Key points
- •
Our workhorse in minimally invasive facial rejuvenation is the MACS-lift (minimal access cranial suspension lift).
- •
A short-scar facelift is not the same as a traditional facelift with a short scar.
- •
In the neck as well as in the face the vertical vector is the rejuvenating one.
- •
Facelifting is not a tightening procedure, but a facial sculpturing technique with correct redraping of the skin. The sculpturing is obtained by suturing techniques, judicious liposculpture, volume addition by microfat grafting, or combinations of these.
- •
All vertical facelifting techniques require a temporal pre-hairline incision to avoid raising of the hairline.
- •
Avoid opening the neck if possible.
- •
Short-scar facelifting is not an absolute necessity: poor skin quality sometimes requires supplementary skin redraping in the retro-auricular region.
Patient selection
As facial rejuvenation surgery has grown in popularity, more women and men from all social and age categories are considering this possibility. In our practice, younger patients, starting in their early thirties, are consulting for preventive and corrective rejuvenation measures. The treatment array includes preventive skin care, botulinum toxin and fillers, and minimally invasive surgical procedures. The candidates for surgery are often unwilling to undergo aggressive and potentially risky procedures. They desire a subtle correction of the early signs of aging, and not a dramatic change often associated with a longer downtime. Older patients also welcome less aggressive but still effective rejuvenation procedures.
The decision whether to select a short-scar facelift or a more traditional type of incision depends partly on the extent of the neck deformity, but mainly on the quality of the skin. It is our conviction that most patients can be perfectly treated with a short-scar facelift, and that if the result in the neck is insufficient then minimally invasive ancillary maneuvers can be added for example, the anterior and posterior cervicoplasty (see ‘Pitfalls and how to correct’ below). This will result in an equally satisfying result but with a lesser morbidity and shorter recovery time.
Indications
The appeal of the minimal access cranial suspension (MACS) lift lies largely in that it offers a stable and natural facial rejuvenation using a simple and safe procedure of 2–2.5 h which can be performed under local anesthesia on an outpatient basis. In comparison to a classical facelift, the MACS-lift has a quicker recovery and a lower morbidity. The final scar is also significantly shorter.
The general principle of MACS-lift is the vertical suspension of sagged facial soft tissues with permanent or slowly resorbable purse-string sutures strongly anchored to deep temporal fascia through a pre-auricular and temporal pre-hairline incision.
Two variations of the procedure were designed:
- •
The simple MACS-lift (S-MACS): Where two purse string sutures are placed for correction of the neck and the lower third of the face (cervico-mental angle, jowling, marionette grooves).
- •
The extended MACS-lift (X-MACS): Where a supplementary third purse string suture is placed to suspend the malar fat pad. This suture will have an extra effect on the nasolabial groove, the midface and the lower eyelid.
Simple MACS-lift
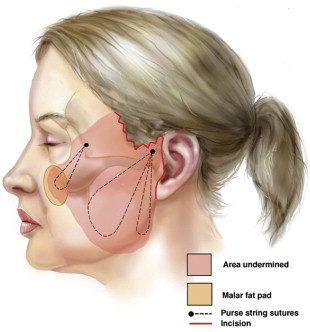
Two purse string sutures are used for correction of the neck, the jowls and the marionette grooves. They are both anchored to the deep temporal fascia above the zygomatic arch 1 cm in front of the auricular helix. The first suture runs as a narrow vertical U-shaped purse string to the region of the mandibular angle catching the lateral border of the platysma muscle. Tying this suture under maximal tension produces a strong vertical pull on the lateral part of the platysma muscle, correcting the cervicomental angle of the neck region, which has been liposuctioned previously. The second purse string suture starts from the same anchoring point above the zygomatic arch and runs obliquely in the direction of the jowls as a wider O-shaped loop. This suture corrects the jowls, the marionette grooves and the downward slanting of the corners of the mouth ( Figure 9.1 ).
