Pitching, catching, and base-running may predispose professional baseball players to injury—particularly in the hand and wrist. In this study, we outline the diagnosis, management, and rehabilitation of commonly encountered injuries among these high-level athletes. Wrist injuries discussed include hook of hamate fractures, extensor carpi ulnaris tendon disorders, scapholunate instability, and triangular fibrocartilage complex tears. Hand injuries discussed include thumb ulnar collateral ligament injury, flexor tendon pulley rupture, hypothenar hammer syndrome, and blisters.
Key points
- •
Injuries to the hand and wrist can be debilitating for professional baseball players.
- •
Though hand injuries are more common than wrist injuries in professional baseball players, wrist injuries more commonly require surgical intervention.
- •
A thorough understanding of the underlying anatomic considerations of a player’s injury may facilitate more rapid recovery and return to play.
Introduction
Baseball players are subject to an increased risk of acute and chronic injury to their upper extremities. The movements required to pitch, catch, and run the bases involve movements at high speeds. It is, therefore, not surprising that baseball players of all skill levels deal with injury to their extremities. A significant portion of these injuries involve the upper extremity—the most affected area being the hand and wrist. ,
Given the increased risk of injury to the upper extremity, the Major League Baseball (MLB) and Minor League Baseball (MiLB) organizations developed a tracking system to better characterize injuries sustained by high-level baseball players. Known as the Health and Injury Tracking System (HITS), MLB and MiLB players who sustained an injury requiring at least 1 day away from play were entered into the system by each club’s athletic training staff. Thus, the HITS database became an important resource for clinicians. In an epidemiologic study of the database by Rhee and colleagues, the authors found that 4478 hand and 1748 wrist injuries were sustained by both MLB and MiLB players over 5 seasons. The most common injury mechanism was batting, and the most common injuries requiring surgery were hamate and scaphoid fractures.
As clinicians learn more about the common hand and wrist conditions highlighted in the HITS database, they can also use this information in treatment algorithms. Many of the injuries encountered in baseball players are conditions seen and treated in most hand specialist practices. However, the challenges of treating high-level baseball athletes include prompt diagnosis, sport-specific treatment, and injury prevention. In addition, considerations such as contract negotiations and playoff implications may further guide the discussion of operative versus nonoperative treatment.
In this study, we identify common injuries encountered in baseball players. We discuss the diagnosis, treatment, and rehabilitation of these injuries and the subtle nuances required to adequately care for the high-level baseball player. We first discuss common conditions in the wrist followed by those encountered in the hand. We hope the clinician will be able to recognize these special considerations in optimizing treatment and facilitating a safe and expeditious return to sport for these athletes.
The Wrist
Wrist injuries in high-level baseball players are both acute and chronic in nature. Common mechanisms of injury include diving, sliding, swinging during batting, and collisions. Wrist injuries account for 28% of overall injuries of the hand and wrist; however, the frequency of surgery is reported to be higher for wrist injuries than hand injuries (13.7% vs 4.5%; P < .001). The most common injuries in the wrist include sprains, contusions, hook of hamate fractures, extensor tendinopathy, as well as triangular fibrocartilage complex (TFCC) tears. In this section, we discuss hook of hamate fractures, extensor carpi ulnaris (ECU) tendon tendinopathy/subluxation, scapholunate instability, as well as TFCC tears.
Hook of hamate fractures
Hook of hamate fractures comprise 11% of wrist injuries among baseball players, compared to a general incidence of 2% to 4% within the general population. , The hook of the hamate is a structure that extends radially and volarly to the hypothenar eminence, serving as an attachment point for the transverse carpal ligament, pisohamate ligament, flexor digiti minimi, and opponens digiti minimi. , The hook of the hamate is also the distal boundary of Guyon’s canal, containing the ulnar artery and nerve. , The deep motor branch of the ulnar nerve traverses around the hook. Hook of hamate fractures can be acute or chronic in nature, generally resulting from an impact from the ball hitting the baseball bat. In particular, the nondominant hand experiences a significant force at the end of the bat. Players who use the “palmar hamate grip,” holding the knob of the bat in the palm of the hand, are especially susceptible to hook of hamate fractures.
