div class=”ChapterContextInformation”>
20. How to Evaluate Treatment Response in Hair Diseases
Keywords
Follow-upDynamic trichoscopyTherapeutic failureHair disordersIntroduction
When treating patients with scalp diseases, it is essential to be able to evaluate treatment response. Treatment response will allow further decision-making such as increasing or decreasing treatment dose, changing the treatment vehicle, changing therapy, or adding adjuvant treatments.
If treatment is not working, the first factor to consider is treatment compliance. Listen to patient concerns regarding symptoms, secondary effects, and emotional burden.
In cicatricial alopecia, it is critical to explain to the patient that the objective is to stop disease progression and keep the remaining hair healthy. It is very common for patients with scarring alopecia to have unrealistic expectations and complain that they did not see any improvement when they come to the follow-up visit.
Sometimes, hair disorders have multifactorial causes, so response to treatment may be affected not only by the prescribed therapy but also by changes in daily habits such as physical exertion, diet, new drugs or supplements, patient’s hair routine, salon’s treatments, deep-conditioning treatments, sleeping patterns, or changes in physical health such as disease, surgeries, or pregnancy.
Always listen to the patient but also verify treatment efficacy using objective methods, as these are the only parameters that really show if the treatment is working.
Instruments to Evaluate Treatment Response
Handheld Dermoscopy
With standard magnification at ×10 and ×20 (handyscope), they are divided into three groups: contact, polarized light contact, and polarized light noncontact. Hybrid dermoscopes work either in contact or in noncontact mode [1].
Videodermoscopy
It is highly beneficial for documentation, as it takes high-magnification and high-quality pictures that can be compared side by side. Magnification from ×14 to ×100 (FotoFinder systems) allows the visualization and characterization of hair and other scalp structures that could not be seen with other devices. Also, these devices have a specialized software that allows to manually measure hair density, number of follicular units, and thickness and proportion of vellus vs. terminal hair, helping to monitor therapeutic response (Folliscope) [1]. Automatic measures require hair shaving, which is gold standard for clinical studies but is not practical in daily life. FotoFinder also offers a very specialized service, called TrichoLAB, where the user can send the pictures taken without shaving and obtain all the measures. This service also offers an expert for the evaluation of trichoscopic pictures and gives accurate diagnosis.
Cross-Section Trichometry
The cross-section trichometer is a handheld device for measuring hair mass. It “grabs” a bundle of hair from a 2 × 2 cm scalp area in a J-slot, measuring the cross-sectional area of the hair bundle. It then displays the Trichometric Index (TMI), which is determined by the number of hair fibers (density) and hair diameter. The numeric value of TMI allows the monitoring of hair mass over time in a given area selected using a template [2].

Phototrichogram
This device measures hair density (hairs/cm2), thickness (μm), length (mm), and linear growth rate (mm/day), which is calculated based on a specified scalp area of 1 cm2 over a period of 3 days. Evaluation of the same area of the scalp at regular intervals allows objective evaluation of treatment response. However, it requires tattooing, hair clipping, and two office visits for each evaluation; not all the patients are willing to undergo this test [1].
