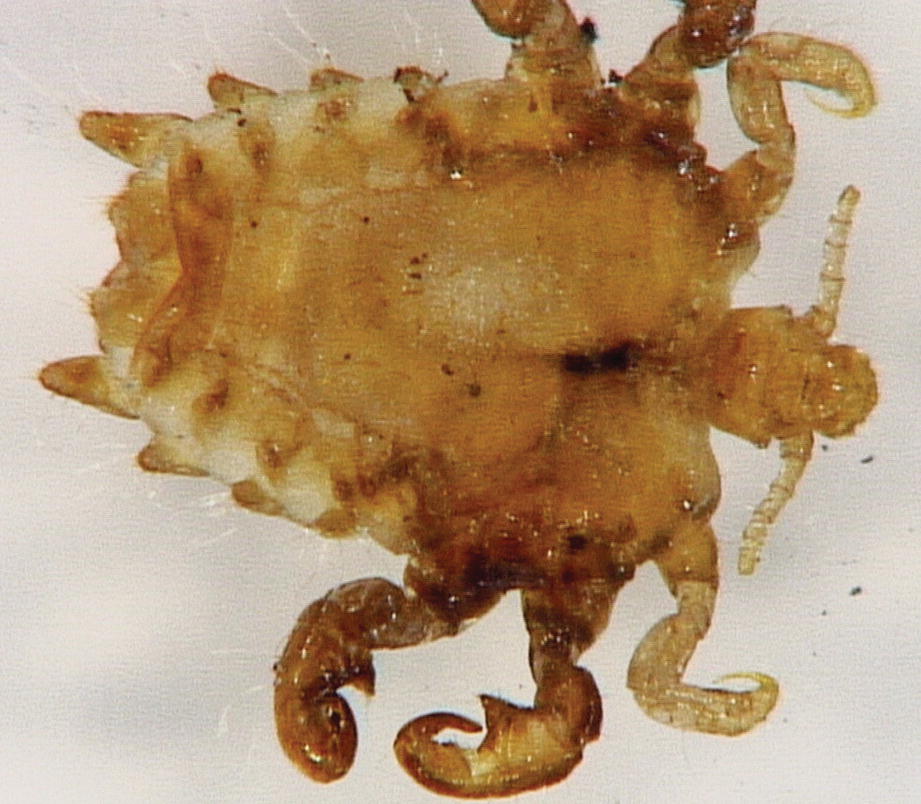
Pthirus pubis (dermoscopy 70×)

Pediculosis capitis (dermoscopy 70×)

Pediculosis nit (chlorazol black 40×)
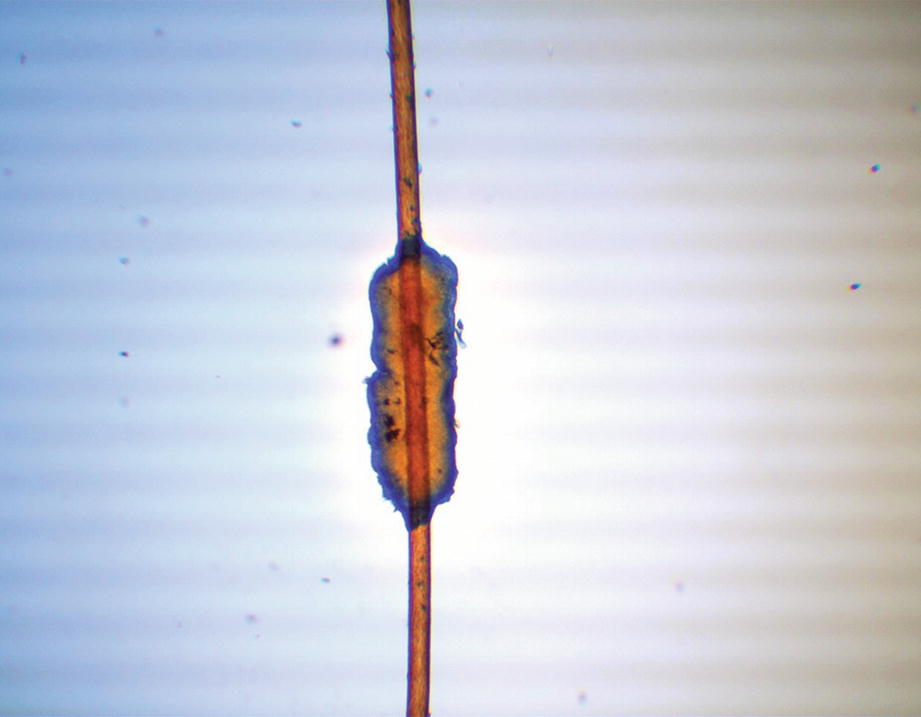
White piedra (Parker blue ink 20×)

Trichomycosis (lactophenol cotton blue 40×)
Treatment Strategy: A General Introduction
Treatment of hair infections and infestations can be topical or systemic. Therapeutic options depend on the drug availability, drug resistance, and education [7]. These diseases mainly occur in vulnerable groups: schoolchildren, homeless people, refugees, and in asylums [8]. Pediculosis in the USA occurs in 6–12 million children (age 3–12 years old) each year [9]. Topical pediculicides are the first line of treatment, but resistance is common. Manual removal of lice and occlusive agents are other alternative therapies. Oral treatment is required for refractory cases. The tinea capitis treatment depends on the clinical form, age, etiological agent, efficacy, safety profile, and pharmacokinetics. Griseofulvin, terbinafine, and itraconazole are the three main drugs used. In piedra and trichomycosis, treatments have a low therapeutic response. Hair shaving and hygiene measures can be excellent options [1–5].
