- •
Wire subcision ensures complete release of retracted scars, deep lines, and folds.
- •
Release should be as close to the line or scar margin as possible.
- •
Hemostasis is extremely important to prevent prolonged swelling, ecchymosis, and protracted induration.
- •
Placement of filler, fat, or tissue graft is recommended to ensure long-term correction.
- •
The filler, fat, or graft should be used as a spacer with avoidance of overcorrection.
Introduction
Cosmetic surgery is marked by the great divide: open surgery on the one side and minimally invasive procedures, or rejuvenation, on the other. To accomplish rejuvenation, surgeons draw from a toolkit of procedures in order to resurface, refill, relax, and redrape. Very recently, another r-word has crossed the chasm from the open surgery side to minimally invasive. That word is ‘release’.
Dissection is fundamental to open surgery where it produces excellent results. But there is an associated cost: incisions that become scars and sometimes cause alopecia, considerable downtime, plus other side-effects that are common to any invasive procedure. In an attempt to achieve the results without the problems, surgeons have been querying various tools, hoping to find one that would deliver a minimally invasive form of release. For a while, forked cannulas and needles looked promising but experience indicated a failure to obtain complete subcision of deep lines, folds, depressions, and retracted scars. Certainly scissors do the job, but they require access incisions. Creating new scars to get rid of old ones does not make a lot of sense.
In 2000, a group of Russian physicians ( ) described another tool: use of a wire scalpel for subcutaneous dissection. After treating 54 patients for soft tissue contour defects, the Russians reported satisfactory or good results in 96.3% of patients at a mean follow-up date of 11 months. The first wire dissection tool consisted of a single needle attached to a short length of serrated wire which broke often and was cumbersome to use. In the quest for an ideal instrument, I helped Nutec International design the Diamond Wire and then consulted with Coapt Systems, Inc. on development of the SurgiWire, which I now use exclusively.
In 2006, I reported on my series of 45 patients undergoing wire release with a longest follow-up of 19 months and a mean follow-up of 12 months. From the 38 of the 45 patients who had wire subcision as opposed to seven patients where the wire was used as a flap dissection tool, the average improvement was two grades on the wrinkle rating scales. In the 24 months since that report, no patient has required repeat treatment of the released lines ( ).
The SurgiWire ( Figure 5.1 ) begins with 3 feet of wire (the length permits multi-pass usage on the same patient) braided from strands of 304-grade surgical stainless steel for strength and to minimize fraying. The wire has a slightly serrated edge to aid in tissue dissection. Two Keith needles are attached to opposing ends of the wire, permitting more flexibility than one needle for circumscribing difficult areas.
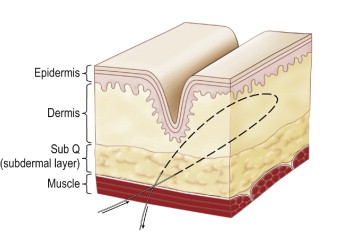
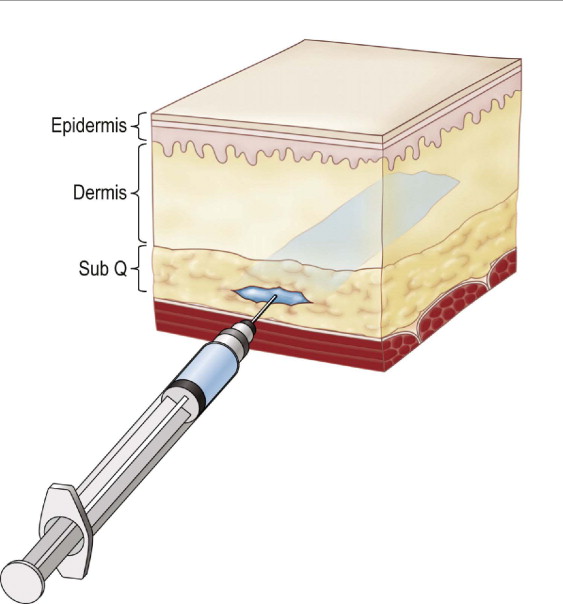
The SurgiWire saws smoothly and quickly through subcutaneous tissue, creating a consistent plane of dissection without a single incision. Risk is minimal, since motor nerves and larger vessels lie in deeper tissues. Upon releasing the subdermal plane beneath a wrinkle, the dermis flattens and the wrinkle relaxes ( Figures 5.2, 5.3 ).
However, successful results are contingent upon good technique. It is particularly important to:
- •
Release as close as possible to the line, fold, or depression being treated
- •
Insure hemostasis to avoid hematomas and prolonged swelling or edema
- •
Irrigate with 1% lidocaine with 1:100 000 epinephrine
- •
Hold pressure for 5 minutes following release
- •
Take care not to overcorrect when using fillers or fat.
Indications, patient selection and consultation
Wire subcision is indicated for patients with moderate-to-severe nasolabial folds, glabellar lines, acne scarring, post-surgical adhesions, and deep labiomental creases. It may also be used for marionette lines, periorbital lines (crow’s feet), radial lip lines, cheek and chin lines, transverse forehead lines, neck lines, and retracted scars. Cellulite is an emerging indication. Finally, the SurgiWire may be used for incisionless dissection to assist in a necklift.