Hair-Shedding Visual Scale (HSVS)
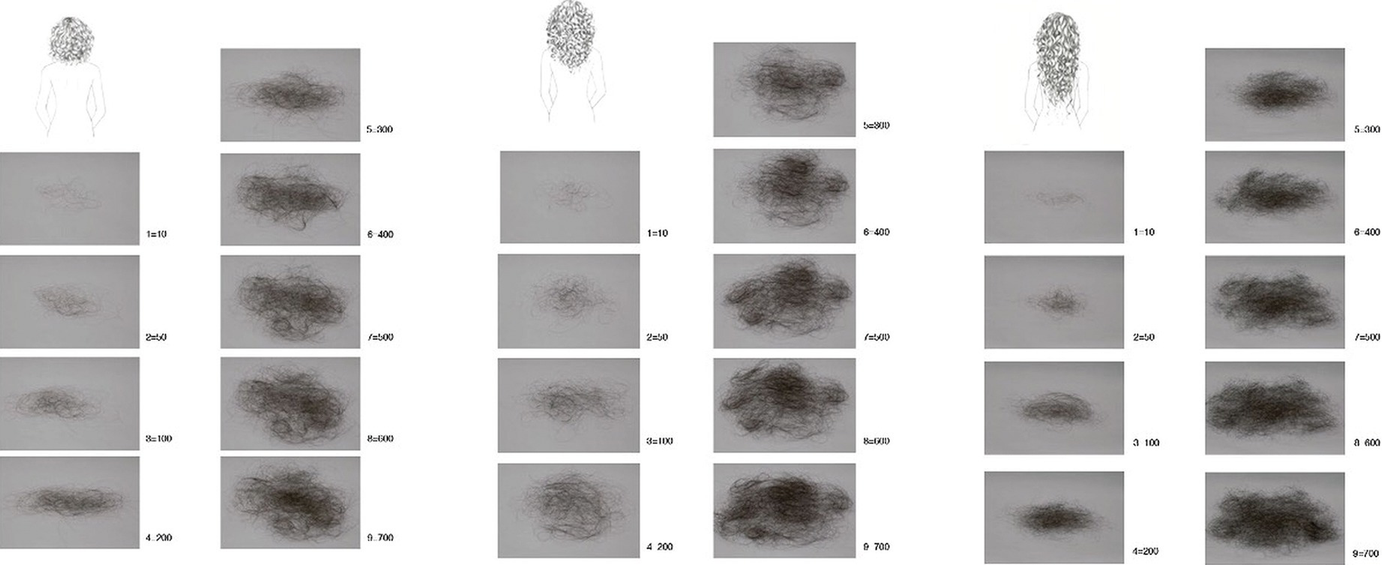
Hair shedding visual scale
Frontal Fibrosing Alopecia Severity Index
Frontal fibrosing alopecia severity index
Thickness and lymphocytic infiltrate correlationa | Trichoscopy vs. histological validation | ||||
|---|---|---|---|---|---|
Grade | Quantitative values | Qualitative values | Lymphocytes/field /40× | Results (median)b,c | Validations (sensitivity/concordance) |
Grade 1 | <0.2 mm | Mild/thin | <5 | 0.12–0.16 mm (0.15 mm) | 54/56 (91%/0.83) |
Grade 2 | 0.2–0.44 mm | Moderate/thin to thick | 5–10 | 0.2–0.44 mm (0.40 mm) | 64/70 (91%/0.80) |
Grade 3 | >0.44 mm | Severe/thick | >10 | 0.50–0.70 mm (0.60 mm) | 14/14 (100%/1.0) |
Frontal Fibrosing Alopecia Severity Index
This index considers hairline recession (grades 1–5), frontal band inflammation, nonscalp hair loss (eyebrow, eyelash, limb, and flexural), and associated features (facial papules, cutaneous , nail, and mucosal lichen planus, and generalized scalp lichen planopilaris). This index has a maximum score of 100 [6].
Frontal Fibrosing Alopecia Severity Score
This score considers grade of frontal and temporal hairline recession (from 1 to 5), grade of eyebrow loss (none, partial, or total), severity and extent of perifollicular erythema and hyperkeratosis, and severity and frequency of pruritus and pain associated with FFA. The resulting severity scores ranged from 0 to 25, with higher scores indicating greater severity. The clinical features included in the FFASS are grouped into two categories: extent of alopecia (up to 21 points) and inflammation (up to 4 points) [7].
Lichen Planopilaris Activity Index

Dr. Tosti’s Scale for Inflammation
This scale is performed to evaluate the degree of inflammation in seborrheic dermatitis and psoriasis. It evaluates percentage of scalp showing arborizing or glomerular vessels and scales under 20× magnification: grade 5, 100%; 4, 75%; 3, 50%; 2, 25%; 1, 25% to 10%; and 0, less than 10%.