Athletes sustaining this injury may typically complain of pain located in the volar and ulnar aspect of the palm. Providers should note tenderness overlying the hook of the hamate, suggestive of fracture. In addition, associated symptoms may include loss of grip strength, loss of flexion of the ulnar 2 digits, or numbness in the ulnar 2 digits. These symptoms may signify associated injuries including compression of the motor branch of the ulnar nerve, entrapment/attrition of the ulnar 2 flexor digits, or ulnar artery thrombosis. , ,
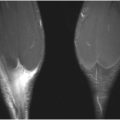
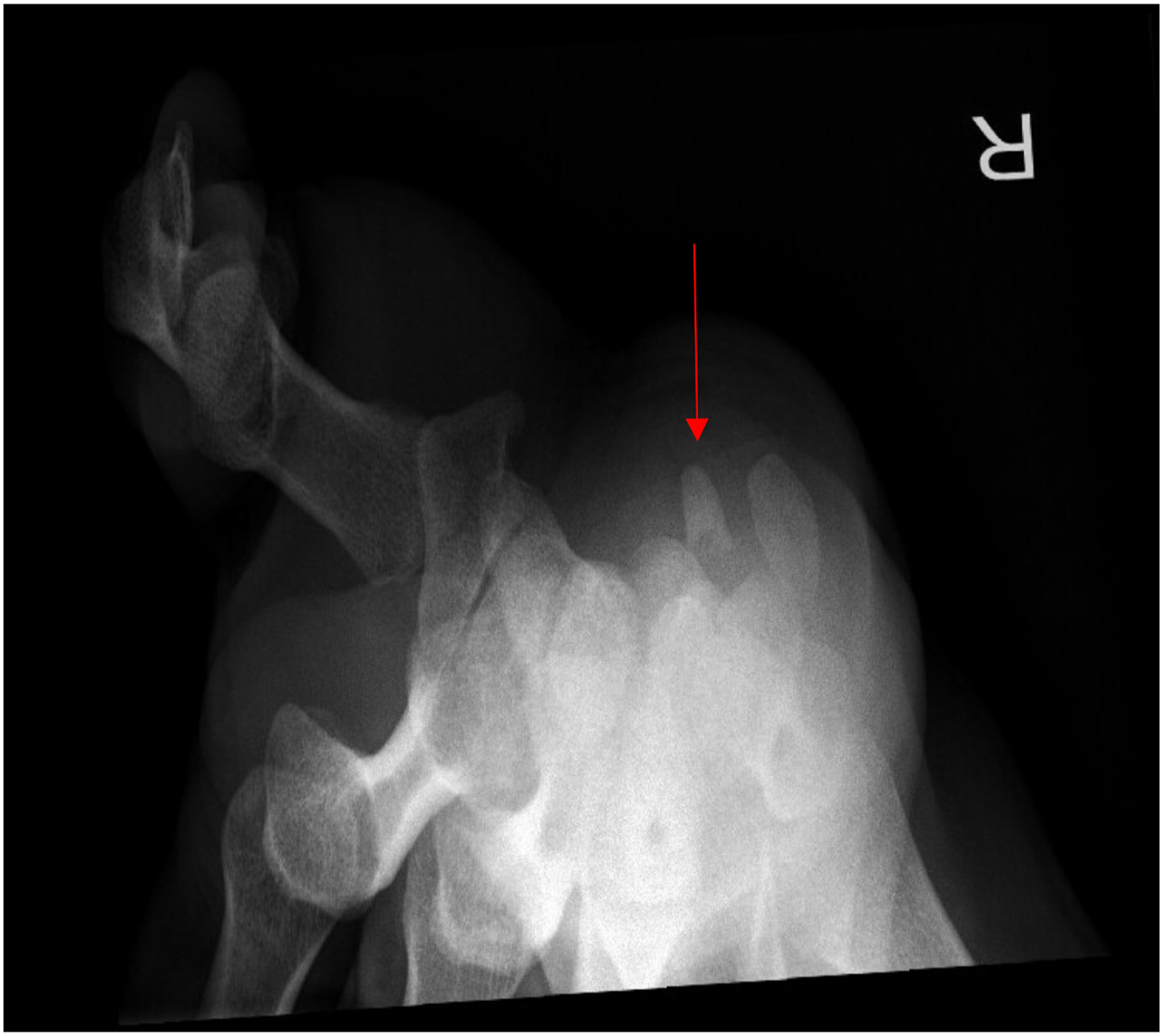
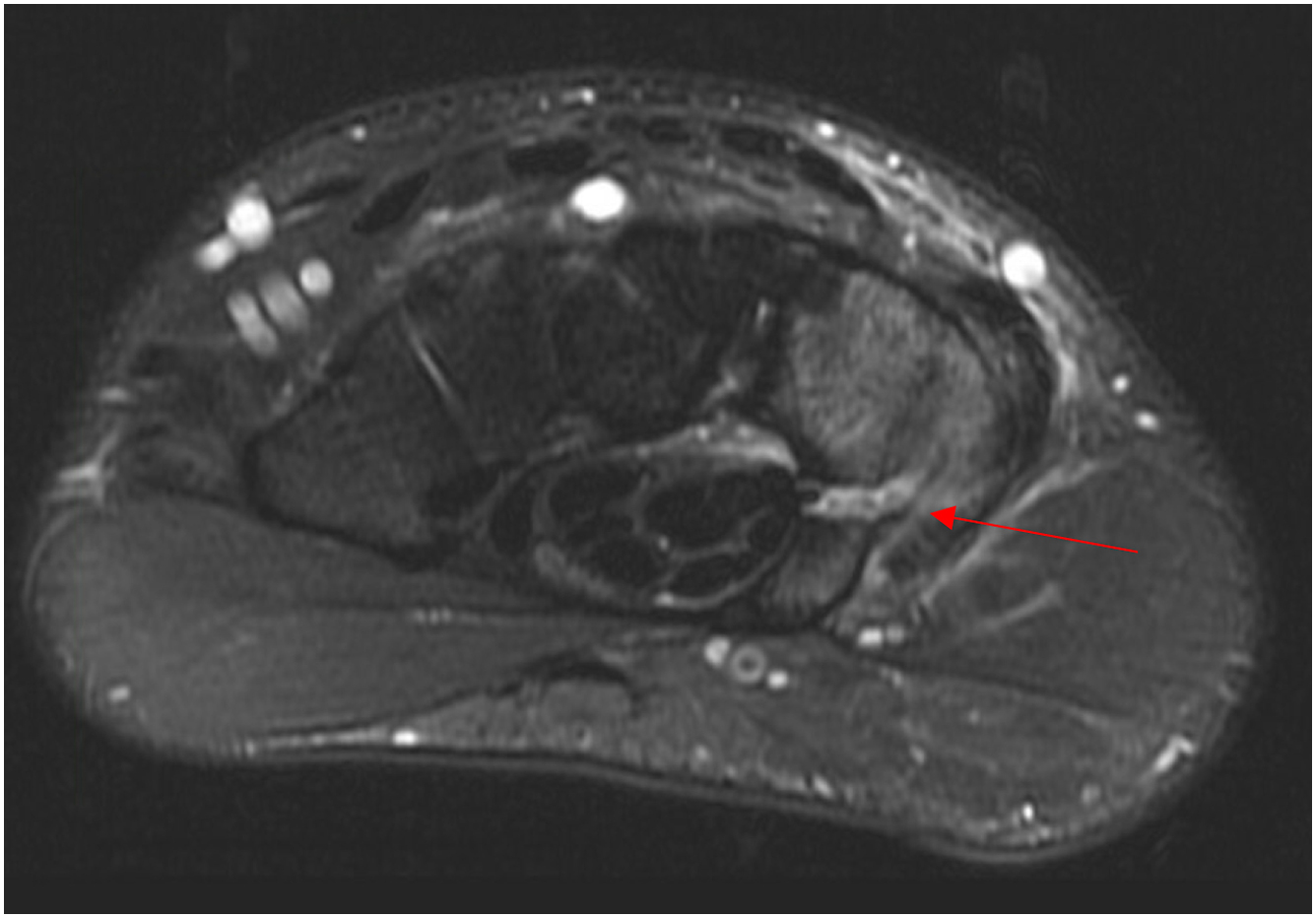
The hook of hamate pull test, described by Wright and colleagues, can be used to further increase the examiner’s suspicion for a hook of hamate fracture. The test is considered positive if pain is encountered with resisted flexion of the ring and small fingers with the wrist placed into ulnar deviation. Suspicion of this injury, however, should be confirmed with standard radiographs and advanced imaging. Posteroanterior (PA), lateral, and oblique views of the wrist may not reveal the fracture. Thus, a carpal tunnel view can be performed if tolerated by the athlete ( Fig. 1 ). The gold standard of diagnosis is the computed tomography, with an accuracy of 97.2% compared with 80.5% for pain radiographs (including all projectional planes). MRI can be used if neurovascular injury or flexor tendon injury is suspected ( Fig. 2 ).