Extended MACS-lift
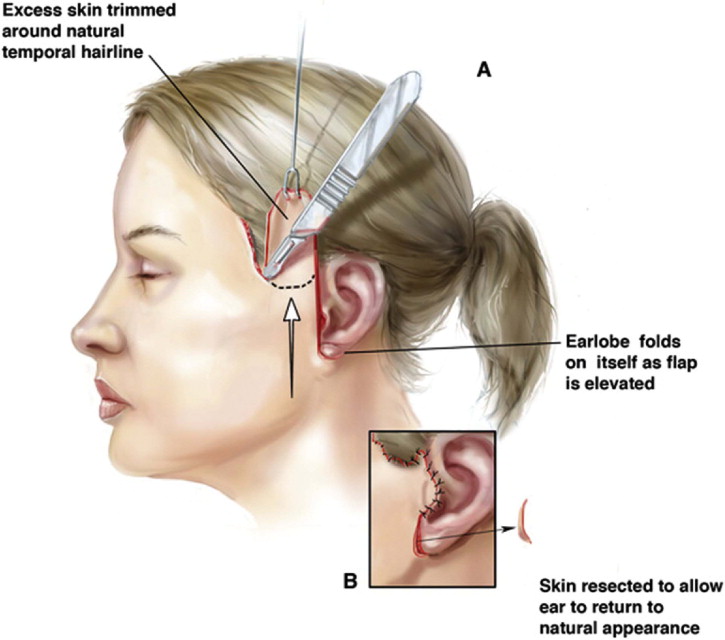
When performing an extended MACS-lift, an additional undermining of the skin over the malar region is performed. A point dropped 2 cm below the lateral canthus has been marked with the patient in the standing position. It will be included in the skin undermining and is the inferior limit of the third purse string suture. This suture originates as well from the deep temporal fascia, but in its anterior part, lateral to the lateral orbital rim. It provides a strong correction of the nasolabial fold, an enhancement of the malar region, a lifting of the midface and a shortening of the vertical height of the lower eyelid ( Figure 9.1 ). In both S-MACS and X-MACS the skin is redraped in a pure vertical direction and the excess of skin above the temporal hairline incision is resected. As no lateral traction on the skin is carried out, there will be no dog ear at the level of the earlobe eliminating the need for a retro-auricular dissection ( Figure 9.2 ).
As a consequence of lifting the malar fat pad in the direction of the lateral orbital rim, a bunching up of skin in the region of the lateral part of the lower eyelid and the paracanthal zone becomes apparent. A skin excision in the subciliary and paracanthal region hence becomes mandatory. This pure skin resection is easy and safe because of the good structural support of the lower eyelid provided by the third purse string suspension suture. This observation has led to the development of the principle of pinch blepharoplasty: the excess of skin is evaluated by pinching the skin between the teeth of a forceps and excised via a lower eyelid blepharoplasty incision with paracanthal extension. Four to eight mm of skin can easily be resected especially in the paracanthal region without the risk of ectropion or scleral show. The MACS-lift provides a powerful correction of submental and upper neck laxity, correction of a blunted submental angle, restoration of a well defined jaw line by correction of the jowls, restoration of the mid facial volume and correction of the nasolabial fold.
The decision whether to perform a simple or extended MACS-lift is not purely determined by the age of the patient. The main consideration is whether the patient needs a correction of the upper half of the nasolabial fold and the midface. The third suture, suspending the malar fat pad, gives a powerful correction of these features. It also enhances the volumetric restoration of the midface and provides a very strong support of the lower eyelid skin. This means that the indication for the third suture can be extended to patients with a flattened malar mound and laxity of the lower eyelids. This is not only determined by age, but also by the facial bony anatomy.