Severity of Alopecia Tool (SALT) Score
The SALT score I is a global severity score that calculates the percentage of hair loss. It divides the head into four projections (top, back, and each side of the scalp). Using this diagram, one can determine the percent scalp hair loss in a given quadrant and multiply this by the total scalp area delineated by that quadrant and sum the resultant numbers for each quadrant to get the total percent scalp hair loss . This diagram also allows the evaluator to graph the area(s) of alopecia, if desired, in order to facilitate the estimate of percent scalp hair loss and to compare the hair loss on subsequent evaluations [9].
Global Photography
For clinical studies, it is important to utilize a stereotactic positioning device where the patient’s chin and forehead are fixed, and on which a camera and flash are mounted, assuring a reproducible view, magnification, and lighting at consecutive visits. Patients should keep the same hairstyle and color. Four standard views (vertex, midline, frontal, and temporal) are recommended, allowing paired comparisons of global photographs after treatment [1].
However, this is not always possible in daily practice. So, you can utilize a normal camera for photographic documentation, but it is important to take the pictures in the same conditions (light, color, and distance) in order to compare in consecutive visits. It is impossible to do a proper follow-up of hair diseases without photographic documentation!
Dynamic Trichoscopy
Dynamic or sequential trichoscopy facilitates the observation of scalp diseases over time, allowing to monitor treatment in cicatricial and noncicatricial alopecias. It helps to identify specific clues about the disease stage and progression, increasing the pathogenetic understanding of scalp diseases. It allows identifying the areas that need therapeutic interventions and showing the patients if treatment is effective [10].
Evaluating Treatment Response in Specific Scalp Diseases
Noncicatricial Alopecias
Androgenetic Alopecia
Treatment Goals
Stop hair shedding . Increase average hair thickness and number of follicular units with more than one hair. Decrease hair shaft variability and proportion of thin hairs and yellow dots per field of view.
Patients need to understand that treatment will work as long as they have good compliance.
Evaluation Instruments
Global photography
Videodermoscopy
Folliscope
Dynamic trichoscopy
Cross-section trichometry
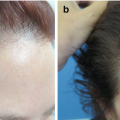
Trichoscopic Signs of Progressing Versus Improving (Fig. 20.2)