Treatment options range from nonoperative to operative. For athletes with acute nondisplaced fractures, favorable healing has been demonstrated with immobilization in a short arm cast for 6 weeks. This may not be adequate in the high-level baseball player, who may not be able to risk nonunion due to the demands of the competitive season. Described surgical options include open reduction and internal fixation versus hook of hamate excision. The gold standard of treatment remains hook of hamate excision due to faster postoperative recovery. Concurrent neurolysis of the deep motor branch of the ulnar nerve can be performed; however, the surgeon should remain conscious of surrounding neurovascular structures to avoid injury.
Postoperative rehabilitation protocols following excision vary among surgeons. Patients are typically immobilized for 2 to 3 weeks to allow for wound healing and edema control. Range of motion is typically initiated following this time period with initiation of hitting at 5 to 6 weeks. , Athletes predictably return to preinjury level of play at around 7 weeks following surgery.
Scapholunate ligament injury
The scapholunate interosseous ligament (SLIL) is the primary stabilizer of the scapholunate interval. Injuries to the SLIL exist on a spectrum, ranging from partial to complete tears that may be either acute or chronic in nature. If not recognized and treated, SLIL injuries can result in a dorsal intercalated segment instability deformity, progressive carpal collapse, and radiocarpal degeneration. In baseball players, SLIL injuries occur during collisions or when diving for a ball. During these activities, the SLIL is predisposed to injury when the wrist is in extension, ulnar deviation, and carpal supination.
Athletes with this injury typically present with dorsoradial wrist pain. In cases of instability, they may note a popping or clicking sensation with wrist motion. On physical examination, swelling, reduced grip strength, and limited range of motion may occur. The Watson scaphoid shift test can be used to obtain a clinical diagnosis of SLIL instability, performed by placing a dorsally directed force on the scaphoid tubercle while bringing the wrist from ulnar deviation and slight extension to radial deviation and slight flexion. An appreciable “clunk” indicates a positive test; however, this should be compared to the contralateral wrist as a false-positive result may occur.
Initial imaging should include the standard 3 views as well as clenched fist radiographs. Contralateral radiographs may be useful for comparison. On initial plain films, widening of the scapholunate interval may be appreciated with possible increased scaphoid flexion and lunate extension on the lateral view. A “cortical ring” sign may be noted on the anteroposterior (AP) radiograph, as the scaphoid is superimposed on itself due to flexion. MRI is also useful in diagnosis and localization of injury, with a 3 T coil supplying the highest sensitivity and specificity.