Pediculosis
General Instructions to All Medications
Patients should be advised to look for lice and eggs in all family members and close contacts; all of them should be treated at the same time (including sexual contacts in pediculosis pubis). They should cover the complete scalp with the medication; be cautious with their eyes and wash the hands after application. Direct head-to-head contact must be avoided as well as sharing of combs, brushes, hats, hair bands, or other hair-related personal items should be sopped. One week after the treatment is finished, every member of the family should be examined [10–15].
First-Line Treatment
Topical Pediculicides
Topical pediculicides
Pediculicide | Mechanism of action | Age group | Application form | Side effects |
|---|---|---|---|---|
Pyrethrins/piperonyl butoxide | Neurotoxic | ≥2 years | Leave on dry hair for 10 minutes and then rinse; repeat 9 days later | Skin irritation, rare breathing difficulties in patients with ragweed and chrysanthemum allergy |
Permethrin 1% | Neurotoxic | ≥2 months | Leave on damp hair for 10 minutes and then rinse; repeat 9 days later | Skin irritation, rare breathing difficulties in patients with ragweed and chrysanthemum allergy |
Malathion 0.5% | Neurotoxic | ≥6 years contraindicated in children aged under 2 years | Leave on dry hair for 8–12 hours and then rinse. A single application is effective; repeat 7–9 days later if live lice are identified | Malodorous, flammable, skin irritation, theoretical risk of respiratory depression if ingested |
Benzyl alcohol 5% | Asphyxiation | ≥6 months | Leave on dry hair for 10 minutes and then rinse; repeat 7 days later | Skin and eyes irritation, transient skin numbness on application site |
Spinosad 0.9% | Neurotoxic | ≥6 months | Leave on dry hair for 10 minutes and then rinse; repeat 7 days later | Skin irritation |
Ivermectin | Neurotoxic | ≥6 months | Leave on dry hair for 10 minutes and then rinse. A single application may be effective; repeat 7–9 days later if live lice are identified | Skin and eyes irritation |
Dimethicone 4% | Asphyxiation | ≥6 months | Leave on dry hair for 8–12 hours and then rinse. A single application may be effective; repeat 7–9 days later if live lice are identified | Flammable |
Pyrethroids
They are made from a natural chrysanthemum extract and neurotoxic to lice. These formulations are often combined with piperonyl butoxide that inhibits the pyrethrin catabolism in the louse and improves drug efficacy. They must be applied over dry hair for 10 minutes before rinsing; treatment must be repeated 9 days later. Permethrin 1% is a synthetic pyrethroid that is applied in the same way but on damp hair. These pediculicides are available over the counter. Prescription-strength permethrin (5%) is indicated only for scabies and not approved as a pediculicide in some countries. Clinical evidence showed that the effectiveness of this preparation is not higher than the over-the-counter ones . Pyrethroids have extremely low mammalian toxicity. In rare cases, they may cause breathing difficulties in patients with ragweed and chrysanthemums allergies. Skin irritation is another potential side effect. Pyrethrins can be used in ≥2-year-old patients and permethrin in ≥2-month-old patients [14, 16, 17].