Progressing: variability (more than 20% miniaturization), yellow dots, thin, short, regrowing hairs.
Improving: decrease in the hair shaft variability, short regrowing hairs of normal thickness
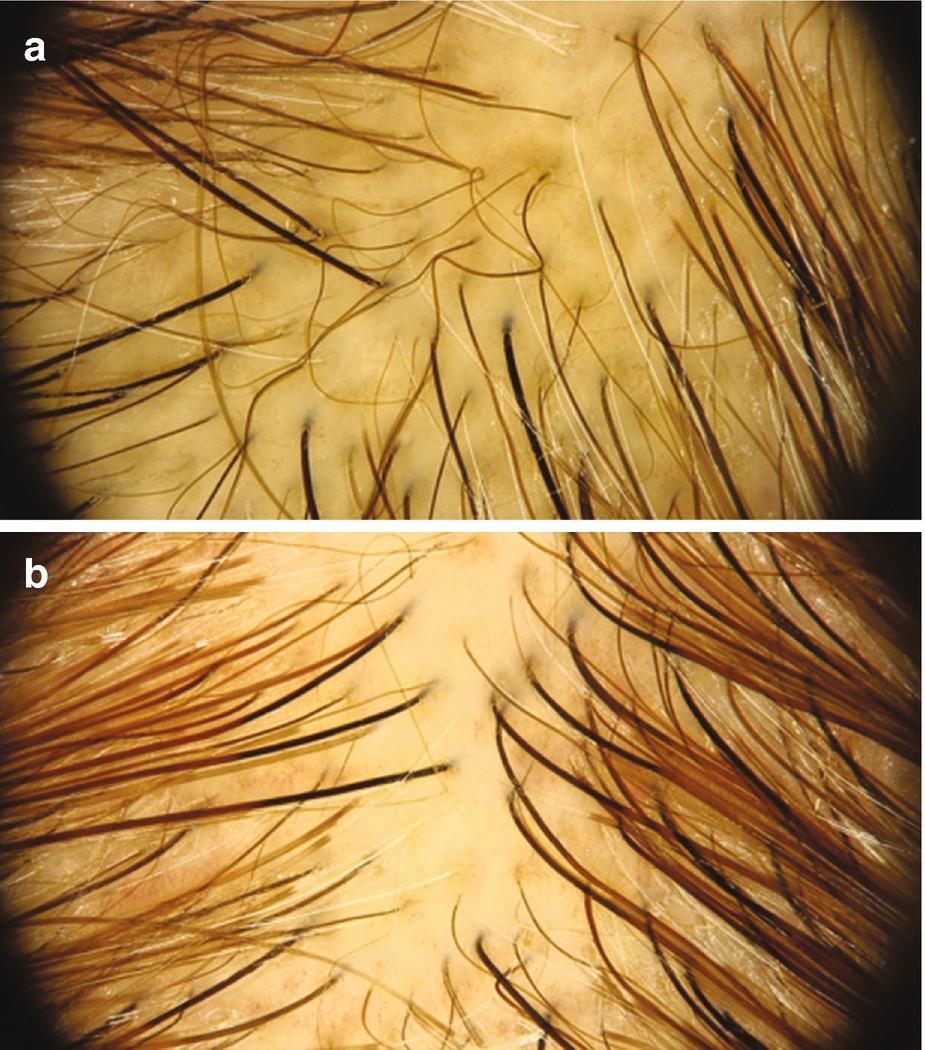
(a) Hair shaft variability (more than 20% miniaturization), yellow dots. (b) The patient after 6 months of treatment with minoxidil 5% and finasteride 2.5 mg; notice the increase in hair diameter and the decrease in hair shaft variability and follicular units of one hair
Hair-Shedding Visual Scale
The scale is very useful for monitoring treatment response in women, favoring the decrease of patient anxiety as they can see they shed less.
What to Expect
Increase in hair density and thickness.
What to Do if Patient Is Not Responding to Treatment
Contact dermatitis is a common secondary effect of minoxidil. Consider patch testing for contact dermatitis , which can be due to propylene glycol or minoxidil. Foam formulation is a good alternative when there is an allergy to propylene glycol. For this purpose, you need to patch test the patient’s personal lotion, propylene glycol 30% in water, and the commercial Rogaine foam. Patients who react to the foam are allergic to minoxidil itself.
In these cases, consider other options such as oral minoxidil, topical latanoprost, or nanoxidilR. Nanoxidil is the patented name for pyrrolidine diaminopyrimidine oxide [PDPO], a potassium channel opener with a molecular structure that is similar to minoxidil but with higher activity on potassium channels and lower molecular weight.
If the patient is not responding to 1 mg of finasteride, consider changing to dutasteride 0.5 mg and combine with adjuvant therapy [11, 12].
Identifying scalp comorbidities is a priority during AGA treatment. Telogen effluvium does not cause androgenetic alopecia; however, it definitely worsens it.
Inquire about new drugs (including contraceptives, such as levonorgestrel) and “supplements,” including vitamin A, wheat proteins, DHEA testosterone, diets of less than 1200 kcal, and new exercise routine (keep in mind that anaerobic exercise increases testosterone levels and aerobic exercise can increase oxidative stress). Also, inflammatory processes of the scalp such as seborrheic dermatitis or psoriasis may affect the response, making it important to control inflammation during AGA treatment. If trichoscopy shows multiple yellow dots or circular (pigtail) hairs, consider alopecia areata incognito as a differential diagnosis, and consider a scalp biopsy.
Telogen Effluvium
Treatment Goals
Identify and correct the triggering factor and stop hair shedding.