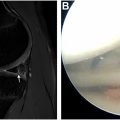
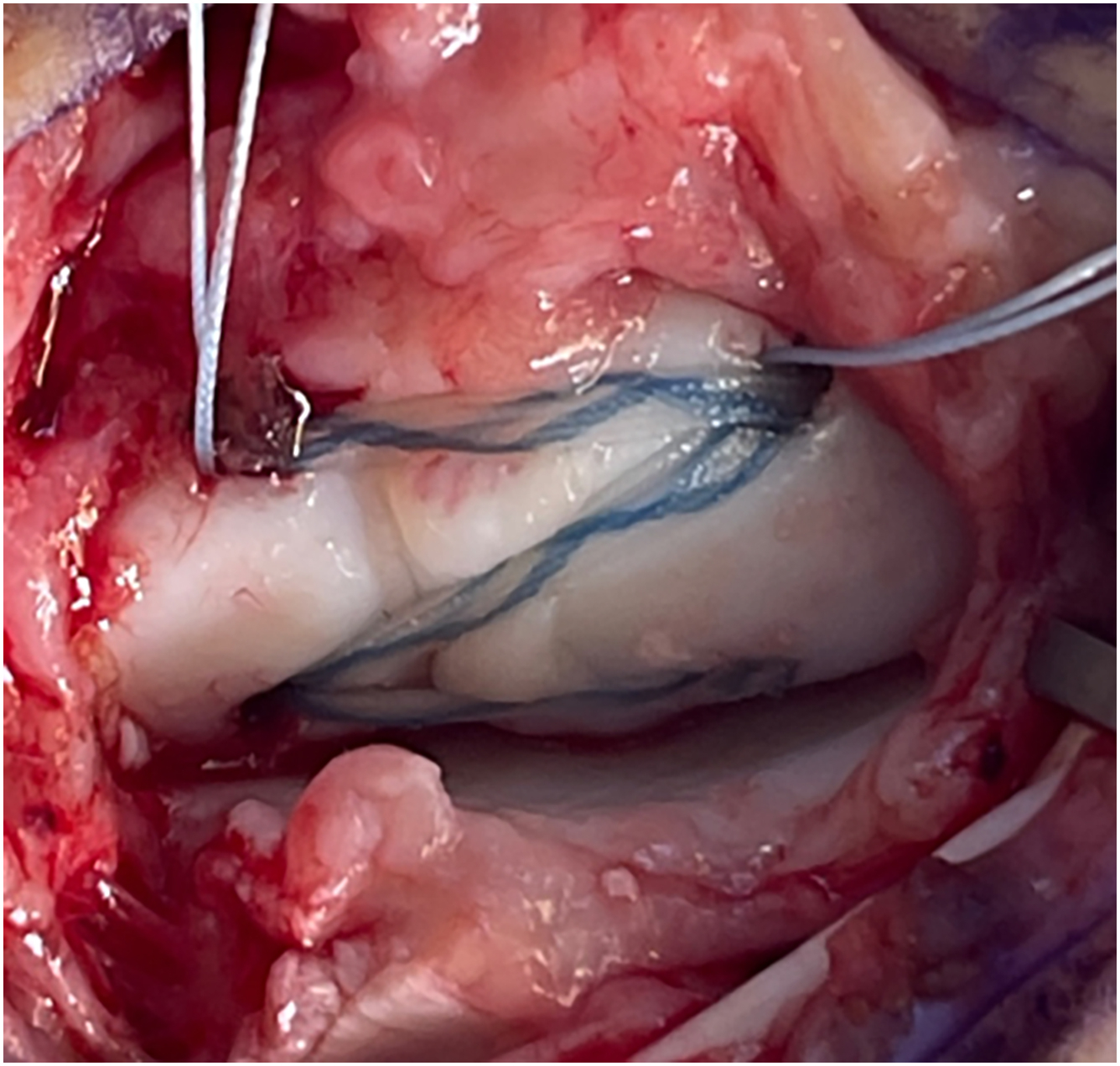
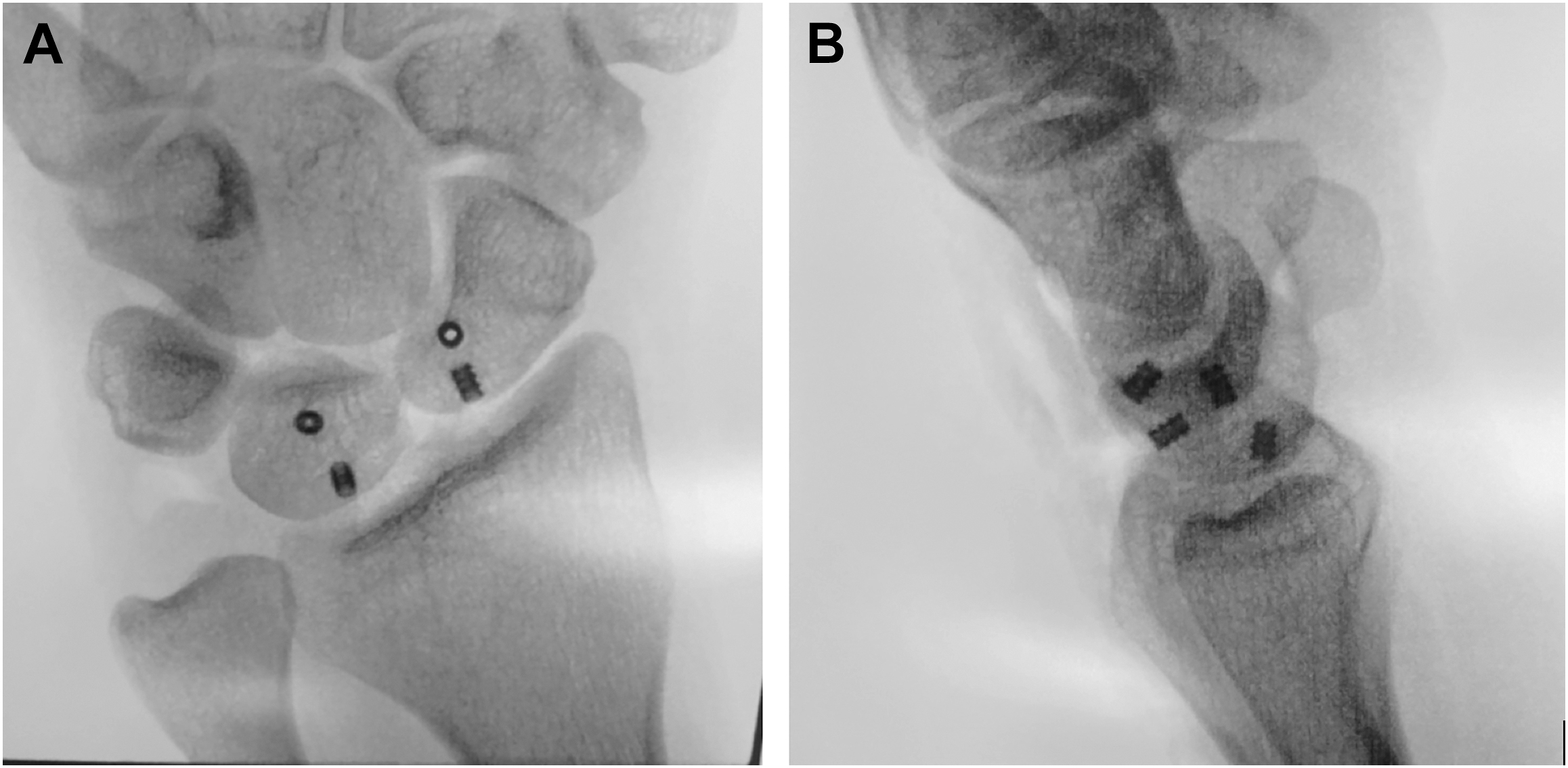
Numerous treatment options for SLIL injuries have been described and are guided by the degree (partial vs complete) and chronicity of injury. Partial tears are initially treated with a period of immobilization, anti-inflammatory medications, and/or cortisone injections. Those who continue to have symptoms may undergo arthroscopic evaluation with possible debridement and thermal shrinkage. For complete tears, open repair or reconstruction may be considered. Though many techniques for this have been described, our preference is internal brace reconstruction with dorsal capsulodesis ( Figs. 3 and 4 A, B ).