In classical teaching, smoking is considered an absolute contra-indication for facelift surgery. Because of the limited subcutaneous undermining and the absence of multiplanar dissection we consider smoking more as a relative contra-indication. As a general rule, only patients without a major medical history or cardiovascular risk factors are selected for outpatient office-based surgery. The decision whether to perform the MACS-lift under local or general anesthesia depends on the surgeon’s and the patient’s preference.
Operative technique
Pre-operative relaxation
Before prepping and draping, we give an intramuscular injection of 2.5–5 mg of midazolam (Dormicum®, Versed®) according to the body weight and the anxiety level of the patient.
Pre-operative marking
With the patient in the sitting position, we ask them to make a double chin and this area including the lower part of the jowls is marked and will be liposuctioned. When an extended MACS is performed, a point ±2 cm below the lateral canthus is marked. This point will be included in the skin undermining.
Infiltration
The sequence of infiltrations follows the sequence of the procedures. This is, firstly the upper eyelids if treated, followed by the submental area, and then by one cheek infiltration (for the anesthetic solution, see Box 9.1 ) . For the submental suction lipectomy an average of 30–40 cc is infiltrated in the preplatysmal fat until a moderate degree of tumescence is reached.
Pre-operative marking: incision
We start the marking at the lower limit of the lobule, going up in the pre-auricular crease. At the level of the incisura intertragica the marking makes a 90° turn backwards to preserve the integrity of this anatomical landmark. The marking then follows the posterior edge of the tragus, ascending towards the helical root ( Figure 9.1 red line).
At the superior limit of the ear, the marking follows the small hairless recess between the sideburn and the auricle and then turns downward to follow the inferior implantation of the sideburn. In males the marking descends approximately 1.5 cm before turning anteriorly to cross the sideburn.
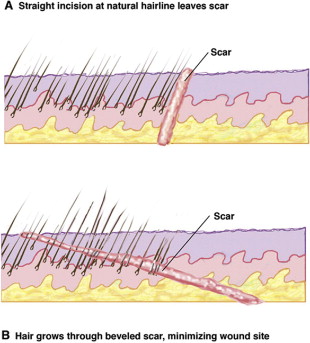
The marking runs further forward in a zigzag pattern, 2 mm within the lower and anterior implantation of the sideburn. In this part of the incision, the knife is inclined to an angle almost tangential with the skin as to cut hair shafts perpendicularly ( Figure 9.3 ) . This manoeuvre will allow hair to grow through the scar. After hair regrowth the final scar will be hidden a few millimeters within the hairline and become virtually invisible. The purpose of the zigzag pattern is to increase the length of the temporal incision for better congruence with the length of the cheek flap thereby reducing dog ear formation. In the simple MACS-lift the incision will extend to the level of the lateral canthus. In an extended MACS-lift the incision goes up to the level of the tail of the eyebrow.
Pre-operative marking: undermining
We palpate the mandibular angle with the index finger and mark this as the lowest point of the undermining. We mark the extent of the undermining starting from the lowest point of the incision at the lobule, directed towards the marking of the mandibular angle, and then curving anteriorly to 5–6 cm in front of the ear. In the case of an extended MACS-lift, we include the undermining of the malar eminence in the demarcation ( Figure 1 pink).
Suction lipectomy
We prefer to use a 3 mm spatula cannula with one opening. The opening is never directed towards the skin to avoid dermal damage. Two or three stab incisions are used to criss cross the marked area optimally. The lipectomy is performed in a preplatysmal plane under tactile guidance of the non-dominant hand. A maximal lipectomy is performed, so that the cannula is visible just beneath the skin. Exceptionally, pre- and/or subplatysmal fat needs to be directly excised as an open lipectomy through a 3 cm submental incision with wide undermining of the neck skin for redrapement.
In cases where a microfat grafting is planned, the submental fat can be harvested with a special grafting cannula ( Figure 9.4 ) which delivers fine-particle fat (1 mm diameter). If insufficient donor fat is present in the submental, area fat is harvested from the abdomen or lovehandles, using other microfat harvesting cannulas ( Figure 9.5 ).