Malathion
It is an organophosphate cholinesterase inhibitor with neurotoxic effects on lice. It is important to know that this agent has pediculicidal and ovicidal properties . A 0.5% lotion can be applied on dry hair for 8–12 hours before washing off with a nonmedicated shampoo. Some reports showed the effectiveness of malathion in applications of less than 20 minutes. Heat sources such as hair dryers, curling irons, or flat irons should not be used on dry hair because of the flammability properties of the product. A single application of malathion is often enough; however, if live lice are identified after 7–9 days, a second treatment must be applied. This drug is malodorous and irritating to the eyes. Stinging sensations and chemical burns are other reported side effects. There is a theoretical risk for respiratory depression after accidental ingestion. It is recommended in patients older than 6 years old and contraindicated in children under 2 years old [18, 19].
Benzyl Alcohol 5%
The mechanism of action involves asphyxiation of lice and paralyzation of louse respiratory spiracles. The lotion is applied over dry hair and rinsed off with water after 10 minutes. Treatment should be repeated after 7 days. Benzyl alcohol may cause skin and eyes irritation, as well as transient numbness at the area of application. It can be used in patients older than 6 months [17, 19, 20].
Spinosad
It is obtained through fermentation using the soil bacterium Saccharopolyspora spinosa ; it affects the central nervous system of lice by interfering with the nicotinic acetylcholine receptor, which causes neuronal excitation and paralysis. Topical 0.9% suspension is applied to the dry scalp for 10 minutes and rinsed subsequently with water. Treatment should be repeated if live lice remain after 7 days from the initial application. Skin irritation is a potential side effect, and its use is not recommended for children under 6 months [20–22].
Topical Ivermectin
This neurotoxic drug binds to the lice glutamate-gated chloride channels, causing paralysis and death. The application is recommended on the dry scalp for 10 minutes with posterior rinse; treatment must be repeated after 7 days in case live lice persist. Adverse effects include ocular irritation, dry scalp, and a burning sensation on the skin [23–25].
Dimethicone 4% Lotion
It is a long-chain linear silicone in a volatile base that asphyxiates the lice. It must be applied for 8 hours at night and washed out the next morning. Treatment must be repeated 1 week later. New dimethicone formulations can be applied for 10 minutes only. These products are flammable; therefore, contact with potential sources of fire (cigarettes or hair dryers) must be avoided during treatment. Resistance to dimethicone is questionable due to its physical mechanism of action [26–29].
- 1.
Hair conditioners must be avoided before application, as they may reduce the efficacy [30].
- 2.
Skin exposure to pediculicides should be limited; thus, the application is recommended over a sink rather than in a shower or bath [31].
- 3.
Apply treatment with warm water instead of hot water to avoid vasodilation and systemic absorption [31].
Pediculicide Resistance
The real prevalence of resistance to a specific pediculicide is unknown, and it may vary from one geographical region to another. It is important to consider this factor for therapeutic elections [32–34]. Pyrethroids and malathion are the pediculicides with the most reported resistances. The primary mechanism for pyrethroid resistance that has been proposed is a mutation in the louse kdr allele which causes a decreased sensitivity of neuronal voltage-gated sodium channels [16, 35]. In the case of malathion, there is an increased production of metabolic enzymes and a decrease in the sensitivity of the drug to neuronal acetylcholinesterase [30].
Second-Line Treatments
Occlusive Agents
These agents aim to suffocate the lice. They are widely used, but their effectiveness has not been evaluated yet in controlled trials. Viscous substances, such as petroleum jelly, mayonnaise, tub margarine, herbal oils, olive oil, vinegar, and tea tree oil, obstruct the respiratory spiracles of the adult louse and the operculum holes of the eggs, blocking the air exchange. All these suffocating-based pediculicide agents must be applied on dry hair, left on overnight, and washed out the next morning. The process must be repeated once per week for 3 weeks [36–39].
Manual Removal
Manual removal of nits is recommended after treatment with any topical pediculicide. It is suggested that lice removed through combing and brushing are damaged and rarely survive. Hair combing is recommended every 1–3 days as an adjuvant and preventive measure. A combination of combing with oils or vinegar facilitates the removal of nits. Fine-toothed “nit combs” are handy for this purpose, and metal combs have proved to be more effective than plastic ones. Complete shaving of the head eliminates lice and prevents reinfestations; however, the use of this method is controversial as it can cause social stigmata [40, 41].