Postoperatively, athletes who undergo SLIL reconstruction with capsulodesis are immobilized for 4 weeks in a molded wrist brace with the thumb and fingers free. Range of motion is initiated at 4 weeks and strengthening is initiated at 6 weeks postoperatively. Sport-specific activities begin at 12 weeks postoperatively with the goal of return to play at 4 to 6 months.
Extensor carpi ulnaris tendinopathy/instability
The ECU tendon may be a common source of ulnar-sided wrist pain for the baseball player. Conditions associated with this tendon include tendinopathy, tenosynovitis, and instability (ie, tendon subluxation). The mechanism of injury typically results from the wrist being held in supination, flexion, and ulnar deviation during batting.
Diagnosis of ECU tendon disorders can be difficult clinically due to the “black box” of ulnar-sided wrist pathologies. Providers should remain cognizant of other possible diagnoses including TFCC tears or disruption of the distal radioulnar joint (DRUJ). On physical examination, dislocation of the ECU tendon may be noted when the wrist is taken through passive and/or active range of motion. Athletes may also experience pain when the wrist is placed in extension and ulnar deviation, particularly with the forearm in supination. Physical examination maneuvers may entail the ECU synergy test or ice cream scoop test. A positive ECU synergy test is noted when the patient demonstrates pain in the ECU tendon with resisted thumb abduction. The “ice cream scoop” test is performed with a scooping motion performed after the patient holds his or her wrist in pronation, ulnar deviation, and extension. With a positive test, the examiner will appreciate subluxation or dislocation of the ECU tendon upon palpation.
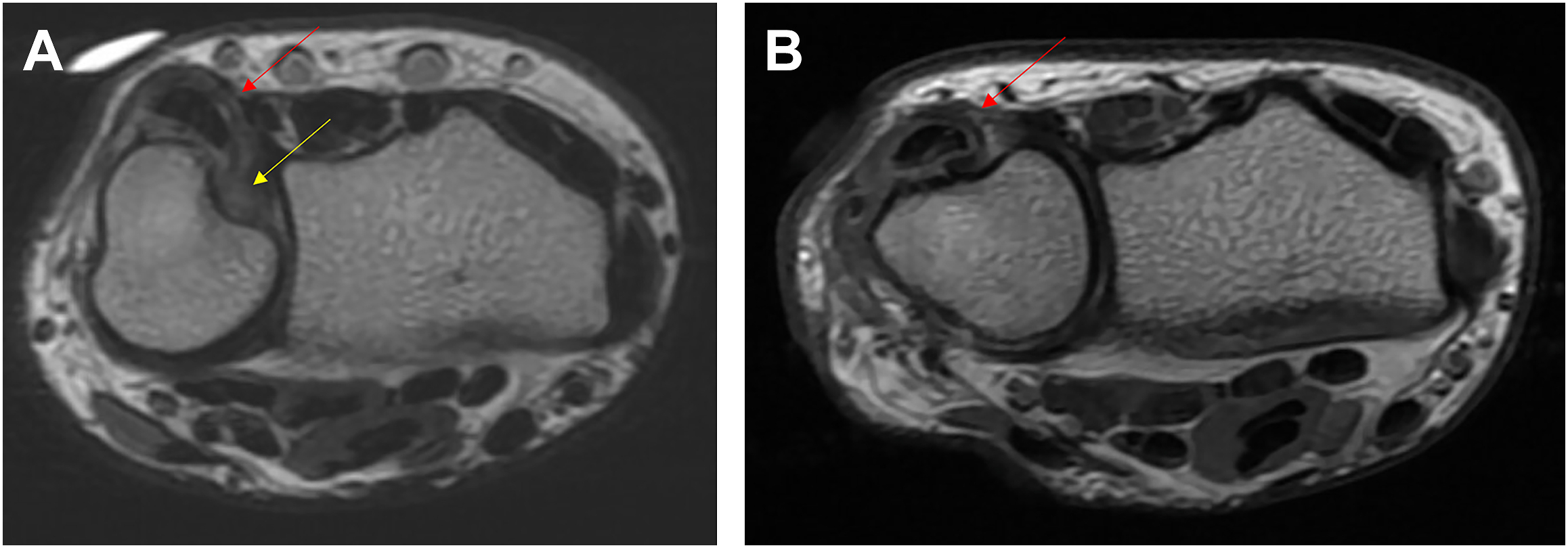
Dynamic evaluation of the ECU tendon may be performed using ultrasound. However, areas of tenosynovitis, tendinopathy, and position of the tendon within the ECU tendon groove may be evaluated on MRI ( Fig. 5 A ). MRI may also help differentiate ECU pathology from other diagnoses. Initial treatment of ECU pathologies may include rest, avoidance of aggravating activities, and immobilization. Immobilization may be performed for 4 to 6 weeks with the wrist in extension and radial deviation and the forearm in pronation to prevent tendon subluxation. Healing can be monitored periodically with MRI or ultrasound. For patients with recalcitrant pain or instability, surgical intervention can be considered. Surgical procedures range from tendon debridement, ECU subsheath repair, to ECU subsheath reconstruction ( Figs. 5 B; 6 ). Postoperatively, patients may undergo a short period of immobilization for tendon debridement procedures, or for a longer period (ie, 4–6 weeks) in extension, radial deviation, and pronation for cases of instability. Athletes may then initiate therapy for range of motion and strengthening, with return to play considered no earlier than 3 to 4 months postoperatively.