The best candidate for wire release is a grade 4 or 5 nasolabial fold on the WSRS (on wrinkle severity rating scale, minimum wrinkling is a 1; maximum is 5) or a grade 4 or 5 nasolabial fold or other facial line on the Lemperle wrinkle assessment scale (a 0–5 point scale where 5 is the most severe). Patients with lower WSRS numbers are usually eliminated because they can be successfully treated with fillers.
With the WSRS, facial and neck lines, furrows, and folds from 11 different areas are compared against graded reference photographs. A grade of 0–5 is assigned to the wrinkle based on this comparison. Once again, grade 4 or 5 lines of the face and neck are the best indications for wire subcision. However, wire subcision in patients with lower WSRS grades may be indicated for: 1) glabellar lines and periorbital lines that are resistant to or poorly responsive to botulinum toxin and fillers; 2) deep radial lip lines that are resistant to or poorly responsive to botulinum toxin, filler, or ablation (laser, dermabrasion, deep chemical peel); or 3) patients with multiple lines of various depths already undergoing wire subcision for the more severe wrinkles.
The typical patient has invested a lot of money on fillers with poor results. Because lifting procedures do not resolve many of the indications described above, wire dissection is the logical recourse. Furthermore, it is affordable, can be done easily and quickly under local anesthesia in the office setting, and is effective with one treatment. In patients with grade 4 and 5 lines, the cost of wire dissection combined with fat or a filler is comparable or even less than the cost required for a single session using short or longer lasting fillers alone.
Additionally, in patients with grade 4 or 5 wrinkles, fillers alone often will not fill adequately under the deep attachment, instead bleeding out to the surrounding tissue, which accentuates rather than improves the line. Patients with such deep lines always require numerous treatment sessions with fillers and often with fat to adequately correct the line. Even after numerous filling sessions, unless a permanent filler has been used, the results are transitory. Wire subcision as opposed to fillers alone has the additional benefit that results appear to be long-lasting.
Another area where previous methods of correction have proved inadequate is in correction of post-surgical adhesions, especially in the face. These are occasionally seen after facelifts, especially in patients with SMAS modifications. Facial and neck liposuction can also leave contour irregularities. Depressions and abnormal adhesions may not be evident at rest, but can be quite prominent during facial animation. Wire subcision with a small amount of a filler or fat offers a simple and effective means of correcting these adhesions and depressions.
During a consultation visit, it is important to discuss the specifics of wire dissection and the need for a filler or fat as part of the procedure. If a patient is concerned about cost, the surgeon should emphasize that the primary function of filler is to serve as a spacer, reducing the rate of re-adhesion. As such, the volume requirements for the filler are much diminished. In fact, it is unlikely that more than 0.3 cc of a hyaluronic acid filler (Restylane®, Juvéderm® Ultra) per nasolabial fold will be used after release. The surgeon should inform the patient that it is possible that they may need another treatment sessions with filler or fat injection, but the volumes required would be small.
Secondly, advise the patient about follow-up visits at 1 week to monitor for adverse effects and at 4–8 weeks to evaluate the need for additional filler. If no adverse effects are present, the patient will return in 4–8 weeks to evaluate the efficacy of the treatment. At that time, more filler may be required. Finally, because the most common complaint about the procedure is prolonged swelling, it is important to alert patients to this possibility in advance, when discussing side-effects and obtaining informed consent. Doing so helps the patient mentally prepare for side-effects and accept them without undue anxiety.
A complete history must be taken as a routine part of consultation. Patients with a history of poor wound healing, immune compromise, hypertrophic scarring, or keloid scar formation are poor candidates for wire release. Those with a history of herpes simplex virus should not have any active lesions, and herpes prophylaxis in those patients should be started 2 days before the procedure and continued for 3 days after the procedure. On physical examination, patients with thin or fragile skin are not good candidates for the procedure.
Pre-operative preparation
Seven days prior to the procedure, patients should discontinue aspirin, ibuprofen, vitamin E, vitamin C and any other medication that may adversely affect the clotting pathway. The patient may resume taking these medications 1 day post procedure. SinEcch™, a homeopathic preparation of Arnica montana, may be started 24 h prior to the procedure to minimize bruising and swelling. SinEcch™ or other over the counter arnica preparations should be continued for 4 days after the procedure as per package instructions.
Wire dissection can be performed alone under local anesthesia or in conjunction with other procedures under general anesthesia. The advantage of the latter is that it facilitates the harvesting of fat for use as a spacer to prevent firm re-adhesion of the released line or fold. Performing the procedure under local anesthesia does not preclude the use of fat for grafting other than the additional time required for the procedure and the discomfort of the donor site. The patient is marked in the upright position with a surgical marker. The patient is marked in repose and then checked again with the patient smiling or wrinkling their brows and forehead to check the extent of the lines. Topical anesthetic (betacaine LA, triple anesthetic cream (BLT: 20% benzocaine, 6% lidocaine, 4% tetracaine) can be applied as well as ice to lessen the discomfort of the local anesthetic injection. Ten minutes prior to the procedure, 1% lidocaine with 1 : 100 000 epinephrine is injected as a local block in the area to be treated. Nerve blocks may also be performed to supplement the anesthesia for the procedure.
The overall goal is to create a plane of dissection that will undermine the defect. To accomplish this, markings should be as close as possible to the defect or wrinkle. See the ‘Variations by procedure’ subsection under ‘Operative technique’ below for more details.
Related posts:





Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