In telogen effluvium without scalp comorbidities, reassurance is important. Explain to the patient that even if hair shedding continues, this will not lead to alopecia. Showing the dermoscopic images with the new hair regrowing is always helpful. However, do not forget that TE can aggravate AGA, so a special effort to control telogen effluvium must be made in patients with dermatoscopic signs of miniaturization [13].
Evaluation Instruments
Videodermoscopy
Folliscope
Global photography
Dynamic trichoscopy
Cross-section trichometry
Trichoscopic Signs of Activity (Fig. 20.3)
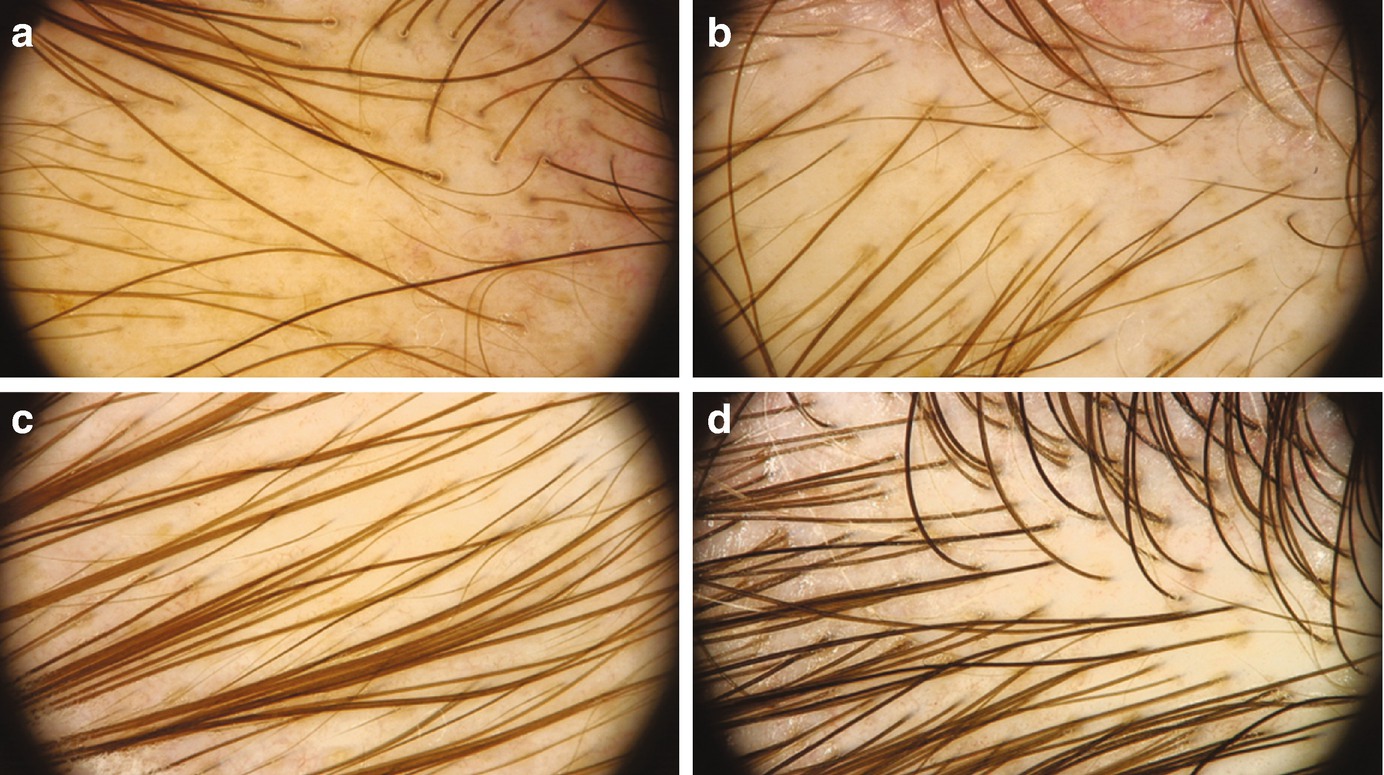
(a) Postpartum telogen effluvium at 3 months after delivery, notice the multiple short regrowing hairs, yellow dots, and single follicular units. (b) Follow-up at 5 months. (c) Follow-up at 7 months. (d) Follow-up at 12 months
What to Expect
Hair shedding stops during the first 3 months, and clinically, visible recovery can be observed at the sixth month. It will be observed as an increase in hair density and no empty follicles.