Triangular fibrocartilage complex injuries
In order to perform the swinging and throwing motions required by high-level baseball players, pain-free motion is critical. As mentioned earlier, ulnar-sided wrist pain can be challenging to diagnose and treat. Another source of pain is the TFCC, which must withstand transmitted loads through the ulnocarpal joint during these motions. Of note, the TFCC absorbs roughly 20% of the load at the wrist, which could be increased in athletes with ulnar-positive variance. The TFCC is composed of an articular disc, meniscus homologue, ulnocarpal ligament, dorsal and volar radioulnar ligaments, and the ECU subsheath. The TFCC receives its blood supply from the ulnar artery from the volar, dorsal, and ulnar aspects. Mechanism of injury during gameplay includes axial loading, ulnar deviation, and extremes of forearm rotation. TFCC tears may be acute or chronic in nature. Palmer initially characterized TFCC tears as being traumatic or degenerative, and later further classified these injuries based on their location.
Athletes with TFCC injury typically provide a history of ulnar-sided wrist pain that is worse with activity and may be associated with instability or loss of grip strength. The onset of pain may be pinpointed to one particular instance when the pain started. On physical examination, athletes may demonstrate foveal tenderness with palpation to this area. Provocative maneuvers described in the literature include the piano key test, ulnocarpal stress test, ulnar impaction test, and the TFCC grind test. These tests may be performed on the contralateral side for comparison.
Plain radiographs are important for initial imaging evaluation, as they allow for an assessment of ulnar variance, DRUJ congruity, as well as an ulnar styloid avulsion that could suggest an acute injury. Contralateral radiographs may be useful for comparison. Assessment of ulnar variance is typically performed on a PA radiograph with the forearm in neutral, shoulder in 90° of abduction, and elbow in 90° of flexion. MRI may also be performed for further assessment of the TFCC for central or peripheral tears, keeping in mind that 3 T MRI scans demonstrate greater sensitivity, specificity, and accuracy compared to 1.5 T MRI scans ( Fig. 7 ). Magnetic resonance arthrography (MRA) has also been increasingly utilized, as increased accuracy has been found in diagnosis of central and peripheral TFCC tears among patients receiving MRA versus MRI. The gold standard for diagnosis, however, is direct visualization and examination via arthroscopy.