Oral Ivermectin
This drug affects the neurotransmission in arthropods and helminths, leading to paralysis and death. A single dose of ivermectin (200 μg/kg) is effective and should be repeated 1 week later. Ivermectin is not recommended for pregnant women or children weighing less than 15 kg [42–45].
Third- and Fourth-Line Treatments
Trimethoprim-Sulfamethoxazole
Its mechanism of action may involve the death of symbiotic bacteria in the louse gut which produces B vitamins necessary for louse survival. Although rare, severe adverse reactions to this drug include Stevens-Johnson syndrome, neutropenia, hemolysis, and renal impairment, which is why this treatment is reserved only for resistant cases [46, 47].
Heat
Heating clothing and bedding with hot water destroy all stages of the lice (52 °C for 30 minutes). Sometimes, due to a hormonal process, lice can make themselves heat-resistant (natural defense mechanism) and tolerate very high temperatures, even above 100 °C [48–50].
Others
Agents like lindane (human neurotoxicity risk), carbamate, isopropyl myristate 50%, crotamiton 10%, benzyl benzoate 25%, 1,2-octanediol, cocamide diethanolamine lotion, and tocopheryl acetate 20% had shown some effectiveness in pediculosis treatment [51–54].
Over-the-counter antilice shampoos are used as adjuvant therapy improving the hair cosmetics but useless as pediculicides.
Tinea Capitis
Treatment Overview
Tinea capitis treatment should be started once the clinical diagnosis and the KOH fungal confirmation are completed. Waiting for culture result is not recommended because delaying treatment may increase the risk for disease progression, permanent hair loss, and transmission [3, 55].
Oral therapy based on the use of griseofulvin, terbinafine, itraconazole, or fluconazole generally results in a clinical and mycological cure. On the other hand, there is no clinical evidence for other oral antifungals such as voriconazole or posaconazole. Tinea capitis requires clinical follow-up to determine if oral antifungal treatment should be discontinued or changed or if additional treatment is needed. Topical therapy alone is not recommended [3, 56].
Griseofulvin and terbinafine are the two drugs approved by the US Food and Drug Administration (FDA). According to BAD guidelines in the UK, the aims of treatment are a clinical and mycological cure, scarring prevention, and the end of the transmission [3, 55–57].
First-Line Treatment
Drugs of choice for each etiological agent
Drug | Etiological agent |
|---|---|
Terbinafine | Trichophyton tonsurans, T. violaceum, T. soudanense |
Griseofulvin | Microsporum canis, M. audouinii |
Itraconazole | Microsporum canis, M. audouinii |
Griseofulvin
It is a fungistatic drug that inhibits nucleic acid synthesis and impairs the synthesis of the cell wall. Presentations include micronized, ultramicronized, and suspension forms. This drug is not always available in Europe and Latin America [58]. The recommended dose in children is 15–20 mg/kg/day in single or divided doses for 6–8 weeks. Absorption and bioavailability can be increased with the intake of fatty food (e.g., peanut butter, ice cream). In resistant cases, doses up to 25 mg/kg may be necessary. The dose must be adjusted for each species. Griseofulvin effectiveness is low against Trichophyton spp. [59]. Ultra-micronized griseofulvin has better gastrointestinal absorption and can be used in lower doses (10–15 mg/kg/day).
A meta-analysis comparing particular doses of griseofulvin and terbinafine has shown that griseofulvin is the first-line treatment for children in whom the etiological agent is unclear [60].
Side effects such as gastrointestinal disturbance, rash, and headache can be observed in 20% of patients. Serious side effects like hepatotoxicity, granulocytopenia, leukopenia, and severe cutaneous reactions are uncommon. Griseofulvin is contraindicated in lupus erythematosus, porphyria, liver disease, and pregnancy. Drug interactions include warfarin, ciclosporin, and contraceptive pills [59, 61].
Terbinafine
It is an allylamine with fungicidal activity on the cell membrane of every dermatophyte, especially Trichophyton spp. [57, 62, 63]. Terbinafine is an alternative first-line treatment and considered the optimal choice due to shorter courses, cost-efficiency, and compliance [59]. A meta-analysis showed that the effectiveness of 2–4 weeks of treatment with terbinafine is similar to that of the 6–8 weeks treatment with griseofulvin for T. tonsurans. In microsporic tineas, higher doses are required [64–68].
Terbinafine pediatric doses
Related posts:




Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