Activity Scale
Hair Shedding Visual Scales
What to Do if the Patient Is Not Responding to Treatment
Re-interrogate for new drugs, diets, extenuating physical routine, emotional stress, anti-cellulite creams, herbal treatments , over-the-counter supplements, recent surgeries, shampoos with keratolytic, vitamin A consumption, excessive sun exposure, changes in hair dye products, new hair care treatments, and interruption of oral contraceptives.
Consider inflammatory scalp conditions such as contact dermatitis, psoriasis, or seborrheic dermatitis that can also cause or aggravate telogen effluvium. Topical or systemic corticosteroids can help to control the excessive shedding while the triggering factor is corrected.
In cases where the triggering factor is identified and treated, repeat laboratory testing to assess if medication is solving the problem.
It is also important to consider the possibility of chronic telogen effluvium, defined as diffuse telogen hair loss that persists over 6 months. Its cause is usually multifactorial and difficult to establish, and it is currently proposed that it may be caused by an intermittent pathologic synchronization of the hair cycle, anagen phase shortening, or early teloptosis. It remains a diagnosis of exclusion, whereby it must be kept in mind that multiple-cause relationships may underlie this type of hair loss, including significant seasonal fluctuations of hair growth and shedding, and potential overlap with androgenetic alopecia . Most of these patients feel distressed when seasonal effluvium comes, so it is vital to help them prepare for this time of the year (some of them refer to trichodynia before shedding) [14, 15].
Alopecia Areata
Treatment Goals
Achieve total or partial hair regrowth through immunosuppression or immunomodulation.
Developing emotional coping skills is crucial, as they will benefit the patient’s compliance and general well-being, allowing a better response to treatment.
Evaluation Instruments
Dermatoscopy
Dynamic trichoscopy
Global photography
SALT score
Trichoscopic Signs of Activity (Active or Inactive Disease) (Fig. 20.4)
Signs of activity of disease: yellow/black dots, exclamation mark hairs, broken hairs, circular hairs and monilethrix-like hairs.
In inactive disease, trichoscopy shows regularly distributed yellow dots and features of hair regrowth, such as the presence of upright regrowing hairs.
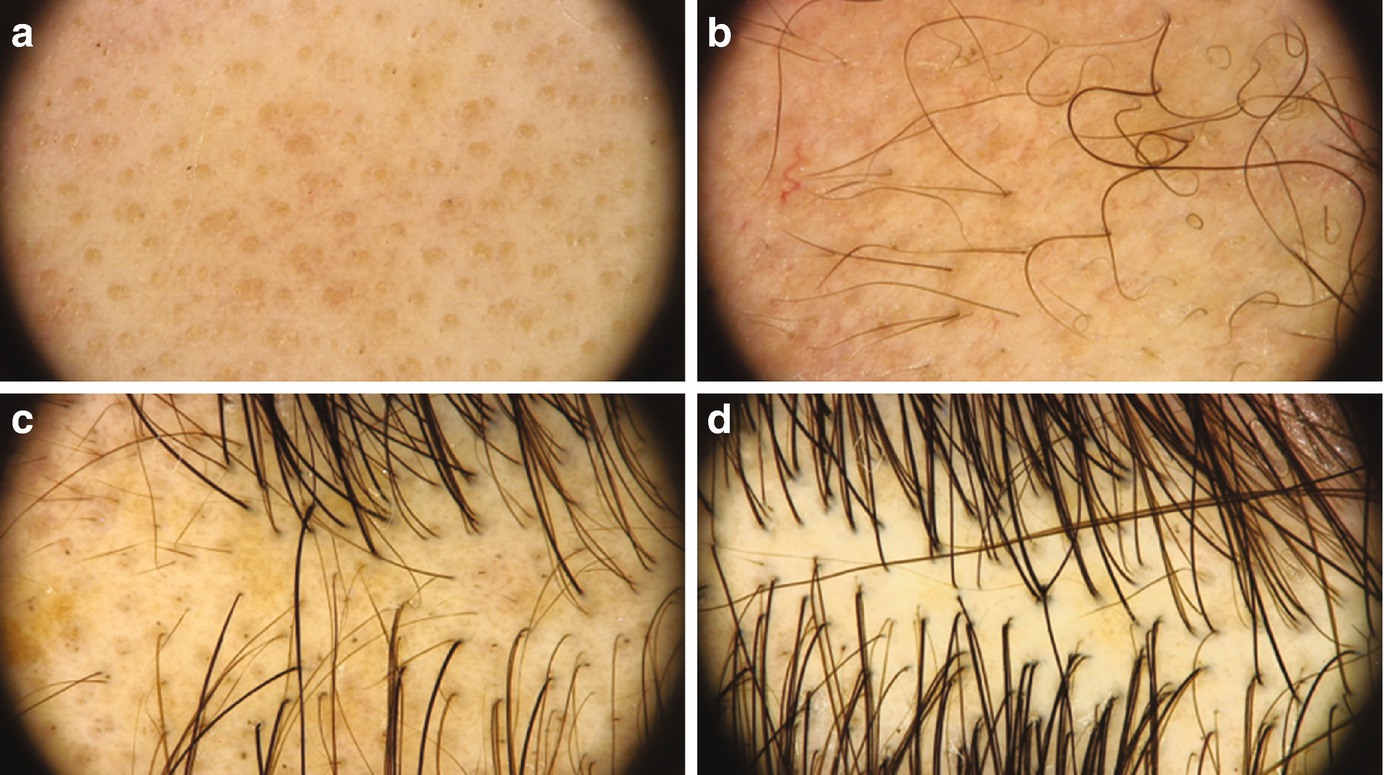
(a) Yellow dots in a patient with alopecia areata totalis of 6 years of evolution before immunotherapy. (b) Follow-up at 3 months with yellow dots, circular hairs, and short regrowing hairs. (c) Follow-up at 6 months with some black dots and multiple short regrowing hairs. (d) Follow-up at 9 months, without signs of activity
What to Expect
Response to treatment and possibility of relapse is unpredictable.
We recommend to check the patient every 3 months when the disease is active.
Therapy is considered unsuccessful after 9–12 months of treatment with no response.
Positive results may be observed from the first month of therapy; however, in most cases, it may take minimum 3–6 months.
If complete regrowth is achieved , follow-up visits to detect relapse must be scheduled every 3 months. Patient should be advised to come back as soon as they detect a sign of relapse.
If relapses do occur, re-start or change treatment as soon as possible.
What to Do if the Patient Is Not Responding to Treatment
Multiple options for treatment are available. Following an algorithm of treatment that takes into consideration the age of the patient, comorbidities, and extent of alopecia will help to establish treatment strategy. Escalating immunosuppressive potency with monotherapy, starting combined immunosuppressive therapy, or adding adjuvant therapy may help obtain better results . Also, evaluate changing the treatment strategy from immunosuppression to immunomodulation or vice versa to achieve hair growth. Discuss camouflage options with the patient to improve quality of life [16–18].
Cicatricial Alopecias
Frontal Fibrosing Alopecia
Treatment Goals
Control inflammation and stop the progression of hair loss and fibrosis.
Reduction of symptoms associated with the disease such as burning and itching sensation.
Help the patient to understand the importance of proper treatment compliance, to avoid cicatricial progression of the disease.
Help the patient to have a normal life. The cosmetic consequences in these patients are significant, so once the disease is controlled, it is important to find options that allow the patient to feel comfortable and secure.
Related posts:



Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


